
Abstract
Female cancer survivors (FCS) have a higher risk of infertility compared to women without a history of cancer. Consuming healthful diets could improve female fertility and promote healthy cancer survivorship. As an initial step to intervention development, this study explores FCS and healthcare provider (HCP) perspectives regarding nutrition and fertility. We conducted semi-structured interviews with 11 HCPs and a secondary analysis of qualitative data from 20 FCS. Data were analyzed using directed content analysis. Two broad themes were identified with several interrelated subthemes: (1) Barriers to Optimal Nutrition: Subthemes: Time Constraints (Both HCPs and FCS); Absence of Standardized Guidelines due to perceived lack of Research and Education (HCPs); Unclear and Insufficient Dietary Guidance (FCS) and (2) Ideas and Opinions about Fertility Nutrition: Subthemes: Skeptic Acknowledgment of Potential (HCPs); Motivation to Change Nutrition Behavior (FCS). Healthful nutrition may improve fertility in women and would be of particular importance for FCS who are at an increased risk of infertility. Addressing the challenges in adopting a healthful diet is essential for creating effective interventions.
Introduction
Female cancer survivors (FCS) represent a distinct population with specific health challenges, particularly regarding fertility and nutrition. The risk of infertility among FCS is significantly higher than among women without a history of cancer, as treatments commonly used for cancer, such as chemotherapy, radiation, and surgery, can cause irreversible damage to reproductive organs and disrupt hormonal regulation.1–3 These treatments can affect ovarian reserve and function, uterine health, and the endocrine system, all essential for fertility. 4 Furthermore, the emotional and psychological toll of infertility, compounded by the experience of cancer, can affect the overall well-being of FCS. Given the growing number of FCS worldwide, understanding the fertility challenges and finding supportive interventions that address the unique needs of FCS are critical for enhancing quality of life and improving long-term health outcomes. 5
Recent research indicates that diet plays an important role in improving fertility outcomes and enhancing survivorship in FCS. 6 Diets rich in whole grains, unsaturated fatty acids, vegetables, fruits, and fish—often referred to as plant-forward diets—are increasingly recognized for their potential to improve reproductive health and promote overall wellness in cancer survivors. 6 Plant-forward diets, such as the Mediterranean diet, have been shown to reduce inflammation, regulate blood sugar levels, and improve hormonal balance, all of which can support fertility. 7 Such dietary approaches have also been linked to a lower risk of cancer recurrence and chronic diseases, such as obesity, which can be of particular concern for cancer survivors due to the long-term effects of treatment.8,9
Despite these findings, research examining the use of nutrition as a complementary treatment to support fertility treatments among FCS is scarce. As an initial step to intervention development, we are exploring FCS and healthcare provider (HCP) perspectives regarding nutrition and fertility. Our previous study found that FCS have suboptimal dietary quality, face multi-level barriers to healthful nutrition, and express interest in a dietary intervention to improve fertility. 10 This study further explores these findings and describes the interrelationships between HCPs’ and FCS perspectives on the role of nutrition in fertility treatment.
Methods
Study Design
This study employed a qualitative descriptive design. Data were collected through in-depth interviews with HCPs working in fertility treatment centers and oncology units. FCS data were obtained from secondary data, which have been previously published. 10 The study was approved by the IRB at California State University, Chico (IRB # 2023-85).
Participants
HCPs were recruited from two states, California and Colorado, through the networks of the last author. They comprised reproductive endocrinologists, fertility specialists, in-vitro fertilization (IVF) nurse coordinators, and a registered dietitian. FCS were recruited through ResearchMatch, an online recruitment service, 11 and online cancer survivorship support groups. Details for FCS recruitment and data collection have been outlined in another study, but briefly, FCS were of reproductive age (18 - 40 years) and resided in the U.S., were not actively undergoing treatment (> 6 months out of treatment), and were considering or had started family building. 10 To maximize participant diversity, participants were purposefully sampled (eg, race/ethnicity, age, history of cancer survived, specialty, and gender for HCPs). FCS consented to their de-identified data being used for future research.
