
Abstract
Long coronavirus disease 2019 (COVID-19) is poorly understood, widespread and debilitating. Integrative medical group visits (IMGVs) provide group medical care virtually or in person and are reimbursed by insurance payors. IMGV introduces integrative modalities such as mindfulness, nutrition, and acupressure in a person-centered, supportive, and educational environment. To evaluate a telehealth IMGV program called Nourish to Flourish (N2F) for patients with long COVID, three researchers conducted a qualitative analysis of pre- and post-group individual interviews. Twenty-five patients provided interviews, of which fifteen included pre- and post-group individual interviews. Main themes were unpredictable symptom patterns, a common range of emotions associated with long COVID experience, reconceptualizing self-identity, multiple barriers to care in conventional settings, and connections formed in N2F. Although symptoms varied, N2F participants found commonalities in their experiences of living with long COVID. They empathized with one another regarding changing symptoms, inconsistent social support, shifting identities, and barriers to effective medical care.
Keywords
Introduction
One in 10 adults experience chronic COVID-19 symptoms after acute infection. Common long-term conditions include postexertional malaise, fatigue, dizziness, brain fog, and gastrointestinal symptoms. 1 Research to date has focused mainly on assessing symptomatology and elucidating mechanisms of disease in long COVID.2–4 To date, few studies have examined the experiences of individuals living with long COVID, particularly in the United States. 5 There is also scant information about digital interventions for long COVID. 6 This manuscript explores the experiences of patients with long COVID who had been evaluated at a post-COVID specialty clinic and referred to a virtual integrative medical group visit (IMGV) program called Nourish to Flourish (N2F).
N2F is a patient-centered model of care adapted from an evidence-based IMGV program for patients with chronic pain, which itself was adapted from the mindfulness-based stress reduction program. 7 A pragmatic randomized controlled trial of IMGV for chronic pain found that IMGV significantly decreased emergency room visits and improved mental health-related quality of life. 7 Authors JB and IR co-developed N2F in 2021 as a specific adaptation of IMGV8,9 tailored to patients with long COVID. Patients with long COVID meet as a group for 8 weekly 2-h sessions via telehealth. Sessions were co-facilitated by a medical provider and a peer with long-COVID with experience with group facilitation and training in mindfulness. Weekly session content included health education topics, principles of mindfulness-based stress reduction, self-care techniques such as self-acupressure and self-massage, and anti-inflammatory nutrition. In a pilot mixed-methods study conducted in 2021 with the first 2 cohorts of N2F participants, perceived stress scale scores improved and the Measure Yourself Medical Outcome Profile (MYMOP ®) primary symptom severity scores decreased. 8
Method
Researchers conducted semistructured individual interviews before and after delivery of N2F to evaluate patients’ experiences with long COVID, the trajectory of their illnesses, and their thoughts about participating in a telehealth IMGV called N2F. Medical providers at a post-COVID recovery clinic (including author JB) diagnosed participants with long COVID and referred them to the group intervention. Experienced qualitative researchers (JB, IR) developed interview questions (Appendix A, B). Interviews were conducted virtually via Zoom. Research Assistants transcribed interviews. 10 This study, reviewed by the University of North Carolina at Chapel Hill IRB # 21-1326, was deemed exempt in part because it is an observational study rather than a clinical trial. Nonetheless, researchers read a consent form to each participant and obtained their verbal consent.
Three researchers completed a thematic analysis following the 7 steps of thematic analysis as described by Nowell et al 11 The research team familiarized themselves with all the transcripts. Initial inductive coding involved peer debriefing and the development of a coding framework. Transcripts, memos, and team meeting notes were stored securely on Microsoft Teams. 12 Through discussion, codes were combined into themes and subthemes. Team members discussed and adjusted the wording of these categories to achieve consensus. Finalized themes and subthemes reflect the analytical choices of the research team.
