
Abstract
Patient-physician communication has the potential to improve outcomes and satisfaction through the shared decision-making process (SDM). This study aims to assess the relationship between perception of SDM and demographic, clinical, and patient-reported outcomes in patients undergoing Hallux Valgus (HV) correction. A prospective analysis of 306 patients scheduled for HV surgery was completed. The CollaboRATE score was used to measure SDM. Multivariable linear regression model was used to assess whether SDM scores were associated with preoperative characteristics or postoperative outcome scores. The mean CollaboRATE score was 2.9 (SD 0.9) and did not differ by age, socioeconomic status, or sex. Lower CollaboRATE scores were associated with more symptoms of depression, lower socioeconomic status, and lower general health scores (p-value < 0.05). There was no association between SDM scores and postoperative outcome scores. In this study, patients with depressive symptoms and lower socioeconomic status had worse perceptions of SDM. There was no difference in postoperative outcomes among participants based on SDM scores.
Key Points
In the context of elective Hallux Valgus correction surgery, depression, poor health, and lower socioeconomic status were associated with worse perceived shared decision making with clinicians.
There was no association found between pre-operative shared decision-making scores and post-operative outcomes for elective hallux valgus correction surgery.
Careful attention and discussion with patients who have concomitant depression symptoms and are of lower SES should be considered during orthopaedic consultation to improve the SDM process.
Introduction
Hallux valgus (HV) is one of the most common deformities of the forefoot, with prevalence estimates between 23% and 35% of adults affected, the majority of which are female.1,2 Discomfort, pain, impaired mobility, and reduction in quality of life are all symptoms associated with this condition.2-4 Given the spectrum of severity of the disease, an array of surgical techniques is used to treat HV, from simple bunionectomy to osteotomy and fusion. Research has shown that these surgical treatments achieve improved outcomes for patients’ pain and mobility.5-7
Given the variety of treatment options available for HV correction, a detailed discussion and a collaborative plan for management must be obtained. Patient-physician communication has the potential to improve outcomes and satisfaction through the shared decision-making process (SDM).8-10 SDM emphasizes the importance of information exchange between the physician and patient, the alternatives to treatment, risks, and benefits are discussed. The exchange offers the treating surgeon insights into patients’ values and then a mutual decision for management is considered together. 11 The concept of SDM has been applied and studied in orthopaedics but a paucity of literature exists for the role of SDM and HV surgical management.
To evaluate how patients perceive SDM in a clinical encounter there have been instruments developed to measure the impact and quality of the SDM process. These instruments are used to measure patients’ perceptions of the SDM process in a variety of clinical scenarios, including orthopaedic surgical decision making. The CollaboRATE measure is a brief three question survey which recalls the perceived SDM of the most recent encounter and is easily completed after a clinical encounter. 12 It is used primarily to assesses patients’ perceptions of their decision-making through understanding of their health issue, their treatment preferences and integration of their preferences into their treatment, important aspects of shared decision making.13,14 The CollaboRATE instrument has been used in a variety of clinical settings and demonstrated a strong ability to evaluate SDM in diverse patient populations given that is not specific to one condition. 15
In this study, the CollaboRATE instrument was chosen to measure the perception of the SDM process of patients undergoing consultations for elective HV correction by an orthopaedic surgeon. The objective of this study is to establish whether there is an association between patients’ perception of the SDM process at time of initial HV consultation and demographic, clinical, and socioeconomic variables. Second, to understand whether SDM was associated with patient's health-related quality of life after HV surgery.
Materials and Methods
Study Design
This prospectively recruited observational study from a single surgical centre in Vancouver, Canada contacted participants to collect clinical and patient reported outcome data on foot and ankle surgical procedures. Consecutive eligible patients between September 2016 and June 2020 of four orthopaedic surgeons with sub-specialty interest in foot and ankle surgery were contacted and enrolled within two weeks of being registered for elective HV surgery. Eligible patients were 18 years of age or older, had a fixed address, and were able to communicate in English.
Patients who had failed shoe wear and activity modifications and had a painful first metatarsal phalangeal joint were indicated for surgical management. The most common operative technique was the Lapidus technique (1st tarsometatarsal fusion, with 1st metatarsophalangeal medial eminence resection, and soft tissue rebalancing) with or without lesser toe correction.
Participants were asked to complete a survey package within two weeks of their surgical booking consisting of several patient-reported outcomes (PROs) and demographic information. The initial survey also included the CollaboRATE instrument, which is a measure of SDM between surgeon and participant. The same cohort was then contacted six months after their HV correction surgery and asked to complete the same PROs excluding the CollaboRATE score. Participants were able to complete their survey package online or on paper and were contacted up to two times to remind them to complete their PROs.
Socio-economic Status
Participants’ PROs were linked with two measures of neighborhood-level socio-economic status (SES), generated independent of this study published by Statistics Canada and known as the Canadian Index of Multiple Deprivation (CIMD). 16 The ethnocultural composition index measures the neighborhood level proportion of the residents that self-identify as a visible minority, are foreign born, have no knowledge of either official language (English or French), and are recent immigrants (arrived in the 5 years prior to the census data collection). This is reported as quintiles from ‘least diverse’ (Q1) to ‘most diverse’ (Q5). The situational vulnerability index measures the neighborhood level proportion of residents that are low income, aged between 25 and 64 years, are without a high school diploma, are in a single parent family, self-identify as Aboriginal, and the proportion of dwellings needing major repair. Which is reported as quintiles from ‘least vulnerable’ to ‘most vulnerable’.
