
Abstract
The study's objective is to describe how individuals accessing a virtual crisis stabilization program following discharge from an emergency mental health visit perceived the service as either facilitating or hindering recovery. Interested service users were identified through feedback surveys and contacted for an interview. Demographic and service utilization variables were obtained from the survey data. Interview data were analyzed thematically using an inductive approach focused on exploring perspectives related to recovery. Twenty-one participants were interviewed; one with a support person. Four recovery thematic categories were identified: (1) connection to others is possible or lacking; (2) access to care providers/therapeutic relationship; (3) ability to remain at home; and (4) virtual service provision. Each category generated subthemes that demonstrated both positive and negative impacts of the virtual service. Lived experience highlights typical aspects of crisis intervention, as well as unique themes related to the home environment and virtual care option. It is important to identify these contextual factors when determining if virtual care is right for an individual. Some areas for service improvement were also highlighted.
Introduction
The United States's National Alliance on Mental Illness defines a mental health crisis as “any situation in which a person's behavior puts them at risk of hurting themselves or others and/or prevents them from being able to care for themselves or function effectively in the community.” 1 Often this represents a phase in the cyclical nature of mental illness; the crisis occurs, the individual deteriorates from baseline, followed by crisis intervention and recovery, and return to baseline. 2 Common precipitants include trauma, stressful life events, and social withdrawal or exclusion. 3 The crisis intervention phase is critical to prevent loss of functioning and support recovery back to baseline. 2 Individuals in crisis often present at emergency departments (EDs) with self-harm, suicidal ideation or attempt, depression, and psychosis.4,5 Furthermore, this crisis presentation is frequently the first point of contact with mental health services. 6
Hospital admission has historically been the first-line management strategy for individuals experiencing acute psychiatric deterioration.2,7 Hospital care has the benefit of close monitoring, psychiatric evaluation, medication access, and mitigation of risk behaviours, 4 with potential harms such as violence or harassment from co-patients, privacy breaches, stigmatization, social isolation, and boredom.4,8,9 Furthermore, the experience of compulsory institutionalization can be traumatic for service users and represents a frequently cited fear and care-seeking barrier.10,11 While inpatient services continue to be vital, 4 it is not ideal for every patient, and is not always necessary for successful crisis management in certain cases. 9
Alternatives to inpatient admission include crisis resolution teams (CRTs), partial hospitalization programs, low-acuity community residential alternatives, and various community services.4,9,12,13 In recent years, virtual crisis management, where a team offers remote support via virtual communication tools, has increasingly become an option.14,15 Some identified challenges include privacy and security factors, concerns over the therapeutic relationship, and technological barriers. 16 However, the virtual modality offers many benefits that make it a desirable option, including convenience and comfort,16,17 as well as reducing possible stigmatization that is associated with inpatient services. 18
Crisis stabilization is a complex and dynamic process that is different for every individual.19,20 The different types of crisis management services each have the potential to facilitate or impede recovery, 4 and thus an understanding of how and when each type of crisis service impacts recovery is essential. As they are newer, there has been little research investigating how virtual crisis services impact this process. This study aimed to describe how patients who received care at a virtual crisis stabilization unit (CSU) and their support persons perceived the impact of the virtual program on recovery, and specific characteristics of the service that impeded or facilitated the journey. The study findings can inform how this modality of support fits within the spectrum of crisis management services.
Methods
Study Design and Setting
We carried out a qualitative description study of patients’ experience with a virtual form of the CSU in a large urban center in central Canada. Qualitative descriptive methodology 21 is common in healthcare research and is especially appropriate for describing participants’ experiences and perceptions.22,23 While qualitative description does not subscribe to a particular theoretical orientation, it is guided by certain basic assumptions, most notably that reality is subjective, data are analyzed inductively, and an emic stance is adopted by researchers. 24 Research ethics for this study was obtained from the Health Research Ethics Board (HS25298(H2021:435)).
