
Abstract
Our objective was to assess the impact of a 4-question patient audio interview (this is my story [TIMS]) on medical staff empathy and communication with hospitalized patients and loved ones. We recorded a 4-question audio interview with patients and posted it to the electronic health record. We used a cross-sectional, mixed methods design to pilot this patient version of the TIMS intervention. To evaluate the intervention we collected a brief evaluation survey and conducted semistructured interviews with medical staff. Fifty-three participants responded to our TIMS evaluation survey. Fifty of 51 respondents reported the TIMS file contained useful information. Twenty-four respondents reported listening to the file decreased their distress. Most responded that they either did not have distress or the TIMS file did not change their distress. Of concern, 3 people reported that listening to the file increased their distress. Importantly, most respondents reported feeling greater empathy for the patient after listening (53%) and most reported listening improved their communication with family members (63%, n = 9/13). Qualitative analysis revealed most participants had positive impressions about TIMS. We conclude that empathy and communication were both improved with use of the 4-question TIMS recording.
Key Points
Brief audio files (this is my story [TIMS]) improve communications among medical teams and patients and loved ones.
TIMS files enable clinicians to feel more empathy for their patients.
TIMS files can reduce stress on clinicians due to a lack of knowledge of their patients.
Introduction
During the COVID-19 pandemic effective and humanizing communication was encumbered by many factors that were overwhelming to cope with as an unprecedented worldwide shift was occurring in the medical field. 1 Clear communication between interdisciplinary and multiprofessional teams, persons with life-threatening illnesses and families is critical for building trust, reaching common ground, and guiding shared decision making, 2 yet building trust in the isolation necessitated by the pandemic was very challenging. 3 The loss of trust, common ground, and shared decision making were evident in the self-reported increase in distress that was observed in our previous investigation into the absence of loved ones in the hospital due to COVID-19. 4 The movement in communication was most evident in changing methods and reduced frequency because nationwide isolation precautions necessitated by the evolving COVID-19 pandemic upended traditional delivery of care, shifting from intimate, in-person interactions to largely remote communications among providers, patients, and families. 2
One solution is to make remote and virtual technology available, yet this may occur without properly integrating it into the natural workflow or culture of care. Additionally, virtual platforms for communication have inherent challenges in providing holistic, interdisciplinary support to patients and their families. 3
Satisfaction with communication was also hindered in discussions with patients, or their loved ones, with studies finding that not being kept informed about the patient's medical condition, and perceptions that family members were not consulted about preferences for medical procedures or treatments resulted in lower satisfaction with care. 3
Satisfaction with communication is based upon the hearer being able to take the information and translate it into meaningful details, including their perspective and way of understanding what is happening, the meaning assigned to it, their culture, and their context. 5 To assist in overcoming the complications of communication, there are several methods to include effective and humanizing communication while those who provide these details may be at a distance or not able to participate in care planning. Incorporating patient narratives into the electronic health record (EHR) is an opportunity to integrate patients’ values and beliefs into their care and improve patient–clinician communication. Equally as important, there was an observed benefit for the medical staff as they felt it made a more robust communication and connection with the patients. 6
This Is My Story (TIMS) is a brief audio file of a patient or loved one of a patient answering on their behalf 4 questions: How do you prefer to be addressed? What brings you joy? What does your medical team need to know about you to care for you best? What brings you peace? The intent of the TIMS file is to humanize the patient, improve clinician empathy and improve communication between the clinical team, the patient and the patient's loved ones. The purpose of this study is to assess whether this distilled version of a TIMS recording limited to simply these 4 questions provides the same benefits to the clinical team as our previously published work utilizing a more open-ended interview has established. 3 We used a cross-sectional, mixed methods design to pilot this patient version of the TIMS intervention. To evaluate the intervention we collected a brief evaluation survey and conducted semistructured interviews with medical staff. An additional modification to our previous protocol involved asking patients themselves rather than loved ones to answer the questions.
Open-ended TIMS interviews conducted in our previous studies yielded audio files that ran between 10 and 20 min in length. These TIMS files required extensive editing to reduce them to the desired length of 2 min or less so they might be quickly utilized on rounds or in other clinical settings.7,8 Analysis of the original TIMS interviews resulted in the 4 questions used in the current study as providing the most information that could provide a personal snapshot of the patient and be clinically actionable. This approach has the added benefit of resulting in an unedited file that runs between 1 and 6 min and is much more easily edited.