Results
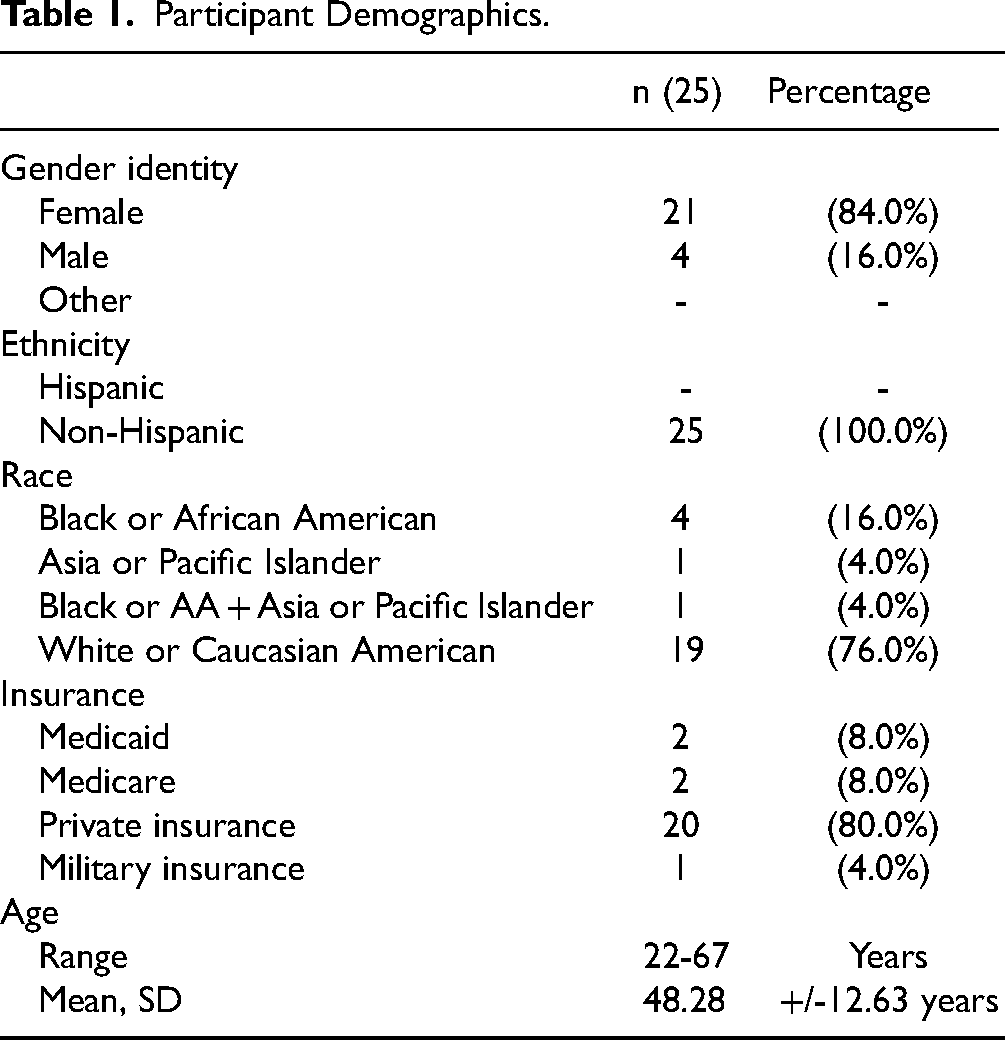
Researchers interviewed 25 individuals, and fifteen participants completed both pre- and post-interviews. The sample was predominately female (84%), White or European American (76%), and privately insured (80%). The mean age of participants was 48 years. (See Table 1)
Participant Demographics.
Five main themes coalesced from qualitative analysis: (1) unpredictable symptom patterns, (2) common range of emotions associated with long COVID experience (3) reconceptualizing self-identity, (4) multiple barriers to effective care in conventional settings, and (5) N2F providing space for patients to share their experiences and support one another.
Theme 1: Unpredictable Symptom Patterns
Participants reported many different symptoms with waxing and waning severity (See Table 2). Reported symptoms included brain fog, fatigue, shortness of breath, heart palpitations, pain, anxiety, depression, insomnia, numbness, headaches, dizziness, loss of balance, muscle weakness, vision changes, digestive problems, malaise, and chest tightness. Many patients described brain fog and provided instances of impaired memory, such as forgetting appointments and difficulty with word finding. One participant stated that brain fog was like “when you're on a computer, or the TV's, you know, running on Wi-Fi, or whatever, and occasionally, it stops to buffer to catch up … it's just hard to function because your mind and your head just feels weird (pt.106).” Patients commonly referenced fatigue when they talked about needing frequent breaks during the day, feeling chronically exhausted, drained, and “not having the energy to do some of the things you used to do (pt.102).” One participant described needing “extravagant rest” (pt.205) in the face of severe fatigue. Shortness of breath was described as breathing that requires excess exertion or “tightness in the chest (pt.104).”
Characterizing the Emotional Experience of Long Coronavirus Disease 2019 (COVID-19).

