
Abstract
Posterior spinal instrumented fusion (PSIF) is a treatment option for adolescent spinal deformity. PSIF leads to loss of spinal segment motion. It is unclear the extent to which spinal stiffness is perceived by adolescent patients after fusion. Focus groups of adolescents between ages 11 and 21 years who underwent PSIF for spinal deformity were performed. Focus groups were evaluated for common themes, and a 36-question survey was designed. Survey responses were analyzed relative to last instrumented vertebra (LIV) and Scoliosis Research Society-22 (SRS-22) scores. Five focus groups were held with 18 patients in total. Three main themes were identified by participants: 56% identified difficulty bending forward, 44% identified difficulty hunching while sitting, and 56% identified difficulty with twisting motions. Patients with more distal LIV reported significant more difficulty with self-care/grooming (P = .014) and chores (P < .001). SRS-22 function/activity scores correlated well with survey categories in self-care/grooming (r = .61; P = .049) and recreation (r = .69; P = .019). Focus groups suggest that spinal stiffness is frequently perceived and leads to alteration in daily tasks in adolescents after spinal fusion.
Introduction
Posterior spinal instrumented fusion (PSIF) surgery for severe spinal deformities in adolescents1-3 is associated with stiffness and loss of spinal mobility, which have been shown to substantially impact certain adolescent activities of daily living (ADL). 4 Many patients cite this stiffness and loss of spinal motion with an inability to return to previous sport. 5 Prior studies have focused on time to return to activities such as school and sports, though no other details on specific functional tasks that may be affected have been described. 6 It is clear that in adults with spinal deformity surgery who had fusion to the pelvis, major alterations in ability to perform life tasks have been demonstrated.
The Scoliosis Research Society-22 (SRS-22) is a validated 22-question survey used in patients aged ten and older that evaluates patient outcomes after surgery for idiopathic scoliosis. SRS-22 covers 5 domains: function/activity, pain, self-perceived image, mental health, and satisfaction with treatment. While reported SRS-22 function/activity scores significantly improved in adults spinal deformity patients with long fusion, 75% were unable to ride a bicycle and 78.6% were unable to use a squat toilet when previously possible preoperatively. 7 Adolescent patient perspective on stiffness with respect to daily life after PSIF has not been previously elicited in detail. Understanding patient perspective of illness and outcomes is a crucial part of delivering excellent care and facilitating active participation of patients and their families in the shared decision-making process. Promising newer fusionless techniques such as vertebral body tethering aims to improve flexibility and patient perception of stiffness, though understanding how stiffness affects patients is a first step in understanding if newer technologies improve patient-reported outcomes.
The first step in understanding a problem for a specific population is an in-depth interview to identify common themes. Focus groups can be powerful research tools in eliciting new perspectives. 8 Virtual focus groups have been proposed as an effective method of engaging diverse participants, including those of low income and varied racial/ethnic backgrounds in research.9,10 The objective of this study was to utilize focus groups in adolescents who have undergone PSIF for spinal deformity to assess patient perception of stiffness. Our null hypotheses are that adolescent patients experience no subjective changes in spinal stiffness following spinal fusion surgery and that distal fusion level is not correlated with greater perceived stiffness.
Patients and Methods
Study Design
Our Institutional Review Board (IRB) approved this study. Chart review was performed to identify adolescents between the ages of 11 and 21 years old who underwent PSIF for management of spine deformity over the past 10 years (2011-2021) and who were at least 1-year post-op. While adolescence is defined as 10 to 19 years of age, we elected to include patients up to age 21 to capture the perspectives of older adolescents who were at least 1-year post-op. Inclusion criteria were a diagnosis of adolescent idiopathic scoliosis (AIS) or Scheuermann kyphosis (SK), ability to communicate effectively in English, and access to audio and video conferencing capabilities. All eligible patients and their parents/guardians were contacted via telephone and email and were invited to participate in virtual focus groups. Patients aged 17 and older were consented over the phone. For patients younger than 17 years of age, consents were completed with a parent or guardian and assents were completed with the patient. Participants were asked to complete SRS-22 questionnaires prior to participating in focus groups.