Methods
Study Design
To evaluate the TIMS intervention, we used a pretest/posttest single group design with a pre/postsurvey and postintervention qualitative staff interviews.
Eligibility and Recruitment
All unit staff was eligible to participate in this study if they provided care or services to a patient with a TIMS recording embedded in the electronic medical record. This included physicians, doctors, fellows, nurses (traveling and institutional), residents, social workers, patient experience representatives, and care technicians. From those who completed the survey, a subsample of staff was asked to participate in a brief semistructured interview.
Patients were identified for participating in the TIMS program by the charge nurse when the chaplain came to the unit twice per week. Considerations for inclusion were cognitively intact patients who had agency who were predicted to remain on the unit for at least 3 days, to enable the TIMS recording to be edited and posted. The chaplain briefly explained the study and if the patient agreed, began the recording with the patient's consent, followed by the 4 questions. Between March and August of 2022, TIMS files (n = 202) were recorded and posted.
Medical Team Questionnaire Development and Administration
Clinical staff who listened to TIMS files were queried prior to listening to the TIMS file and afterward. Our questionnaire is self-report based, allowing the respondent to evaluate their distress, communication, and empathy, after having listened to the recorded interview and determining for themselves how much had changed. We took this approach as there are no current validated measures that we were aware of that could capture this as an a priori method. The prelistening questionnaire consisted of 4 items and the postlistening questionnaire five. These were accessed with a QR code; data was collected via Qualtrics. Responses to the surveys were collected anonymously. If the participant agreed to be contacted for the brief semistructured interview, they provided their preferred email.
Staff Interviews
Staff interviews were conducted on the unit 1:1 with a medical student (CI). Questions for semistructured interviews were developed by the study team to address questions related to the feasibility, acceptability, and staff-perceived benefit of TIMS (see interview guide).
Results
Quantitative Analysis
Staff Participant Description
Fifty-three participants responded to our TIMS evaluation survey. Among survey participants, average time working on the unit was over 4 years (mean 57 ± 47.9 months). The majority of respondents (64%, n = 34) were nurses. Additional roles that responded included physicians, nurse practitioners, technicians, residents, social workers, dietitians, and receptionists (Table 1).
Clinical Roles of Those Listening to TIMS Files.
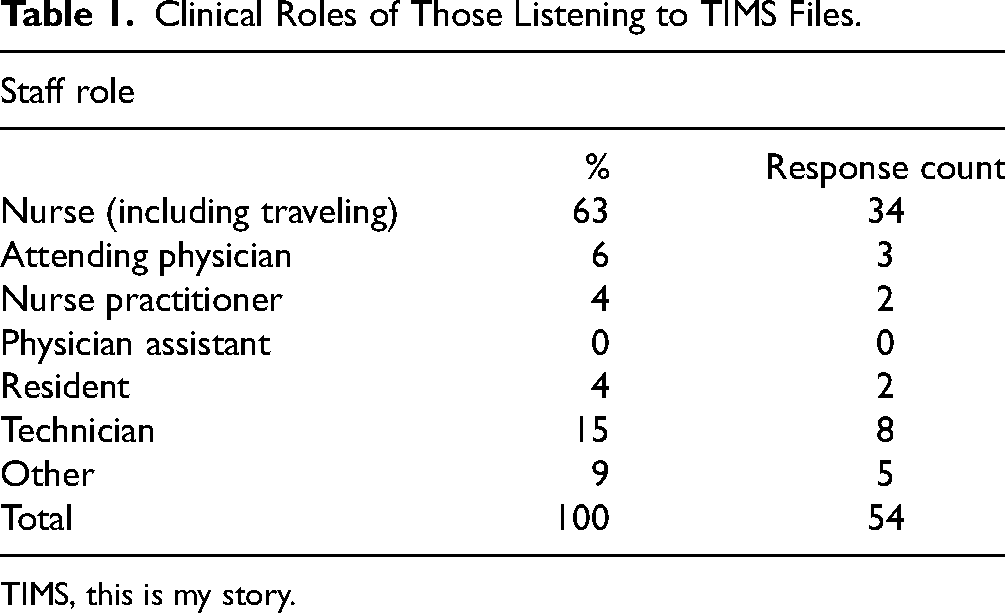
TIMS, this is my story.
