
Abstract
Background:
The global COVID-19 pandemic has resulted in the widespread suspension of bariatric surgical programs. Although this rapid adaption was initially necessary, the implications of delaying the most effective treatment for weight loss in a population at risk from this crisis are not well known. Moreover, as the health care trusts plan the reintroduction of elective services, it is vital to also consider the patient’s perspectives, to adequately weigh up the benefits and risks of this recommencement in the current climate.
Objectives:
We aimed to investigate the impacts that postponing bariatric surgery has had on patients, and their priorities when restarting elective surgery.
Methods:
An online survey of patients awaiting surgery was undertaken, examining the physical and psychological impacts of pandemic isolation policies and postponing surgery, and exploring patient preferences regarding surgery during the pandemic.
Results:
Of 71 patients, 67.6% gained a median of 4 kg (interquartile range: 2.6-6.4), and 74.6% had adverse psychological effects; 93.0% were keen to proceed with surgery. Thematic analysis of qualitative data revealed delays have worsened physical symptoms, increased anxiety, and delayed secondary life-altering treatments.
Conclusion:
From the patient’s perspective, postponing surgery has been deleterious and efforts to safely reintroduce bariatric programs should be promoted.
Introduction
Background
The global COVID-19 pandemic has led to major disruptions in health care systems, exhausting available resources, and resulting in the suspension of elective surgical services (1,2). Bariatric surgery has followed a similar fate. In United Kingdom, one of the worst affected countries by the pandemic, bariatric services have been restricted, with only the most clinically urgent cases being prioritized currently (3).
Patients with morbid obesity are one of the most significantly at-risk cohorts from COVID-19 (4). On the other hand, the efficacy of bariatric surgery in the treatment of obesity is unequivocal (5). The 2016 NICE guidelines state that bariatric surgery can improve quality of life, reduce the risk of premature mortality in patients with morbid obesity, and is the main option of treatment for adults with a body mass index (BMI) above 50 kg/m2 (6). In addition, people with BMI of 40 kg/m2, or between 35 kg/m2 to 40 kg/m2 with significant disease that can be improved with weight loss, in whom all the nonsurgical measures have been tried but failed to achieve clinically beneficial weight loss, bariatric surgery is recommended (7). There is growing evidence that prior metabolic surgery with subsequent weight loss and improvement of metabolic abnormalities is associated with lower rates of hospital and intensive care unit admission in patients with obesity who became infected with SARS-CoV-2 (8).
Objectives
The suspension of bariatric services, combined with nationwide policies of isolation while understandable and necessary, the impact of these policies on patients with morbid obesity remains poorly understood. Additionally, as services plan to reintroduce elective surgery, very little is known about the patient’s perspective on undergoing such procedures in the current climate. We aimed to explore these lived experiences to understand the personal impact of suspending elective bariatric surgery and explore patient views in response to the reintroduction of elective working.
Methods
Study Design
This was a cross-sectional study conducted as an online survey using Google Forms between July 20, 2020, and July 31, 2020, in our tertiary bariatric unit. An anonymous questionnaire was designed in conjunction with bariatric surgeons and specialist nurses. It contained a series of closed and open questions focussing on the primary end points, including the physical and the psychological impacts of the pandemic on the patients and their views and perspectives on undergoing surgery during this time. A “free text” comment box which gave patients an opportunity to share additional concerns not covered by the closed questions, was also included (Online Appendix 1).
Participants
All patients listed for primary and revisional bariatric surgery at our unit before the suspension of elective services on March 23, 2020, were invited to participate. The questionnaire was distributed electronically as a URL link, along with an information letter, and in those who could not access the link, the survey was completed by going through the questionnaire over the phone.
Bariatric surgery had been postponed at the time the survey was conducted due to the COVID-19 pandemic. The survey was part of a broader service evaluation undertaken to ensure the safe reintroduction of bariatric surgery. Additionally, to plan our service in case of subsequent “surges” of the pandemic, it was considered pertinent to understand the impacts of the postponement of bariatric surgery had on the patients, and their choices if they were offered surgery.
Data Collection and Analysis
Data were collected and analyzed on Google Forms and Microsoft Excel. A descriptive analysis was undertaken of quantitative data which was presented as mean (standard error, SE), median (interquartile range, IQR) or percentage. Thematic analysis of the qualitative data was undertaken using Braun and Clarke’s 6 step framework (9). The comments were read and reread to familiarize with data and organized in a chart line-by-line by one researcher. “Codes” were identified from this organized handwritten data using an “inductive” approach. “Themes” were generated from recurring patterns of the codes. Themes were reviewed using a thematic map to ensure they depicted the contents of the comments accurately and were finally defined.