Focus groups were held over a secure virtual platform (WebEx, Cisco Systems, San Jose, California). Participants were advised that these sessions would be recorded for the purposes of data collection. Each focus group consisted of 2 to 5 participants. Each participant participated in only one focus group. Focus group participants were given lists of dates to schedule participation; no attempt was made to cluster similar participants (based on age or time postoperative) in the same focus groups.
A trained focus group moderator followed a structured script to conduct one-hour focus groups. The script contained the following categories: morning routine, school/work, physical activities/sports, other extracurricular activities, hobbies, chores and ADL, and social activities. For each category, each participant was asked to consider whether spine stiffness following PSIF altered their ability to participate in any way. Questions were designed to be broad and open-ended to avoid leading participants to certain answers and to encourage discussion among participants. Examples of questions posed to the group are as follows: We are going to shift our discussion now to talk about leisure activities. These include things like backpacking, dancing, cycling, skiing, horseback riding, and swimming. This also includes gardening, camping, fishing, attending sports events/concerts. What things have you done recently? Please go ahead a make a list of activities that you enjoy on the scratch paper in front of you. Please include things you enjoyed both before and after surgery. Now, please think about if your activities stayed the same or if they changed after your surgery. Are there any new activities you are doing now that you didn’t do before your surgery? Are there activities you are no longer doing? Are there any adjustments you made to participation in these activities after surgery? Take a moment and write your thoughts down, and then we will come together as a group and discuss.
Each participant was given a chance to speak, and participants were encouraged to interact with each other and to build on ideas. Focus groups were frequently paused, and participants given several moments to reflect to encourage more reticent participants to speak. While the same questions were posed by the moderator to all focus groups, discussions naturally took different trajectories as different participants brought their own ideas and experiences to discussions.
This study is predominantly qualitative research; thus, no power analyses were conducted. Based on available focus group literature, it is recommended at least 4 focus groups of a particular patient population be conducted to achieve saturation of themes and terminated once the point of theoretical saturation is reached in which no new or relevant new themes or data is obtained. 11 Focus groups were stopped once 5 focus groups had been conducted and saturation was subjectively achieved. All eligible patients who wanted to participate in the study were contacted and were given the opportunity to do so.
All focus group videos were transcribed. Transcriptions were reviewed and common themes related to stiffness were identified and categorized. The number of participants who mentioned each theme was also noted. Focus group themes were divided into the following categories: general bending/twisting, self-care and grooming, chores, fitness and sports, recreation, and transportation. Using these themes, a preliminary 36-question survey was created and distributed to all focus group participants. Patients were asked to think about how flexibility and mobility of their trunk had changed following surgery and rated to a Likert scale of ease or difficulty in performing the task. Each question was then given a score of 1 (much more difficult) to 5 (much easier) based on participants’ responses. Questions were grouped into similar function or tasks related categories for statistical analysis.
Demographic information (age, sex, and race/ethnicity) and surgical details were collected via retrospective chart review. Focus group recordings/transcriptions and data were stored on a secure, encrypted platform through our institution.
Statistics
Descriptive statistics of baseline characteristics including demographic and surgical details were calculated. An analysis of variance (ANOVA) was conducted to assess the relationship between last instrumented vertebra (LIV) and participant survey response scores by category. A regression analysis was then performed to assess correlations between SRS-22 function scores and participant survey response scores by category.
Results
A total of 18 patients (13 females and 5 males) meeting inclusion criteria agreed to participate in this study. The age range of participants at the time of focus group participation was 14 to 21 years old. Sixteen patients (89%) had a diagnosis of adolescent AIS (mean Cobb angle 59° ± 9.1°) while 2 (11%) had a diagnosis of SK (mean kyphosis: 80° ± 7.1°). The mean number of levels fused was 10.8 ± 2.3 with 22% LIV to T12 or L1, 33% LIV to L2, and 44% LIV L3 (Table 1). The mean SRS-22 function score and total score were 4.4 ± 0.59 and 3.9 ± 0.45, respectively.
Demographic Characteristics of our Cohort of 18 Patients >1 Year Status Post Posterior Spine Fusion for Management of Deformity.

At the time of focus groups, participants were mean 29.3 ± 10.9 months postoperative (median = 34, interquartile range = 19.5). Five total focus groups were conducted with 2 to 5 participants in each focus group.