Data Collection and Analysis
HCPs completed a structured descriptive survey and a consent form online. Interviews were conducted virtually by four trained female research assistants, via Zoom compliant with the Health Insurance Portability and Accountability Act. Interviews with HCPs, each lasting 35-40 minutes, explored perspectives on fertility nutrition and its potential to enhance fertility treatment outcomes among FCS. Interviews were audio-recorded, transcribed, and analyzed using NVivo software. 12 Data collection ceased at thematic saturation. Directed content analysis guided data coding and analysis, using a team-refined codebook, with two researchers independently coding the data.
Previously collected FCS data were also analyzed using directed content analysis to identify barriers and opportunities for integrating nutritional guidance into fertility care. 10 A separate codebook was developed and refined, with codes assigned to barriers, motivators, and perceptions regarding fertility nutrition. Two team members independently coded the data. Themes from both datasets were synthesized to explore their interconnections. This is visually displayed in Figure 1.
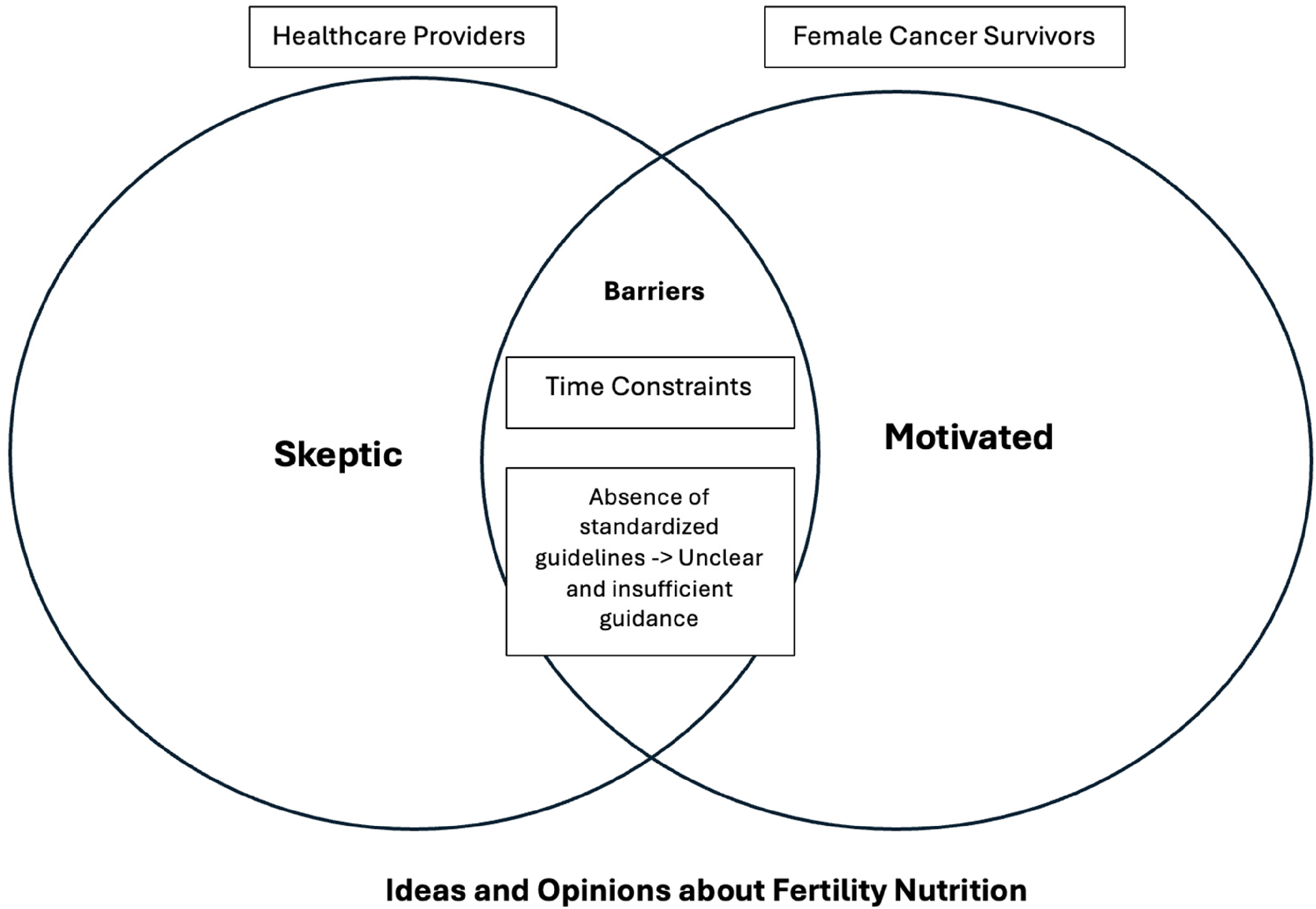
This figure displays the interrelatedness of themes and subthemes. HCPs and FCS share a common barrier of time constraints to providing nutrition-related care and adopting healthful nutrition, respectively. Furthermore, the absence of standardized nutrition guidelines among HCPs and institutions affects FCS, as the nutrition information they receive is often unclear and insufficient. In terms of ideas and opinions about fertility nutrition, HCPs are generally more skeptical about its potential benefits, whereas FCS are more motivated to adjust their nutrition behaviors to improve their fertility. FCS, female cancer survivor; HCP, healthcare provider.