Prior to listening to the TIMS file almost half of respondents reported minimal or no knowledge of the patients (n = 22) and a small proportion reported some or substantial distress relative to their knowledge of the patient (n = 8) (Table 2).
Staff Distress Prior to TIMS File.

TIMS, this is my story.
Almost all respondents reported the TIMS file contained useful information (50/51 reported yes or some useful info.)
In terms of self-reported effect of the TIMS file on distress and empathy, 24% of respondents reported listening to the file decreased their distress, but the majority response was that the respondent either did not have distress or the TIMS file did not change their distress. Of concern, 3 people reported that listening to the file increased their distress (Table 3).
Change in Staff Stress After TIMS.

TIMS, this is my story.
* 2 subjects did not respond
Importantly, most respondents reported feeling greater empathy for the patient after listening (53%) and of those who communicated with family members, most reported listening improved their communication with family members (63%, n = 9/13) (Table 4).
Change in Staff Empathy after TIMS.
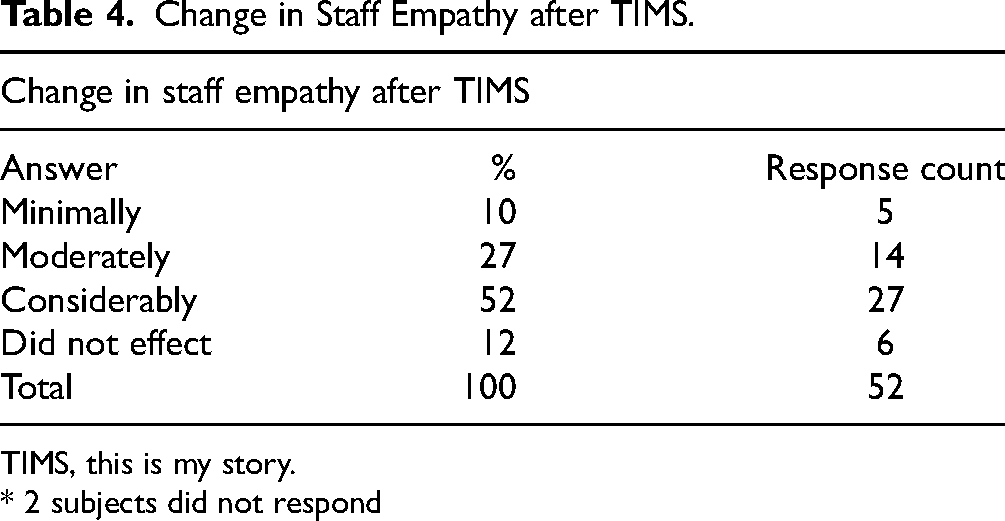
TIMS, this is my story.
* 2 subjects did not respond
Qualitative Analysis
Of the participants who were involved in patient selection for TIMS, several factors influenced the selection of patients: mental status, behavior, personality, isolation status, and time to discharge. The length of the recording and the number of questions was deemed appropriate while still providing information about the patients. Two questions were mentioned as specifically helpful in soliciting actionable patient preferences: (1) How would you like to be addressed and (2) What should the care team know to take better care of you?.
Overall, users had positive impressions about the use of TIMS to provide additional perspectives and multidimensionality to their patients. Users indicated that the TIMS files were helpful in providing context to someone who is “not just a bunch of figures on a flow sheet.” Additionally, the files provided ways to “understand [the patients] a little better” and form greater connections in periods where users were lacking time to spend time with patients outside of direct duties. No interviewees reported negative feelings or emotional difficulties in listening to the TIMS files. Of note, users received TIMS files and were notified about the files in different ways listed as follows: via secure chat, email, and a note with a link in the chart. Users were encouraged to listen to the files in different ways as well, via in-person chaplain reminders as well as emails reminding staff to review the TIMS files. Staff suggested that technology delivery could be streamlined to improve user experience in accessing the files. Some also expressed the audio volume and quality of the patients’ interview was too low at times. Of note, users consistently seemed to listen to files at workstations and without headphones, sometimes as an activity shared with other staff members working on the floor.