Patients often described long COVID as a tumultuous “roller coaster” (pt.107) where symptoms waxed and waned. The breadth of symptoms, which encompass both physical and psychological impairments, was difficult to navigate. One participant stated, “I just, I really want to be able to manage my life. With all this stuff going on in my body, I've never been this sick before and having to deal with physical issues as well as all the emotional mental things that [I] have to go through (pt.104).”
Factors that exacerbated their symptoms included “too much physical activity, doing too much mental activity, any emotional upset, too much social interaction (pt.203).” Moreover, patients frequently mentioned that additional stressors heightened their anxiety and disrupted their sleep, leading to worsening symptoms. One patient noted that certain foods such as alcohol, coffee, or processed foods worsened their symptoms (pt.210).
Theme 2: Common Range of Emotions Associated with Long COVID Experience
Many participants described similar emotions managing long COVID. Subthemes included negative and positive emotions related to the severity and length of participant symptoms, gratitude for support and frustration when support was lacking, and their feelings about the future. Examples of negative emotions include grief, uncertainty, helplessness, frustration, and fear (See Table 2).
Persistent and debilitating symptoms often caused participants to feel helpless. One patient described the experience as “digging a hole and crawling in it” (pt.205). Some patients were scared that their symptoms would continue to worsen, wondering “how much longer will this last, and how much longer can I continue like this (pt.207)?”
Commonly, patients described frustration with family and friends who had unrealistic expectations. Patients noted that their loved ones struggled to grasp the chronic nature of their condition and the profound uncertainties surrounding it. One patient expressed this sentiment by saying, “I think everybody has been like, you know, I can't wait to get better, I hope you get better and better. And I'm like, I don't think I'm going to get better anytime soon (pt.104).”
On the other hand, positive emotional reactions reflected resilience and hope. Some patients acknowledged that the journey to feeling better would not be easy but was possible. When talking about changing their lifestyles and adhering to health care recommendations, one patient said, “You got to do it, you got to do it, you got to do it … if you start skipping because you don’t feel quite right, then I think I’m not going to get better (pt.102).” This resilience was often rooted in patients feeling hopeful that chronic symptoms would improve. Some patients recognized that long COVID was an evolving condition and were also hopeful that research would improve treatment options.
Patients sometimes drew strength from their social circles. They expressed gratitude for the understanding and support they received from their friends and family. As one patient emphasized, “I'm lucky that my husband and kids are very supportive, and a lot of people don't have that (pt.208).”
Through social media, some patients found solace in realizing that they were not alone. Reflecting on their encounter with support groups on Facebook, one patient shared, “It was so eerie reading their stories and how similar everyone was. Some had a few different things but just the way people would describe the tightness of the chest and a feeling like something was sitting on them and not being able to expand, it was just crazy to read all these people writing things that I could've written (pt. 208).”
Theme 3: Reconceptualizing Self-Identity
When faced with a new disease, most patients struggled with adapting to and accepting their new reality. Some patients commented on the loss of identity due to the inability to continue working. For example, “That's one thing to be sick, but then to be sick and not be able to work…all those things that we have used to describe ourselves as who we are … have been just kind of ripped away from me right now. It's very humbling … it's time to look at who you are outside of all those things (pt.116).” Other participants described the struggle between resisting and accepting their new identity as a chronically ill person. This participant describes that struggle: “I'm coming to terms with the fact that I'm never going to be who I was before I got sick, but I have to learn how to be this person that I'm becoming because she's so foreign to me. It's like waking up in a stranger's body every day and not knowing what to expect … learning to let go of the feeling of, ‘When am I going to get better?’ And accept the fact that this may be who I'm going to be. And how do I adjust? How do I find a quality of life with the new limitations that I'm still not sure are going to stay (pt. 107)?”
A subset of the patients interviewed experienced chronic pain since contracting COVID. Most people experienced life-altering chronic fatigue. A patient described learning to accept this reality as, “I hurt all the time. My joints and stuff hurt all the time. I just have to listen to my body and when my body says it's tired, I have to go to sleep. So finally beginning to accept where I am (pt. 204).”
The strategy of “listening to one's body” and avoiding overexertion is sometimes referred to as “pacing.” This has become an important cornerstone of long COVID treatment.13,14 A young adult patient recounted the danger of pushing through their exhaustion and trying to put “mind over matter”: “People just want to push it to the back of your mind because I know at the beginning, I was like ‘I’m 22 years old. I can’t let this thing take over my body.' A lot of people think that if you don’t think about it, it won’t happen, but I’ve come to learn that it will even if you don’t think about it. Nobody thinks that they’re going to pass out behind the wheel on the way home and hit a light pole (pt. 110).”