There were 3 main themes identified by participants during focus groups: 56% identified difficulty bending forward (touching toes, putting on shoes, and reaching low objects), 44% identified difficulty hunching while sitting (ie, painting, writing, and drawing), and 56% identified difficulty with twisting motions (ie, dancing, turning around while driving) (Figure 1). These identified themes and comments were used to design a postfocus group survey (Supplemental Appendix 1). Examples of some of the transcribed text are as follows: Socks are a bit harder now. I have to bend my knees like all the way up to my chest to get them on. I had noticed that I'm a lot less flexible. I wasn't really that flexible to begin with, but now, in my hips and in my back, I am even less flexible. I can’t touch my toes. I did a lot of martial arts before my surgery, but I have had to stop now because I can’t do all the bending and twisting that is required. Vacuuming and sweeping are very difficult.

Bar graphs demonstrating focus group themes by frequency. Each bar represents the percentage of focus group participants who endorsed difficulty secondary to postsurgical stiffness with the indicated task.
Eleven patients completed postfocus group surveys. Patients with more distal LIV demonstrated significant more difficulty with self-care/grooming tasks (P = .014) and chores (P < .001), though no difference in fitness/sports abilities (P = .58) (Table 2).
ANOVA Analysis of Average Survey Response Scored by Category [(1) Much More Difficult, (2) Slightly More Difficult, (3) No Change, (4) Slightly Easier, or (5) Much Easier] and LIV. Patients With More Distal LIV Demonstrated Significant More Difficulty With Self-Care/Grooming (P = .014) and Chores (P < .001).
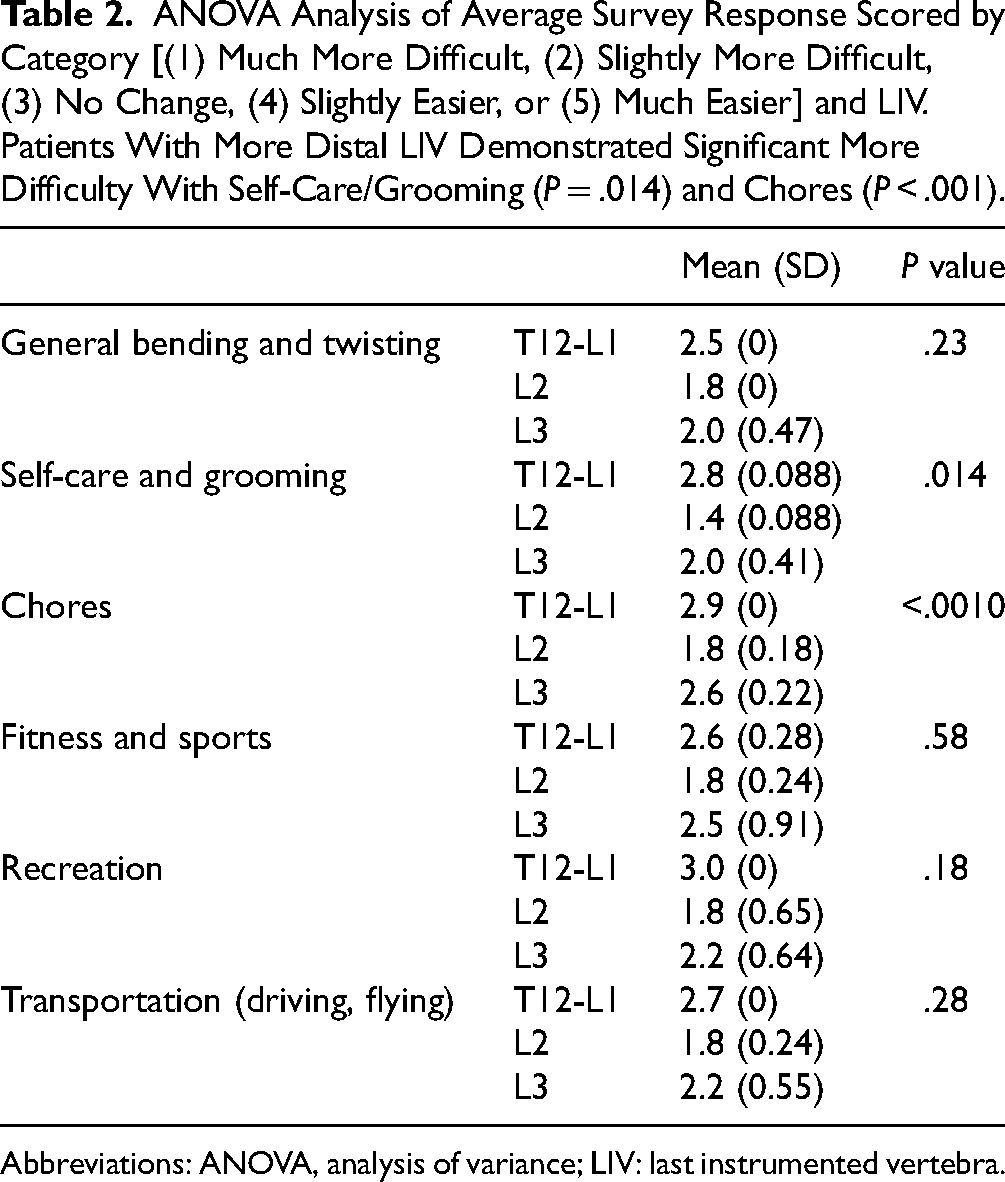
Abbreviations: ANOVA, analysis of variance; LIV: last instrumented vertebra.
SRS-22 function scores had statistically significant positive correlation with survey categories in self-care/grooming (r = .61; P = .049) and recreation (r = .69; P = .019) (Table 3). The other domains of general bending and twisting, chores, and transportation did not reach statistical significance with SRS-22 function scores.
Correlations of Scoliosis Research Society (SRS) Function and SRS Total Scores, and Average Survey Response Scored by Category [(1) Much More Difficult, (2) Slightly More Difficult, (3) No Change, (4) Slightly Easier, or (5) Much Easier].
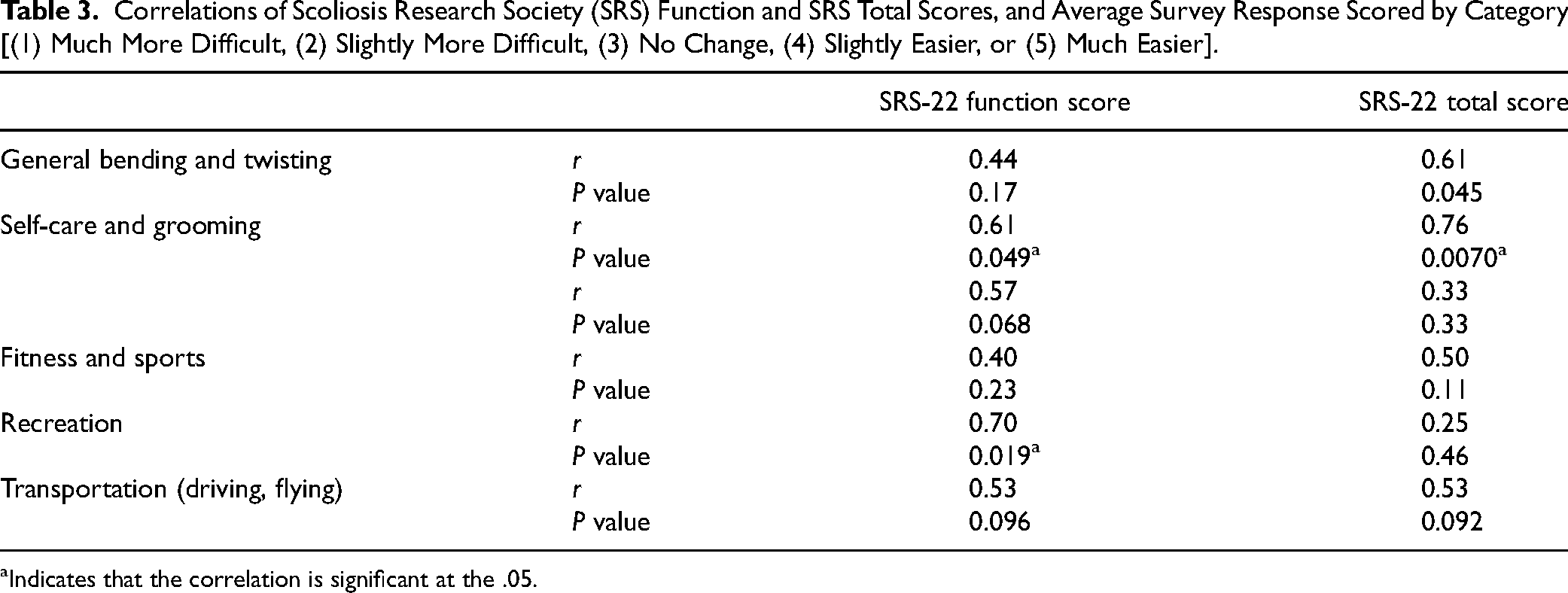
Indicates that the correlation is significant at the .05.