Confirmability, credibility, dependability, and transferability were applied to ensure trustworthiness. 13 Confirmability was achieved by documenting all research-related activities. Credibility was ensured through peer-checking, where the research team reviewed the codes and themes to verify the accuracy of the data analysis. Dependability was upheld by involving at least two team members in the data analysis process. Transferability was supported through the purposive sampling of research participants.
A normality test was performed for continuous FCS and HCP data using the Shapiro-Wilk test, and the data were found to be normally distributed. Descriptive data were summarized as means and standard deviations for quantitative variables and frequencies and percentages for categorical variables using SPSS v. 28.
Results
Descriptive Characteristics
Eleven HCPs and 20 FCS participated in this study (N = 31; Table 1). The mean age for HCPs was 47.09 ± 9.5 years. Most of the HCPs identified as female (n = 10, 91%), non-Hispanic White (n = 9, 82%), and had more than 10 years of practice (n = 7, 64%). HCPs had varying specialties, including IVF Nurse Coordinator (n = 4, 36%), Reproductive Endocrinology and Infertility (REI) (n = 3, 27%), Medical Oncology (n = 1, 9%), and Registered Dietitian (n = 1, 9%).
Participant Demographic and Personal Characteristics.
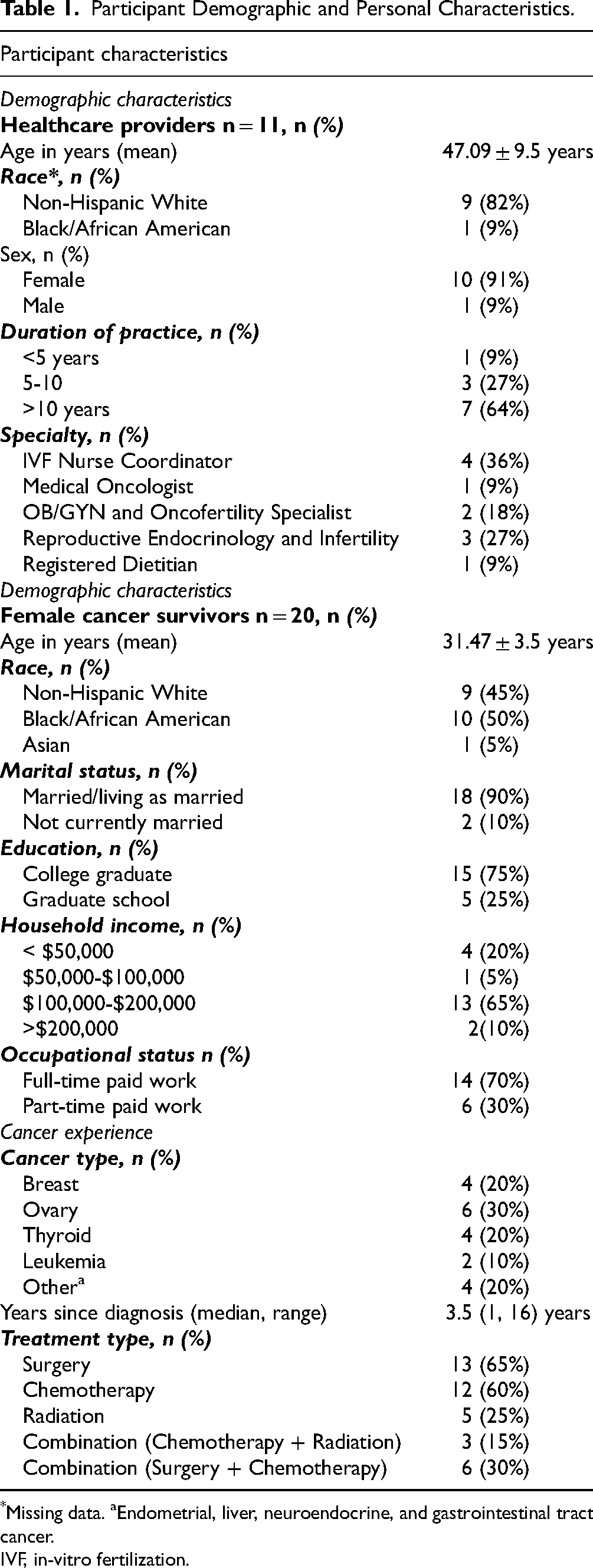
*Missing data. aEndometrial, liver, neuroendocrine, and gastrointestinal tract cancer.
IVF, in-vitro fertilization.
The mean age for FCS was 31.47 ± 3.5 years. Most identified as either non-Hispanic White (n = 9, 45%) or Black/African American (n = 10, 50%). Most of the women were married or living as married (n = 18, 90%) and were college graduates (n = 15, 75%), with some in graduate school 25% (n = 5). Regarding cancer type, breast cancer survivors comprised (n = 4, 20%), ovarian cancer (n = 6, 30%), thyroid cancer (n = 4, 20%), leukemia (n = 2, 10%), and other cancers comprised (n = 4, 20%). The median number of years since cancer diagnosis was 3.5 years (range 1 to 16 years). Most had undergone surgery (n = 13, 65%), chemotherapy (n = 12, 60%), or a combination of surgery and chemotherapy (n = 6, 30%). Fertility History is described elsewhere. 10
Qualitative Findings