The CSU is a subacute voluntary in-person unit that supports individuals in crisis who do not require hospitalization. In 2020, the CSU launched a virtual alternative (vCSU) in response to the COVID-19 restrictions, which has since remained open and expanded. 14 Individuals are referred from all EDs and urgent care centers in the city, including a 24-hour walk-in mental health crisis center. At both the CSU and the vCSU, service users have access to a multidisciplinary team of mental health professionals, as well as group psychoeducation sessions, psychiatric consultation, medication support, and connection to community mental health and addiction resources. 14 The vCSU operates 7 days a week during daytime hours through a combination of virtual means including telephone, video-conferencing, and email or SMS communication. After-hours support is available through an affiliated crisis helpline.
Data Collection
All individuals who were admitted to the vCSU or CSU between March 2022 and May 2023 were invited following discharge to complete a web-based survey on their experience. The survey was accessible via an email sent by the clinical team or via a link/QR code posted on the in-person unit. The survey collected demographic data on prior crisis admissions (in-person or virtual), age, gender, and ethnicity and contained questions relating to satisfaction with the service they utilized.
The research team contacted willing survey respondents who had any contact with the virtual program to be interviewed. Those who agreed were contacted to obtain informed consent. Interviewees had the option of being interviewed with a support person of their choice who provided further insight into the patient's experience. Interviews were conducted virtually over Zoom or telephone, and utilized a semistructured interview guide consisting of questions which explored personal experiences of receiving crisis care virtually (see Figure 1). Interviewees received a $25 e-gift card for participating.

Sequence of interview topics.
All interviews were audio recorded using Zoom or a hand-held, digital voice recorder. The audio files were transcribed verbatim from an outside transcription service. The verified and deidentified transcripts were uploaded to NVivo 12.
Data Analysis
Demographic data collected in the survey were analyzed descriptively. The researchers employed thematic analysis for the interview data to generate a qualitative account of the data that was nuanced and in-depth. 25 To further qualify and understand the sample, indicators for additional interviewee characteristics were derived from the interview data including reason(s) for coming to care, employment status, relationship status, living situation, and parental status. The qualitative analysis process began with 2 researchers (A1 and A5) independently coding the first 5 transcripts and meeting to compare initial themes. After reaching agreement, a codebook was generated and shared to guide the coding of subsequent transcripts. The remainder of the transcripts were then split between the 2 coders who continued to meet periodically to discuss themes and definitions and the codebook was revised and updated as needed. After the analysis of 10 transcripts, theoretical sampling, the selection of participants based on certain characteristics, was employed in an effort to fully develop emergent themes. 26 Recruitment of participants continued until it was determined that theoretical saturation was reached as no new themes were emerging from the data 27 and the benchmark average of 12 to 13 interviews for achieving saturation was surpassed. 28 Once the codebook was finalized, the research team reviewed to consolidate the codes into categories aligned with broader themes related to recovery in the context of virtual crisis intervention. Throughout, the researchers exercised reflexivity by engaging in memo writing in an effort to identify subjectivity in order to clarify researcher bias and its influence on data interpretation. 29
Results
This study aimed to describe the ways in which the vCSU impacted patient recovery. Twenty-six survey respondents agreed to be contacted for an interview. From those, 21 agreed to participate in interviews. One of the 21 interviews included a support person. Interviews ranged from 23 to 89 min in duration.
Participants’ Characteristics
Demographic and service utilization variables of service users are summarized in Table 1. There were high rates of prior crisis service use, with a third or more having in-person CSU admissions or psychiatric hospital admissions. The average age was 38.2 years, and the majority of participants identified as a woman (76.2%) and of white ethnicity (85.7%). The most common reason for coming to care was worsening symptoms, followed by experiencing a stressful life event or trauma. Most commonly, participants were employed or enrolled in school, and living alone with no children.
Characteristics of Interview Participants, N = 21.