Results
Of the 147 eligible patients invited to participate in the survey, 71 (48.3%) responded and were included in the analysis. Demographics were available for 64 patients. Mean (SE) age was 50.3 (1.4) years, 52 (81.3%) were female. Mean (SE) BMI was 48.1 (1.1) kg/m2. Comorbidities, n (%), included hypertension (HTN) 28 (43.8), type 2 diabetes mellitus (T2D) 24 (37.5), ischemic heart disease 2 (3.1), obstructive sleep apnea (OSA) 36 (56.3), arthritis 36 (56.3), and preexisting anxiety or depression 28 (43.8). There were 61 (86.0) patients awaiting primary bariatric surgery, while remainder awaiting revisional surgery. Detailed responses to the survey are presented in Online Appendix 1.
Impacts of Suspending Surgery
Physical impacts
A median (IQR) weight gain of 4.7 kg (2.6-6.4) was observed in n (%) 48 (67.6) patients with 43 (60.6) unable to engage in more physical activity than normal (Figure 1) and 29 (40.8) unable to adhere to appropriate eating plans during the 4-month “lockdown” period (Figure 2).

Engagement in more physical activity than normal. Data represents n.

Eating habits during lockdown. Data represents n.
Psychological Impacts
The delay in bariatric surgery led to an adverse psychological impact in n (%) 53 (74.6) patients, versus 28 (43.8) presurvey (Figure 3). Although 37 (52.1) were concerned of acquiring COVID-19 infection during the early phase of the pandemic, 38 (53.5) however were now less fearful of contracting the infection.
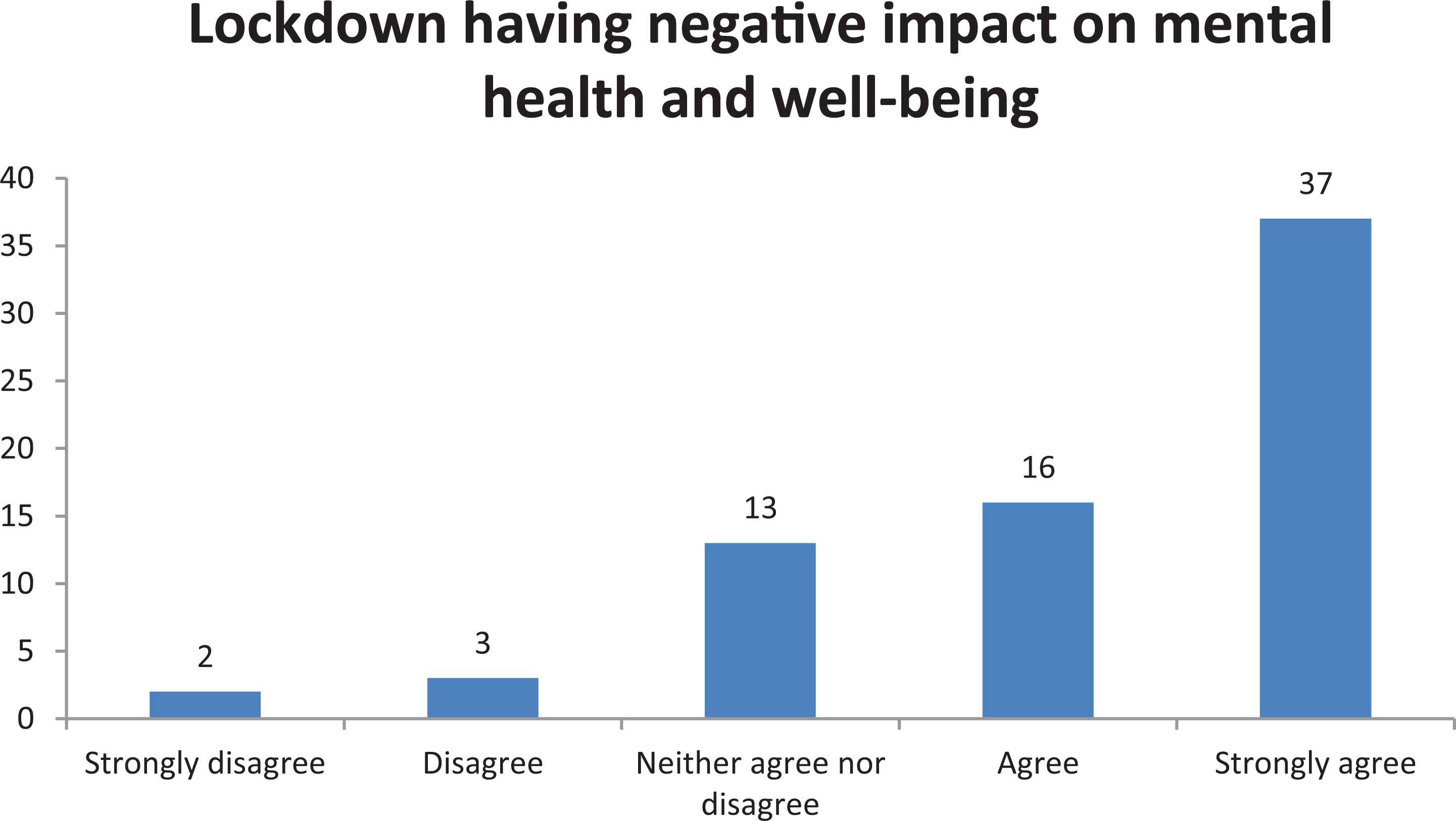
Impact of lockdown on mental health and well-being. Data represent n.