Two broad themes were identified with several interrelated subthemes: (1) Barriers to Optimal Nutrition: Subthemes: Time Constraints (Both HCPs and FCS); Absence of Standardized Guidelines due to perceived lack of Research and Education (HCPs); Unclear and Insufficient Dietary Guidance (FCS) and (2) Ideas and Opinions about Fertility Nutrition: Subthemes: Skeptic Acknowledgment of Potential (HCPs); Motivation to Change Nutrition Behavior (FCS). Table 2 compares the different themes, while Figure 1 illustrates the interrelationships among these themes.
Themes and Exemplary Quotes.

IVF, in-vitro fertilization.
Theme 1: Barriers to Optimal Nutrition
Subtheme: Time Constraints
Our analysis identified barriers to providing and adapting optimal nutrition among HCPs and FCS, respectively. Time constraints emerged as a significant barrier among both groups. This subtheme was consistently discussed by both HCPs and FCS, highlighting the impact of limited time on the ability to provide or receive adequate nutrition information and education. HCPs frequently expressed that time limitations in their work environment were a major obstacle to addressing nutrition optimally with patients. Several of them noted that the pressures of maintaining a fast-paced clinical schedule significantly reduced the time they could dedicate to discussing nutrition in-depth with patients. H1005, a 39-year-old IVF nurse with over 3 years of practice, stated, “Honestly, it's probably because of time…it's about an hour-long appointment, and so there really just isn't time to kind of go into it in a whole lot of depth.” Another provider, H10010, a 33-year-old registered dietitian for about 7 years, reported that time pressures often led to prioritizing immediate medical concerns over preventive health strategies like nutrition education:
“Providers are asked to do a lot of things, and they need to prioritize and oftentimes nutrition is just not going to fit in the time that they have. If it's a 30-minute visit about fertility, they may not have time for a good discussion on diet and nutrition.”