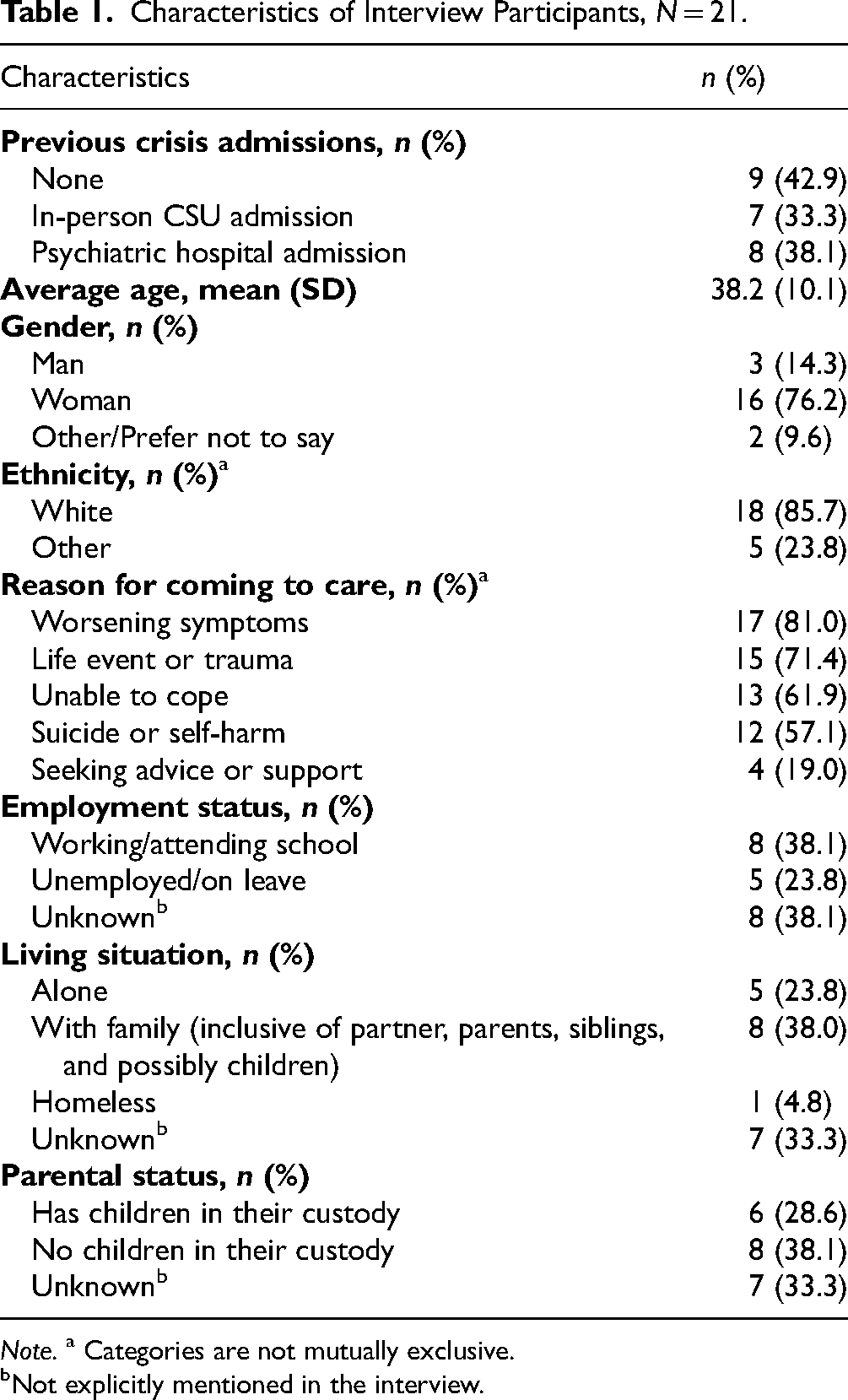
Note. a Categories are not mutually exclusive.
Not explicitly mentioned in the interview.
Four thematic categories related to the impact that the virtual program had on crisis resolution and recovery were created, each with subthemes. These were Connection to others is possible or lacking; Access to care and building therapeutic relationships; Ability to remain at home; and Virtual service provision (see Table 2).