Some patients described shifting roles within their marriages as necessitated by fatigue and cognitive impairment. For example, this patient describes an inability to help problem-solve financial issues, “We had a financial situation the other day and I just had to tell myself, I just looked at my husband and said, ‘You take care of it, I can’t deal with it.' He wanted to talk about it some more last night and I told him, ‘I’m not going to talk about it, I can’t deal with it. You’re going to have to deal with it yourself ’ (pt. 111).”
Theme 4: Multiple Barriers to Effective Care in Conventional Settings
Many patients expressed frustration at a lack of effective treatment for long COVID and a desire for respect and empathy from their healthcare providers. Unfortunately, many did not receive that, and were often met with skepticism. One participant described being met by the medical community with blank stares, like “deer in the headlights” (pt.106).
Participants expressed frustration about persistent symptoms and a lack of effective treatment options. Several participants thought that the most frustrating part of long COVID was that “nobody knows how to treat it (pt.101).” One participant described feeling discounted when her provider did not have answers, “… there was still the pain and breathlessness. And then after that, she wasn’t taking me seriously, like a long-term thing. You know, she told me to rest (pt.104).” Another participant related her experience of abandonment, which was shared by others on Facebook: “I think a lot of them felt abandoned by the medical community for a long time too because there are a lot of doctors who said, ‘I’m sorry, there's nothing that we can do for you.' The fact that there was so much emphasis being put on the vaccine and helping people with acute COVID, and it was like ‘what about us' (pt.208)?”
Many patients noted the inaccessibility and inadequacy of medical care. The absence of accurate COVID testing early in the pandemic led to uncertainty about a diagnosis of long COVID. Patients described lack of health insurance and frustration related to accessing disability benefits. For example, one patient explained: “Things that are completely out of my control but are negative things have really been kind of a setback for me lately. Like I’ve been trying to deal with health insurance and disability benefits with my HR and they keep messing everything up … The emotional exhaustion is just killing me. My head hurts all the time and I want to cry all the time (pt.201).”
Many participants used complementary approaches to manage long COVID including acupuncture, massage, chiropractic, Qi Gong, and dietary supplements. One patient explained: “Doing Qi Gong has helped I think … with like my energy, you know, even if it's for that moment, like mentally just kind of given me a space to detach from all the finance stuff, the grief, but you know, the loss of so much in such a concentrated span of time (pt.116).”
Theme 5: N2F Provides Respect, Connection, and Knowledge
Many patients in N2F found that they could identify and rely upon each other to help make sense of their experiences. Individuals identified a range of components of N2F that they found useful, including breathwork, meditation, general relaxation techniques, nutrition, and yoga. They also learned the general importance of daily, regular practice. These patients describe approaches to self-care encountered through N2F: “For me, just going back through and doing the body scans and different meditations just reminds me the importance of doing that daily and having a daily practice for it … For the aches and when I feel like all shivery and gross, I think just doing meditation, taking a bath with some salt. Yeah, I do like self-massage. I don't know if it is— I mean, it makes me feel more relaxed. And I think when we're more relaxed, right, it lowers like our cortisol, which helps our body, in general, heal and recover things (pt. 116).” “I learned a lot about nutrition and relaxation and doing yoga. I guess it was probably well that, and the relaxation meditations were my favorite out of everything (pt. 107).” “I had times where I couldn’t go to sleep or stay asleep. So, I felt like yoga, or meditation can help with that. So, I felt all of that is the calming stuff … which is one of the things that they’ve told me about the oxygen and my heart rate being so high, some of the meditation things that can help self-regulate some of that (pt. 102).” “What I got out of it is trying to eat better. It gave you a sense of awareness, of being mindful of what you eat. Also, it made you mindful of trying to look at the better side of things, of what God has provided for us. Looking at nature and meditating. Trying techniques to try to calm yourself down even though yes, we’re going to have upset moments. Trying to appreciate what you have right now (pt. 111).” “I think a lot of validation was important for all of us, being heard. [The doctor] was just there and compassionate and receptive to discussing any issue. And then the breathing techniques, the yoga techniques, the nutrition, antioxidant type information, I thought that was all really beneficial (pt. 205).”