Discussion
It is important to emphasize that this study seeks to characterize adolescent perception of function and stiffness following spinal stiffness rather than objectively quantifying range of motion. In our study of 18 patients, we found that spinal stiffness is frequently perceived in adolescents following PSIF for management of spine deformity and leads to alteration in some daily tasks. A large proportion of our subjects identified stiffness-associated limitations with bending forward, hunching, and twisting. We found that patients with more distal LIV had more self-reported difficulty secondary to stiffness with tasks related to grooming/self-care and chores. Our regression analysis demonstrated moderate correlation between our findings and the SRS-22 function outcome measure, though with divergence in several specific domains. Our study is the first to explore the extent to which adolescent patients perceive stiffness and its associated limitations after fusion surgery.
There is variation in the literature regarding the effects of PSIF for the management of adolescent spinal deformity on quality of life. The SRS-22 is the most widely used outcome measure for adolescent spinal deformity surgery. The SRS-22 is a 22-question survey validated in patients aged ten and older that evaluates patient outcomes after surgery for idiopathic scoliosis. SRS-22 covers 5 domains: function/activity, pain, self-perceived image, mental health, and satisfaction with treatment. There are 5 questions in the SRS-22 pertaining to function/activity: current level of overall activity, current level of work/school activity, financial difficulties due to back, whether back pain limits ability to do things around the house, and whether back pain limits ability to go out with friends and family. The SRS-22 questionnaire does not specifically query postoperative stiffness or loss of motion, and several of the function questions focus on pain limitations to activity rather than stiffness limitations to activity. Our survey is a 36-question survey that focuses only on stiffness as a possible sequelae following PSIF.
Previous studies have found variable outcomes in the SRS-22 function/activity domain following surgery.12,13 Medium-term follow-up systematic reviews (2-5 years after PSF) demonstrated no significant improvement in the function domain.14,15 Longer-term studies (>10 years) after PSF suggest significant decrease in function and ADLs with time.4,16-19 Concerns have been expressed previously regarding ceiling effects of the SRS-22 outcome instrument.20-22 This ceiling effect has been shown to be worsened in adolescents younger than 15 and specifically affects the function/activity domain of SRS-22.23-25 In their study of early adolescent (aged 10-14) AIS patients, Karakaya et al found no statistically significant correlations between SRS-22 and a pediatric quality-of-life (PedsQL) inventory and concluded that SRS-22 may be inadequate in assessing physical activity parameters to evaluate overall quality-of-life. 26
Consistent with prior literature, our patients demonstrate overall good SRS-22 function/activity scores, but our focus group data suggests that perhaps SRS-22 function/activity scores are not fully capturing adolescent perspective related to stiffness and loss of mobility. This is further supported by the results of our regression analysis. We found moderate to good correlation between our results with the SRS-22 function/activity outcome metric suggesting that stiffness may lead to perceived functional deficit. These correlations were statistically significant for both self-care/grooming and for recreation. However, we also found statistically insignificant correlations in the remaining domains demonstrating divergence from the SRS-22 function/activity score that appears to be dependent on specific tasks/activities. Divergence suggests that the SRS-22 domain does not fully capture all functional changes associated with stiffness.