FCS echoed similar time constraints. Despite their intentions to eat healthily, their demanding jobs and lifestyle often made this difficult. Several FCS explained that their busy schedules led them to rely on convenient, easy-to-prepare meals.
F1017, a 25-year-old leukemia survivor, stated: “When I get extremely stressed, and I have too many things going on to manage, then like, my diet is probably one of the first things that goes out the door.” F1006, a 33-year-old thyroid cancer survivor mentioned skipping breakfast altogether because her mornings are so busy: “That is pretty frequent. I often don’t have breakfast just because I feel too busy in the morning.”
Subtheme: Absence of Standardized Guidelines due to perceived lack of Research and Education (HCPs); Unclear and Insufficient Dietary Guidance (FCS).
Many HCPs reported the lack of evidence-based, fertility nutrition dietary guidelines for women both with and without a history of cancer. This absence was largely attributed to a perceived deficiency in research specifically targeting fertility nutrition. Providers noted that the lack of tailored guidelines made it difficult to offer concrete advice or create personalized nutrition plans for patients. As H1008, a 49-year-old REI specialist with 20 years of practice put it, “Every single patient asks me, Are there any foods that can be to help me with my fertility … I don't have patient facing materials or patient facing guidelines from the American Society for Reproductive Medicine or the American College of OB GYN. I don't have those resources to give to them.” Another HCP, H1002, a 56-year-old REI specialist with 24 years of practice explained, “And with such a dearth of data, it's hard for us to give them any specifics other than, you know, healthy diet and healthy lifestyle. And that's about as specific as we get which is obviously very general.”
On the other hand, FCS reported feeling confused and unsupported by the dietary guidance they received from healthcare professionals. The advice they were given was often too vague or generalized, making it difficult to apply to their specific needs. One survivor, F1027, a 30-year-old female ovarian cancer survivor, shared, “I was just given, like the surface information about it [fertility nutrition].” Another, F1028, a 37-year-old leukemia survivor, shared, “And they’re like, ‘you know eat some chicken.’ I’m like, okay well I can only eat so much chicken in two weeks [laughs]. So I asked for some ideas, and they didn’t have specific foods or drinks or anything.” Survivors expressed a strong desire for more personalized, practical dietary recommendations that considered their cancer history and fertility. As one FCS, F1013, a 30-year-old breast cancer survivor, reported: “So I’d rather be told the exact food to take. Yeah, I’d rather be told that you should take this food for breakfast, you should take this for lunch, and you should take this for dinner, and so on.”
Theme 2: Ideas and Opinions about Fertility Nutrition
Subthemes: Skeptic Acknowledgment of Potential (HCPs); Motivation to Change Nutrition Behavior (FCS).
Both HCPs and FCS expressed varying ideas and opinions regarding fertility, nutrition, and its potential benefits. Some HCPs expressed hesitation in recommending fertility nutrition interventions. Many acknowledged the potential of nutrition in enhancing fertility, but they highlighted the lack of definitive studies linking healthful nutrition to improved fertility outcomes. This perceived lack of robust scientific evidence led to skepticism and reluctance to integrate nutritional advice into fertility treatments. H1001, a 34-year-old IVF nurse coordinator with 9 years of practice, shared, “I have to see good studies that actually prove that diet has an impact on fertility outcomes … I am skeptic at nature … I think that well rounded nutrition hopefully would have an impact. So, I would say like 20% [impact].” This sentiment was also shared by H1002, “I think but for the most part is that it [fertility nutrition] just hasn't been studied.” and H1004, a 58-year-old IVF nurse coordinator, “There are studies but I don't know if there are a lot of food studies or nutrition studies that help you know, that prove that it helps fertility.”