In relation to participation in N2F, one of the most common things that patients said they got out of the experience was the reassurance gained from hearing about others’ similar experiences: “I guess just that feeling of connecting can be comforting, because isolation feels stressful. And like that loneliness of [does] anyone else know what I'm going through (pt. 119)?” “I just think like getting to know each other, just getting to know each other and supporting each other. I feel like we all took turns…having a good week and a bad week. And whenever anyone was having a bad week, we all just rallied to their support, and we dig each other out of the hole. I think that was really good, that was special. Also be able to laugh with each other, laugh at ourselves. I was thinking we were going through so much but not so much that we couldn’t laugh at ourselves in the situation that we’re in. And friendships, it did build friendships with some of the people there (pt. 207).” “The reason I would recommend it [N2F], is the support, the comradery. I don’t think Long COVID is really known out in the general public. I think it's getting there, but I don’t think a lot of people even hear about it or know about it. You go through these symptoms, and you just don’t know why you’re feeling this way. So, the group was able to validate how I was feeling (pt. 117).”
In this quote, a participant describes how the group helped them understand both the varied presentation of long COVID and the common need for rest: “The more you push, the more tired you are, and so through the group you learn that you need to rest more. You need to take more breaks; you need to show yourself grace. With Long COVID you walk a tight rope. What you do today, you may not be able to do tomorrow. What you do today, you might be able to do two weeks from now, but you may not be able to do it tomorrow. And if you do too much today, you may end up in bed for two days, so it's just a very-it's a balancing act that you want to do enough every day, that you don’t want to be a couch potato. Nobody wants to be a couch potato, but you have to find that balance without exhausting yourself …. It seemed in observation from my own perspective and from what I [listened to] from everybody else is that COVID seemed to attack everybody differently and it seemed to have attacked wherever you were weakest and wherever you had issues prior to COVID. It seems to have attacked that area and made it ten times worse (pt. 107).”
The most common criticism of N2F was the lack of information specific to the treatment of long COVID. Participants sought solutions to their conditions, and they were eager to learn about research findings. “I would just love to have more information about the research that's going on or the trials that are going on out there. It would’ve been great to have more information about that because we didn’t get any of that (pt. 109).” Some participants remarked that the 2-hour session was too fatiguing. “With brain fog and fatigue that was a little long for me to stare at the computer because when I’m concentrating and looking at a screen at the same time trying to process things, that wears on me (pt. 106).”
Discussion
The 5 themes resulting from this qualitative analysis of N2F participant interviews shed light on the experience of living with long COVID and offer insights regarding the potential therapeutic role for group based medical care for patients with long COVID. This manuscript also contributes to a growing body of knowledge about the lived experience of long COVID.5,15–19 Among participants, there was a wide variety of symptoms and symptoms patterns. Participants’ symptoms were similar to those reported in other studies of patients with long COVID, including postexertional malaise. Postexertional malaise is emerging as a defining feature of long COVID. 1 Postexertional malaise refers to a delayed and often protracted exacerbation of symptoms in response to excessive physical, emotional, or mental exertion. 20 Therefore, patients’ comments about learning to listen to their bodies are particularly salient given the central role that pacing has come to play in the management of postexertional malaise associated with long COVID.1,13
Amid the diversity of symptoms, there were common emotional responses to living with long COVID. Fear, frustration, and isolation were often accompanied by appreciation for social support from other patients with long COVID. Patient's emotional responses, sources of support, and experiences were similar to those in other populations and included experiencing fragmented health services and increased social isolation. 21 Previous research has indicated that the long COVID illness experience has influenced identity, changed the relationships patients have with their providers, and altered how individuals perceive the reliability of the medical system in its entirety.5,22 Given the pervasive experience of fragmented care, group medical visits may be one mechanism for minimizing harm and rebuilding trust in the medical establishment, as groups diminish the hierarchy of patient-provider relationships and provide extended time with providers.23,24
For some participants, meeting with other long COVID patients was key to their social network. This occurred through social media as well as through N2F. N2F addressed patients’ needs for treatment options, respect, and connection. Many participants appreciated the introduction of complementary health modalities, and group visits are a potential avenue for increasing access to integrative care. Providing breaks or shortening the 2-hour session to 90 minutes could lighten the cognitive load for participants. Future iterations of N2F can include new research findings and treatment approaches as best practices arise. Research to elucidate the specific role of N2F as compared to other social support and integrative healthcare options (such as social media, online support groups, in-person support groups, group therapy, or individual provision of integrative therapies) is needed.