A more distal LIV has been shown to reduce motion in several planes, especially in forward flexion. 27 There is discordance in literature regarding whether trunk flexibility resulting from a more distal LIV has implications on patient reported outcomes as measured by SRS-22.28,29 This discrepancy suggests limitations in the ability of SRS-22 to evaluate functional outcomes related to stiffness. In our study, we found that patients with more distal LIV reported stiffness-related functional limitations with self-care/grooming tasks and chores. Functional outcomes related to stiffness and LIV have not previously been elucidated.
Our preliminary survey was able to elicit perceived functional changes experienced by adolescent patients following PSIF that were not captured by SRS-22. In contrast to the activity/function domain of the SRS-22 survey which contains only 5 broad questions, our survey includes 36 questions, all of which are related specifically to stiffness. Our utilization of focus groups allowed us to design specific, activity-focused questions applicable to our population. Each question in our survey is related to an activity, and this helps respondents hone in on specific tasks rather than considering an abstract topic such as stiffness on its own. We suspect that the granularity of our survey enabled it to capture stiffness not captured by SRS-22. The benefit of SRS-22, however, is that it is a widely accepted, validated metric. It encompasses function/activity, pain, self-perceived image, mental health, and satisfaction with treatment, and it was not designed to capture the nuances of stiffness. The purpose of creating our survey was not to supplant SRS-22, but rather to offer a supplement to help facilitate future investigations of stiffness following PSIF. Our survey requires critical refinement and external validation prior to any future use as a possible adjunct to SRS-22 when stiffness is an outcome of interest.
Limitations
There are several limitations to consider in our study. First, our study is limited by a small cohort studied at a single institution. While there were only 18 participants included in our study, we followed guidance in previous literature regarding recommendations on limiting focus groups once discussion themes reach saturation. 11 By our fourth and fifth focus groups, no new themes were identified and all researchers were in agreement that saturation had been achieved. Second, in our study, we found that patients with more distal LIV reported stiffness-related functional limitations with self-care/grooming tasks and chores. However, we did not have any participants with LIV L4 or L5, as these patients were rare in our practice, and these levels were not included in our study. Third, in our survey, we did not include all topics discussed in our focus groups and instead elected to include only the most common themes and activities brought up by our participants. While we made efforts to make our survey as broadly applicable as possible, there may be certain regional biases of the activities reflected in our questions, limiting generalizability of our survey. Finally, our study contains more female participants than male participants. AIS is more common in girls than in boys, and there were therefore more girls eligible for participation than boys. It is important to consider that the implications of surgery for spinal deformity may be perceived differently by girls and boys, and this was not captured by our study.
Conclusions
Spinal stiffness is frequently perceived in adolescents following PSIF for management of spine deformity and leads to alteration in some daily tasks. Stiffness limits activities such as bending forward, hunching, and twisting. More distal LIV is associated with greater self-reported stiffness. Ours is the first study to assess in detail and report on adolescent perspective of stiffness.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241282937 - Supplemental material for Adolescent Perception of Stiffness After Spinal Fusion Surgery
Supplemental material, sj-docx-1-jpx-10.1177_23743735241282937 for Adolescent Perception of Stiffness After Spinal Fusion Surgery by Sarah E. Lindsay, Austin Thompson, Jenny Hummel, Matthew F. Halsey and Scott Yang in Journal of Patient Experience
Footnotes
Authors’ Contributions
Sarah Lindsay and Scott Yang: conceptualization; Sarah Lindsay and Austin Thompson: data curation; Scott Yang: formal analysis; Sarah Lindsay, Austin Thompson, Jenny Hummel, Matthew Halsey, and Scott Yang: investigation; Sarah Lindsay, Austin Thompson, Matthew Halsey, and Scott Yang: methodology; Scott Yang: supervision; Sarah Lindsay: writing–original draft; Austin Thompson, Jenny Hummel, Matthew Halsey, and Scott Yang: writing–review and editing.
Data Availability
The data that support the findings of this study are available within the article or in its Supplemental Material. Additional data from focus groups are not publicly available due to patient confidentiality.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Review Committee Statement
Approval was obtained from the Oregon Health & Science University Institutional Review Board (IRB approval number: 00023135). This study was performed in accordance with the 1964 Declaration of Helsinki and US HIPAA regulations. All patients who had reached the age of majority provided written consent. For patients under the age of majority, written consent was obtained from a parent or guardian and written subject assent was obtained.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.