Themes Relating to Crisis Resolution and Recovery, Separated Into Those Being a Facilitator and Those That Were a Potential Barrier.

Connection to Others is Possible or Lacking
Connection was a category often reflected in the participants’ recovery journeys. Participant narratives discussed how the virtual service either aided or hindered the service user's ability to form and maintain connections that were helpful in their crisis resolution. There were 4 themes, 3 of which indicated a positive effect on connection: (1) connection to others through group sessions, (2) involvement of natural supports, and (3) access to regular care providers and prescribers. For example, one participant noted that being part of group sessions provided a feeling of connection: “Because you get the connection of like, oh, yeah, there are other people in this virtual program, right? There are other people who are at home in a bad place just like I am” (P.4). The one negative theme was (1) feeling disconnected from others in group sessions, illustrated by a participant's experience of the virtual group sessions being less personal: “Whereas you can’t really do that with the virtual, I found that a lot of people don’t really want to talk in the virtual one” (P.10).
Access to Care and Building Therapeutic Relationships
This category captures how the virtual service either impacted a patient's ability to access and form a helpful therapeutic relationship with mental health professionals and how that related to recovery. Five positive themes include (1) check-ins, (2) relationship building with the clinician is present, (3) staff qualities, (4) talking about difficult topics, and (5) starting point for recovery. The value of brief check-ins with a mental health professional was identified by many participants such as one who stated, “I think that it is a really good resource to have and some people all they need is someone just to check in on them and that's good enough to help you through a crisis sometimes” (P.5). The continuity of daily support with the same clinician was also seen as important: “I really started to notice like that connection starting to build. It was just picking up where we left off the following day…” (P.15). One negative theme was (1) relationship building with the clinician is absent, where staffing changes or a perception that interactions were superficial made the participant feel that connection was absent.
Ability to Remain at Home
Access to the home environment with virtual support was discussed by participants as it related to their ability to engage in recovery. Five positive themes in this category include (1) access to personal comforts, (2) coping in a natural environment, (3) continuation of responsibilities and obligations, (4) managing co-occurring health needs, and (5) avoidance of inpatient triggers, which divided into (5a) avoidance of socioenvironmental triggers, and (5b) avoidance of COVID-19 triggers as this study assessed service use during parts of the pandemic. Access to personal comforts was discussed by many participants, including their own bed, pets and other coping objects. Many participants talked about having a sense of control over their environment as comforting. Three negative themes include (1) less engaged or committed, (2) limited structure or socialization, and (3) community triggers. For some, being at home reinforced more avoidance: “it's easier not to go sometimes when it's virtual” (P.1), and continued exposure to potentially unhelpful triggers in community such as substances.
Virtual Service Provision
This final category details the specific aspects of a virtual modality that either helped or hindered crisis resolution. Four themes were positive: (1) viable alternative to in-person services, (2) convenience, (3) decreased wait times, (4) and personalized resources. Many found that the service came close to providing what an in-person program would do: “it was about as close to in person therapy as I could have asked for” (P.15). The convenience meant that participants could balance other demands like work or school and still receive needed support. Additionally, 4 negative themes include (1) unpredictability or uncertainty of the service, (2) technological barriers, (3) contact availability was insufficient, and (4) form of contact was not adequate. Contact availability further divided into (3a) requiring more regular contact or check-ins, and (3b) after hours support was lacking. Form of contact generated 3 subthemes: (4a) lack of options for care contacts, (4b) contacts were too brief, and (4c) lack of visual cues over the phone. Many of these themes related to the majority of contact being done by phone and the limitations felt with that.
Discussion
This study explored how patient recovery was impacted by virtual crisis stabilization support from the perspective of patients and their support persons. The results illustrate how users of the vCSU felt the service contributed to their crisis resolution and the various positive and negative impacts of the program. In addition to the essential components of crisis resolution like support, therapeutic relationships, and connections to resources, additional positive and negative themes arose. This highlights that while virtual services may be helpful for certain people, individual characteristics and contextual factors make it less suitable for others. This is consistent with the notion that recovery is complex19,20,30 and that different crisis services have varying efficacy for different individuals. 19 Findings from this study also highlight areas for optimization in the delivery of virtual crisis care.