Most interviewees did not note direct care changes due to TIMS—the impact was more helpful in providing additional dimensions to the patients themselves and understanding them. One user indicated that in periods of difficulty in connecting with patients, the TIMS files became a helpful resource in finding avenues to better connect with them. A notable instance of direct care change involved patient preferences in how they were addressed, which TIMS users noted was not something that was typically included in medical charts. One TIMS user described a meaningful change of addressing a young patient as follows: “I specifically remember like one patient, that it kind of stuck with me. We, had, our patient on the unit, who had been there for a really long time, and he was a younger kid, and we would always call him […] Mr So and so when he was like 20, so we listened to his interview, he said he like to be called Alex, so I started calling him Alex […].”
No interviewees mentioned changes to how TIMS files changed their interactions with the patients’ families. However, they did note greater understanding of the patient and their support system when family came up as a topic in the TIMS files. Notably, one interviewee remembered hearing an interview file from family since the patient was intubated, which was impactful to provide context to the patient.
Alternative venues of interest that were suggested for the TIMS program included outpatient settings, rehabs, in-patient, and in ICU settings where patients are not verbal. Additionally, one user expressed interest in expanding languages offered for the TIMS program to be more inclusive of patients who could participate.
Discussion
Our study aimed to determine if a streamlined recorded audio interview consisting of only 4 questions asked of the patient, known as a TIMS file, could help improve empathy among clinical staff caring for hospitalized patients on a medicine unit and whether communications between patients, clinical staff, and loved ones was also improved. Our previous work demonstrated a positive impact in both outcomes utilizing more open-ended interviews with loved ones of noncommunicative patients. 4 In seeking to streamline the process of creating TIMS files so that the process can be scaled, we conducted a simple, 4 question interview with patients who could speak for themselves. Our results indicate that this format remains helpful in increasing empathy and improving communication.
Clinical staff have been experiencing burnout and compassion fatigue for some time, and this was exacerbated by the COVID-19 pandemic.1,9,10 TIMS was created as a direct result of interactions with clinicians expressing their frustration at not knowing anything about their patients, who were often intubated, sedated and prone, with no loved ones at bedside to speak for them. Success with the TIMS intervention on the medical intensive care unit led to expansion throughout the Johns Hopkins Hospital. The current study builds upon that success and demonstrates that when the interview is distilled to 4 simple questions asked of patients themselves both empathy and communication are improved, outside of pandemic conditions.
This study and our previous research demonstrate the ability of a TIMS file to improve communication and increase empathy on the part of the medical staff. Our intention is continue to expand use of TIMS files in many more medical settings and to assess their impact in additional dimensions, including impressions from patients and loved ones about the experience of recording a TIMS file and their perceived impact on the care they receive. We are also involved in streamlining the process of recording, editing and posting the file so that other clinicians might easily include TIMS as part of their scope of work.
Limitations
One concern that emerged in this study and furthers results from our previous work is that some clinicians indicate that listening to the TIMS file increases their distress. In qualitative interviews with medical staff we learned that the files make it more challenging to maintain distance from patients, although that is balanced by increased empathy.
Our study is limited in the number of responses to our survey versus the number of TIMS files generated. This may indicate fatigue with repetitive surveys about individual TIMS files.
Conclusions
A TIMS audio file recorded with patients simply answering 4 questions and placed in the EHR helps improve empathy on the part of medical staff and improves communications between the care team, patients, and loved ones.
Footnotes
Authors Contributions
Concept and design: E.T., J.W., and M.A-S; acquisition, analysis, or interpretation of data: E.T., J.W, M.A-S, and C.I.; drafting of the article: E.T. and C.I.; critical revision of the article for important intellectual content: E.T., J.W., M.A-S, and C.I.; statistical analysis: N/A; administrative, technical, or material support: E.T., J.W., C.I., and M.A-S.
Data Sharing
All the data submitted comply with Institutional or Ethics Review Board requirements and applicable government regulations.
Disclosure Statement
The authors declare that there is no conflict of interest.
Ethics and Consent
This study received approval to conduct research from the Johns Hopkins Health System Institutional Review Board (Research Ethics Board) under submission number IRB00335743. It proceeded with a waiver of consent documentation for the patient or their legally authorized representative, as this research was of minimal risk and not normally required outside of the research setting.
Funding
This research has been generously supported with grants from the John Conley Foundation for Ethics and Philosophy in Medicine.