FCS, in contrast, seemed motivated to adopt healthful nutrition, and this appeared to stem from a deep desire to gain control of their health and fertility, particularly after the experience of cancer treatment. For some participants, having an aspect of their fertility, such as their nutrition, which they could work towards improving, felt empowering to them. F1017 shared, “So, it's a little bit empowering to hear that like, hey, there is something you can like more than just bear through this whole process and you can do something. That's really nice.”
This sentiment captures the essence of how adopting healthful nutrition wasn’t only about eating better—it was about having a sense of control in a situation where they had felt largely powerless. F1002, a 25-year-old liver cancer survivor also shared that her motivation for maintaining healthful nutrition would not only support her health but will additionally benefit her future child's: “But I'm, yeah, totally motivated, especially knowing that most likely it's [healthful nutrition] going to impact me systemically with my current medications and stuff, and I want to be as healthy as possible knowing I'm going to have immunosuppressants and that could impact my child.”
Discussion
This study explored HCPs’ and FCS's perspectives on fertility nutrition as a preliminary step to intervention development. This discussion compares the study's findings with previous research and integrates the main themes into key takeaways.
Time constraints in healthcare are a common issue that hinders patient-centered care and the provision of quality nutrition counseling services. 14 Healthcare professionals often face heavy workloads, tight schedules, leading to rushed appointments, limited communication, and less personalized care. Additionally, time pressures can cause HCPs to prioritize efficiency over empathy, potentially compromising patient satisfaction and overall health outcomes. 15 Fertility-related nutritional care often requires personalized and in-depth discussions, which can be challenging to fit into brief appointments. 16 This is especially important for FCS, as fertility is not only a major concern but also has significant psychological and social impacts on their quality of life. 17 An interdisciplinary team approach is required to address the fertility needs of FCS, ensuring that referrals and treatments are properly coordinated. 18 This will reduce the burden on individual HCPs and ensure that the necessary information, such as nutritional information, is provided.
Several FCS in our study reported that work-related barriers, particularly time constraints and the stress associated with their jobs and lifestyles, hindered their ability to maintain a healthy diet. This finding aligns with other studies that have identified work demands as one of the most common obstacles to healthful lifestyle behaviors among young adults.19,20 Therefore, it might be essential to provide young adults, including FCS, with strategies to improve their dietary habits while considering their work and lifestyle. Dietary interventions could consider addressing time and stress-related constraints associated with women's work and be tailored to fit their lifestyles. 10
Many HCPs in our study reported that the nutritional guidelines they provided to patients were not standardized and varied from facility to facility. They also mentioned a lack of research and education in the field of fertility nutrition. The lack of standardized nutritional guidelines, in addition to insufficient research and education, in fertility nutrition presents significant challenges in healthcare practice. Without clear, consistent recommendations, FCS may receive conflicting advice from different providers or facilities, leading to confusion and uncertainty about the best dietary practices to improve fertility. This inconsistency in care could undermine the potential benefits of nutrition in reproductive health, as patients may follow outdated or ineffective strategies. Additionally, HCPs, lacking evidence-based resources, may miss opportunities to educate patients on the critical role of nutrition in fertility, thus limiting proactive care and optimal patient outcomes. The lack of clear, standardized guidelines can hinder fertility outcomes, as patients may miss out on the latest research-based dietary advice. Healthcare institutions could consider developing standardized protocols, supporting ongoing research, and providing continuous education to ensure optimal nutritional care for fertility.