Recovery-oriented services are those services that function to facilitate a patient-centered view of recovery, rather than solely focusing on symptom resolution.19,31 Some aspects of the virtual service promote patient self-management and align with recovery-oriented principles such as promoting a “starting point for recovery,” “connection to others,” and “coping in one's natural environment.” These findings are in-line with previous research on CRTs, which have been widely implemented throughout Europe. 12 Like the vCSU, CRTs generally consist of a multidisciplinary team of mental health professionals who aim to deliver intensive mental health care to individuals who would otherwise require inpatient hospitalization. 12 CRTs, through in-person home-based support, were designed to reduce the harms and stigmatization associated with inpatient admission, and the notion that coping skills are more likely to be effectively applied if they are being used in the same context in which they are taught. 12 Not surprisingly, the strengths outlined by the CRT model32–34 are consistent with the vCSU model which strives to achieve the same benefits through entirely remote support. Similar to the findings in this study, CRTs have been shown to have lower satisfaction and efficacy rates when there are inconsistent or infrequent home visits, and when patients do not feel they have the intensity of support that they require.32,33
This study also identifies potential hindrances to crisis resolution with the virtual model. For some individuals, this model may perpetuate underlying patterns of avoidance or maladaptive coping that is preventing them from achieving meaningful recovery. Previous research has similarly explored the potential for a diminished therapeutic relationship4,35,36 and concerns with the limitations of virtual care.4,16,36 Ultimately, these findings emphasize the important notion that crisis intervention needs to be individualized. 16
Strengths and Limitations
Although theoretical saturation was achieved and the sample was representative of the typical CSU users, 37 the sample lacked representation of the older patient demographic. Additionally, there may have been selection bias in that interview participants only consisted of individuals who were agreeable to utilize virtual services in the first place. A large number of participants had experience with both virtual and in-person services, which allowed some comparisons. Interview participants utilized the vCSU when it was still fairly new; some aspects of the service that were identified as hindering or inadequate could be improved with service enhancements. Additionally, the effects of the COVID-19 pandemic (although improving at the time of this study) may have continued to have an impact on service users’ attitudes toward virtual care. The use of videoconferencing for interviews allowed researchers to conveniently engage with participants in real-time, 38 and the ability to witness facial cues to help contextualize those responses. 39 Any barrier to using Zoom was mitigated by offering telephone or in-person interview options.
Conclusion
Overall, this study illustrates, for both service users and providers, how virtual crisis care can fit within available services. This study also highlights the feasibility and acceptability of this model of crisis stabilization support, and identifies some of the unique ways in which receiving help at home can facilitate one's recovery. Service users and providers who have access to this type of support can consider when and for whom this is a good option and where needed, be aware of the ways in which it could enhance or inhibit crisis resolution. Additionally, decision makers can consider the role of virtual crisis support in the local system as it seems to be a viable alternative to inpatient care for a number of individuals and could lead to more person-centered options that are cost-saving for the health system.
Footnotes
Acknowledgments
The authors wish to acknowledge the patient participants who shared their stories of a vulnerable time in their personal journey towards mental health recovery. We also acknowledge the contributions of our research assistants and clinical staff who supported survey administration and participant recruitment.
Declaration of Conflicts of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Hensel and Bolton have received consulting fees within the last 3 years from the Health Sciences Centre Foundation for advising on virtual care planning.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Canadian Mental Health Association Joule and Manitoba Medical Services Foundation Grant in Aid.
Ethical Approval
Research ethics approval for this study was obtained from the University of Manitoba Research Ethics Board (HS25298(H2021:435)).
Statement of Human and Animal Rights
Not applicable.
Statement of Informed Consent
Respondents gave written consent for review and signature before starting interviews.
Data Availability Statement
Data supporting this study are not publicly available due to confidentiality reasons. Please contact the corresponding author to discuss access.