Perspectives on Restarting Elective Services
In total n (%), 66 (93.0) patients wanted to proceed with surgery (Figure 4), of whom 49 (69.0) were not concerned of acquiring in-hospital COVID-19 infection. The remaining 17 (23.9) although had concerns of nosocomial infection, still opted to proceed.

Patients wanting to proceed with surgery despite the pandemic. Data represents n.
Thematic Analysis
The following 4 themes emerged from the analysis of the 37 free-text comments: a) Postponement of secondary surgical procedures
One of the themes that emerged from the thematic analysis and observed in n (%) 11 (29.7) of the comments was postponement of other secondary procedures (Table 1) due to the delay in bariatric surgery.
Procedures Delayed Due to Postponed Bariatric Surgery in COVID-19 Pandemic.

“I can’t wait for surgery because I need a kidney transplant”,
“The delay has severely impacted on my life as I am awaiting hip surgery after having bariatric surgery, so the delay has caused more pain and distress for myself”.
Bariatric surgery acts as a bridge and enables patients to undergo other life-altering treatments once they have achieved clinically beneficial weight loss. Analysis of the comments demonstrated that delays in bariatric surgery have resulted in a detrimental impact on the quality of lives of patients, in particular those awaiting secondary procedures. b) Worsening mobility
Another theme that emerged from the qualitative analysis and observed in n (%) 11 (29.7) of the comments was worsening joint pains, poor mobility, and reduced ability to exercise. Individuals with morbid obesity often have joint pains and arthritis. Their inability to achieve clinically beneficial weight loss due to the delay in bariatric surgery, combined with lockdown measures and reduced opportunities to exercise, has compounded their symptoms: Even though there is a slight increase in my weight, it has had a significant impact on my mobility and osteoarthritis. The increase in my weight has restricted my mobility further and this has led to my mood being low.
c) Increased anxiety
The theme of increased anxiety was observed in n (%) 12 (32.4) comments. Patients felt extremely anxious during the pandemic, and the uncertainty of when they will be able to undergo bariatric surgery led to further worsening of their anxiety and mental well-being. I feel extremely anxious about COVID-19 and have had to have an increase in my anxiety meds due to lockdown, stress and anxiety. Not knowing when I am scheduled to have bariatric surgery is having a detrimental effect on my mental health and wellbeing.
d) Loss of support services
The uncertainty and lack of support secondary to the suspension of surgical, allied health professionals, and administrative services was observed in n (%) 9 (24.3) comments. Some of the patients have been waiting years to undergo bariatric surgery and suspension of bariatric services with no regular updates has led to further uncertainty. Analysis of other comments suggested that patients would benefit from online support and exercise classes, as lockdown measures had led to suspension of support groups and face-to-face sessions with the allied services. Really wish we could access exercise groups—happy to do online if someone professional is running it. The cancellation of my surgery was expected but there has been no support of any kind which leads to doubt and upset.
Discussion
To our knowledge, this is the first UK-based study examining the physical and psychological impacts of postponing bariatric surgery during the global pandemic, from the perspective of patients. Furthermore, this study has highlighted several unintended consequences such as delays in secondary treatments. More than two-thirds of patients gained weight during “lockdown” and almost three-quarters experienced increased anxiety. In their survey, Almandoz et al reported similar adverse outcomes as a result of “stay at home orders” in United States, which they attributed to finding less time to exercise and stress eating (10). Sisto et al similarly in their survey of 434 patients demonstrated increased psychological distress in patients awaiting bariatric surgery and increased frequency of snacking affecting their dietary compliance (11). A multidisciplinary team approach involving clinicians, dieticians, specialist nurses, psychologists, and support groups is often required to ensure patients remain motivated to achieve presurgery target weight loss. Loss of these support services, closure of facilities such as gyms and uncertainty about “the future” are likely contributing factors to increased anxiety levels, loss of motivation, poor adherence to dietary advice, and weight gain.