HCPs are often skeptical about the potential for nutrition to improve fertility due to the emphasis on evidence-based medicine and the uncertainties surrounding complementary and alternative medicine (CAM), with which nutrition is frequently associated.21,22 This finding is similar to the results from our study. While nutrition research itself is rigorous and increasingly evidence-based, its association with CAM—often viewed as lacking scientific validation—fuels skepticism among healthcare professionals. Because nutrition-related therapies are often categorized under CAM, which has historically been met with caution due to concerns over safety and efficacy, HCPs may be reluctant to incorporate them into fertility treatment plans.23,24 In addition, medical education for HCPs outside the field of dietetics typically includes minimal training in nutrition, further contributing to skepticism.25,26 The conflicting advice within the nutrition field, along with the individual variability in responses to dietary changes, and the limited nutrition knowledge among HCPs further complicates its integration into mainstream medical practice. However, nutrition is a rigorous science with research at its core. Advances in nutrition research have led to the development of personalized nutrition, which tailors diets to individual needs. Despite this, there seems to be a disconnect between HCPs’ perceptions about nutrition and advances in nutrition science. Therefore, expert bodies such as the American Society for Reproductive Medicine (ASRM) might need to provide more recognition of the crucial role of nutrition in fertility treatments, much like how the American Institute for Cancer Research (AICR) and the American Cancer Society (ACS) have acknowledged nutrition's importance in cancer care.
In contrast, several studies, including ours, have shown that cancer survivors are generally motivated to change their nutrition and lifestyle behaviors.27,28 This could be because these are risk factors that they can be empowered to control. Research indicates that providing detailed nutritional information significantly improves dietary practices among cancer survivors, encouraging them to adopt healthful eating habits. 29 Given these reasons, there is a need for HCPs to provide FCS with evidence-based nutrition guidance during their fertility and reproductive journeys.
Our study findings indicate that FCS with reproductive desires may benefit from specific, practical interventions post-cancer treatment. These might include the integration of registered dietitians into oncofertility clinics, where they can provide individualized dietary counseling. Additionally, the development of standardized nutrition handouts focused on fertility can help ensure consistent messaging across HCPs. Expanding survivorship care plans to formally include fertility-related nutrition components may also enhance continuity of care post-treatment. These interventions should be tailored to meet the specific needs of FCS, taking into account factors such as cultural appropriateness and health literacy.
Limitations and Strengths
Our study had a small sample size of both HCPs and FCS, which may limit generalizability. However, this allowed for in-depth interviews and the exploration of nuanced perspectives on fertility nutrition, and existing gaps. While the FCS sample was diverse, there was limited diversity among HCPs, with a predominance of non-Hispanic White participants.
Qualitative research often presents challenges when combining primary and secondary datasets 30 However, these were minimized in our case, as the study PI (last author) designed and oversaw data collection for both studies. The PI intentionally adopted a phased approach to data collection, enabling comparison and contrast across stages as a foundation for future intervention development.
Conclusion
FCS are eager for reliable evidence-based nutrition guidance to support reproductive health and survivorship, and HCPs are uniquely positioned to provide it. Improving FCS fertility outcomes will require the development of standardized fertility nutrition guidelines, the integration of nutrition support into oncofertility treatment, and prioritizing funding for fertility-related nutrition research with a focus on the FCS population. Future research could explore the feasibility of a tailored evidence-based fertility nutrition guideline and its effect on fertility outcomes among FCS. These efforts could ultimately offer FCS the consistent, trusted nutritional support they seek, improving both reproductive outcomes and overall survivorship.
Footnotes
Acknowledgments
We would like to acknowledge Sruthi Vobbilisetti, BS, Harpreet Dhami, BSN, and Divya Bodapati MS, for their dedication and hard work in recruitment, consenting, interviewing, and transcript cleaning.
Author Contributions
CK, LA, MZV, and KB designed the study. Research Assistants listed in the acknowledgements conducted the interviews with JQO. JQO and CK coded all transcripts. JQO, CK, and NLB conducted data analysis. JQO, CK, and NLB wrote the first draft of the manuscript. All authors contributed to refining and writing the final draft of the manuscript. All authors have read and approved the final manuscript.
Data Availability Statement
De-identified interview transcripts are available upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
This study received approval from California State University, Chico IRB (IRB # 2023-85), and all research was carried out in accordance with this. Written informed consent was obtained from participants for the publication of their anonymized information in this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the California State University, Chico’s Research, Scholarship and Creative Activity (RSCA) Grant. The funder played no role in data collection, interpretation and reporting.