Understanding the range of emotions experienced by long COVID patients will help strengthen future adaptations of N2F. These findings will also help formal and informal caregivers better understand the emotional and physical needs of people with long COVID. Findings can also inform new models of care that support the expansion of group-based models alongside research to refine group-based interventions. This aligns well with the groundwork laid by the United States Department of Veterans Affairs (VA) for person-centered healthcare transformation. The VA has been a leader in the redesign of healthcare towards a “Whole Health” approach that is person-centered and individualized.25,26 The VA applied this same vision to their conceptualization of a population-based approach to treating long COVID that includes peer support, groups, complementary and conventional treatment, and health coaching. 27
The Agency for Healthcare Research and Quality recognizes that some people with long COVID are disabled. 27 There are varying ways of defining disability from an individual medical condition to a social construction. The social relational model of disability offers a means of evaluating this complexity. According to this framework, disability is constructed at 3 levels: The experience of limitations of the body, the “social relationships that undermine the psycho-emotional wellbeing of people labeled or designated as ‘impaired’,” 27 and the restrictions people encounter in society.
Regarding long COVID and N2F, the social relational model provides a framework for understanding the needs of patients with long COVID. First, it is important that N2F affirms the biological basis of participants’ symptoms and supports effective treatment. Second, N2F creates a social space capable of connecting patients, normalizing emotional responses to chronic illness, and supporting psycho-emotional well-being. Regarding the restrictions people with long COVID encounter in society at large, spaces such as N2F facilitate the exchange of ideas and strategies to advocate for and obtain accommodations and services.
This study has certain limitations. First, it occurred within a single post-COVID recovery clinic and fails to account for the experiences of patients at other clinics or within different healthcare systems. Second, the patient sample does not fully represent all patient groups, as most patients were female, White or Caucasian American, and privately insured. Persons not represented include non-English speakers and those undiagnosed due to disparities in healthcare access or poor health at baseline that obscures the role of long COVID. To enhance the comprehensiveness of research in this area, it is important that future studies include more patients from underrepresented populations.
Conclusion
People with long COVID describe being on a roller-coaster whose course involves symptoms that are unfamiliar and unpredictable. Group-based care provided treatment options, respect, connection, and knowledge to patients. This model of virtual healthcare delivery may be particularly well suited for the needs of patients with long COVID and may help to re-establish trust in the medical establishment. Given the magnitude of this illness and the lack of definitive treatment, Integrative Medical Group Visits such as Nourish to Flourish can harness the power of individuals to work collectively to manage this chronic, debilitating illness.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241230144 - Supplemental material for Different but the Same: Common Themes in Illness Experience Among People With Diverse Long COVID Symptoms and the Potential Benefits of Virtual Group Medical Visits
Supplemental material, sj-docx-1-jpx-10.1177_23743735241230144 for Different but the Same: Common Themes in Illness Experience Among People With Diverse Long COVID Symptoms and the Potential Benefits of Virtual Group Medical Visits by Jessica Barnhill, Aisha Chilcoat, Bethany Kavalakatt, Raveena Mata, Malik Tiedt and Isabel Roth in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735241230144 - Supplemental material for Different but the Same: Common Themes in Illness Experience Among People With Diverse Long COVID Symptoms and the Potential Benefits of Virtual Group Medical Visits
Supplemental material, sj-docx-2-jpx-10.1177_23743735241230144 for Different but the Same: Common Themes in Illness Experience Among People With Diverse Long COVID Symptoms and the Potential Benefits of Virtual Group Medical Visits by Jessica Barnhill, Aisha Chilcoat, Bethany Kavalakatt, Raveena Mata, Malik Tiedt and Isabel Roth in Journal of Patient Experience
Footnotes
Key Points:
Patients with long COVID share common illness experiences amid varied symptoms. Despite their large numbers, patients with long COVID experience isolation and frustration encountering disbelief and resignation in social and medical settings. Managing long COVID in group settings may alleviate suffering and improve function.
Acknowledgements
The authors wish to acknowledge and thank the people who committed the time and effort to share their experiences so that collectively we raise awareness, reduce additional harm, and help restore health for millions of persons affected by long COVID. We also wish to thank our mentors and pioneers in the field of group medical visits, Dr Paula Gardiner and Dr Jeff Geller.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Complementary and Integrative Health (grant number 5T32AT00378-12, 1-K01-AT011578-01A1).
Ethical Approval
Ethical approval was obtained from the Institutional Review Board of the University of North Carolina at Chapel Hill study ID 21-1326.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Institutional Review Board of the University of North Carolina at Chapel Hill study ID 21-1326 with the approved protocols.
Statement of Informed Consent
Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.