Our survey demonstrated that the majority of patients wanted to proceed with bariatric surgery and were not concerned about nosocomial COVID-19 infection. This position is in contrast with the survey conducted by Waledziak et al in Poland, who found only half of their surveyed population opting to proceed with surgery during the pandemic (12). Compared to their survey, our population was older (50.3 vs 39.0 years), had a higher BMI (48.1 vs 34.2 kg/m2) and worse prevalence of metabolic comorbidities (T2D 37.5% vs 11.6%, HTN 43.8% vs 33.1%, OSA 56.3% vs 7.8%, arthritis 56.3% vs 34.0%), which may explain their stronger desire to proceed with surgery. Furthermore, our thematic analysis suggested that delays in subsequent procedures, physical distress due to weight gain and poor mobility, reduced ability to exercise, and increased anxiety with mental distress may have contributed to patients remaining keen to proceed with surgery. The strength of feeling and the degree to which our UK patient cohort wished to proceed with surgery must also be considered in the context that confirmed COVID-19 cases and associated mortality is 5 and 20 times more than that in Poland, respectively. Furthermore, the incidence of COVID-19 in North-West local population is the highest in the United Kingdom, and at the time of writing, has seen subsequent surges.
In light of guidelines published by International Federation for the Surgery of Obesity and Metabolic Disorders on the recommencement of elective bariatric surgery (13), our study provides an important perspective from a key stakeholder group. Bariatric surgery during the pandemic can be reintroduced safely (14) and is “medically necessary time-sensitive” surgery, rather than “elective” (15). The results from an international collaboration examining the safety of bariatric surgery (GENEVA) during the pandemic are shown to be similar to prepandemic levels (16).
The broader evaluation in response to the ever-changing COVID-19 pandemic has led to the remodeling of bariatric services in our unit. Monthly support groups for both pre and postoperative patients are now conducted virtually by the bariatric specialist nurse and allied health professionals such as dietitians. Patients awaiting surgery are kept regularly updated, while extra support is provided to individuals who have gained weight. The Federation of Surgical Speciality Associations clinical guide to surgical prioritization during coronavirus pandemic (17) was introduced to prioritize clinically urgent cases. Precautions to reduce the risk of COVID-19 such as preoperative swabbing, 2 weeks of strict preoperative isolation and postoperative care in non-COVID operating theatres and wards is carried out as per the British Obesity and Metabolic Surgery Society guidelines (18).
Limitations
We acknowledge that our study has relied on a nonvalidated survey to assess the physical and psychological impacts on patients. The strength of the survey may have been improved had patient representatives been involved in the design and management of the study, or if the sample had included families and carers who also hold important perspectives. Our response rate was 50%, likely due to a relatively short window during which patients could respond. We acknowledge that although the demographics of the included patients may represent the population awaiting surgery in the UK NHS setting, this may not be more widely representative. Furthermore, the survey was conducted during the first wave of the pandemic since which much time has passed and subsequent waves have occurred. It is possible that patients’ perspectives may have changed with time and the ever-changing COVID-19 pandemic. A further validated survey may help to understand any such changes. The findings of this study should therefore be considered in the context of these limitations.
Conclusion
Postponement of bariatric surgery during the COVID-19 pandemic has had deleterious physical and psychological impacts on patients. The majority of patients are not concerned about acquiring nosocomial COVID infection and wish to proceed with their bariatric surgery. This is an important consideration for services as they plan for the reintroduction of elective programs.
Supplemental Material
Supplemental Material, sj-docx-1-jpx-10.1177_23743735211008282 - Serious Impacts of Postponing Bariatric Surgery as a Result of the COVID-19 Pandemic: The Patient Perspective
Supplemental Material, sj-docx-1-jpx-10.1177_23743735211008282 for Serious Impacts of Postponing Bariatric Surgery as a Result of the COVID-19 Pandemic: The Patient Perspective by Babur Ahmed, Mohammad Altarawni, Jodi Ellison and Bilal H Alkhaffaf in Journal of Patient Experience
Footnotes
Authors’ Note
This anonymous survey was undertaken as part of a service review in preparation for the reintroduction of elective bariatric services. Participants were invited to take part and not under obligation to complete the survey. Consent was assumed by participants completing the survey. This article does not contain any studies with human or animal subjects.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.