Shared Decision-making
The CollaboRATE instrument was used to determine participants’ perceptions of the SDM process for HV correction. The instrument assesses three aspects of SDM between the clinician and patient: the effort made to explain health issues to the patient, the effort made to elicit patients’ preferences and the effort made to integrate patients’ preferences into clinical decisions.13,14 The version of the instrument used in this study has three items, each item ranging between 0 (i.e., ‘No effort was made [to communicate]’) and 4 (i.e., ‘Every effort was made [to communicate]’). The three items are averaged to create a single score. Higher scores correspond with more positive perceptions of clinician–patient communication. This instrument has been shown to have discriminative validity, and good intra-rater reliability in psychometric studies. 13
Patient Reported Outcomes
The Patient Health Questionnaire-9 (PHQ-9) is a nine-item instrument used to measure symptoms of depression. The instrument's items were each scored on a 4-point scale ranging from 0, meaning ‘Not bothered at all,’ to 3 meaning ‘Bothered nearly every day’. The instrument's score is the sum of the item values and lower values correspond with having fewer symptoms of depression.17,18
The Pain, Enjoyment of Life and General Activity (PEG) is a three-item instrument that evaluates pain intensity, interference with enjoyment, and general activity. Each item's values range between 0 which means “no pain” and 10 which means “pain as bad as you can imagine”. The instrument's score is the average of the three items with higher scores denoting worse pain. 19 Health status was measured using the Euro-QoL's EQ-5D (5L) which includes a visual analog scale (VAS) measuring overall current health status. 20
The Foot and Ankle Outcome Score (FAOS) is an instrument that measures five subscales: pain, other symptoms, activities of daily living, sport and recreation function, and quality of life (QOL) subscales.21,22 Previous work has demonstrated that the sport and recreation subscale was not responsive and this subscale was excluded in this study to reduce the likelihood of spurious findings. 22 Each item's values range between 0 meaning ‘no symptoms’ and 5 meaning ‘extreme symptoms’. Following convention for this instrument, the subscales were each converted to a score that ranged between 0 and 100, where higher scores were associated with better function or symptoms.21-23
Statistical Analysis
All demographic, socioeconomic and PRO scores were summarized using summary statistics. Age was categorized into four groups for presentation. Ethnocultural composition and situational vulnerability were reported by quintile but collapsed in regression analyses if <10% of the cohort were in an individual quintile. Differences between all participants and those who had undergone surgical intervention were tested using simple summary statistics. Statistical significance was set at p < 0.05 for a two-tailed test. P-values were not adjusted for multiple comparisons since this was an exploratory study.
Summary statistics of participant's CollaboRATE scores were calculated for all age categories, SES dimensions, treating surgeon, and sex. Differences in CollaboRATE values between demographic and socioeconomic factors were measured using analysis of variance (ANOVA) methods. Preoperative and postoperative PRO scores were compared using paired t-tests.
To measure whether participants’ characteristics were associated with their perceptions of the SDM process a multivariable linear regression model was used. The model adjusted for participants’ age group, sex, ethnocultural and situational vulnerability, and baseline PRO values.
To measure whether participants’ preoperative perceptions of their SDM were associated with their self-reported symptoms six months following HV correction, multivariable linear regression models were used. Separate regression models were created for each domain of the post-operative FAOS score as the dependent variable; independent variables included participants’ age group, sex, ethnocultural composition and situational vulnerability (which were collapsed as there were few participants in the two lowest SES categories quintiles), and baseline PRO values.
Missing data was assumed to be missing at random (MAR) and incorporated using multiple imputations. 24 The fit of the regression models was assessed through visual examination of residual plots. All regression variables were retained irrespective of their statistical significance. Regression coefficients, their standard deviations and p-values were reported. This study was approved by the Behavioural Research Ethics Board of the University of British Columbia (REB#: H22-01846).
Results
A total of 306 participants were identified as having been booked for HV correction by one of four surgeons and completed baseline questionnaires including demographic information, PRO's and CollaboRATE scores. Of those 107 (35.0%) participants had undergone the HV correction procedure and had 6-month follow-up PRO data complete at the time of data extraction. In total, 84.9% of participants were female and the average age was 57.1 years old (SD = 11.8) with only 12.4% over the age of 70. As shown in Table 1, there were no differences in age, sex, or SES between all participants and those who had reached the 6-month follow-up PROs collection time point.
Summary Presentation of Demographic, Socioeconomic, and Baseline PRO Data.

Preoperative FAOS and CollaboRATE scores did not differ among age groups, sex, or SES categories, except for the FAOS QoL subscale that demonstrated higher scores (better QoL) among participants in the older age groups (p < 0.05). There were no differences in CollaboRATE scores among participating surgeons.
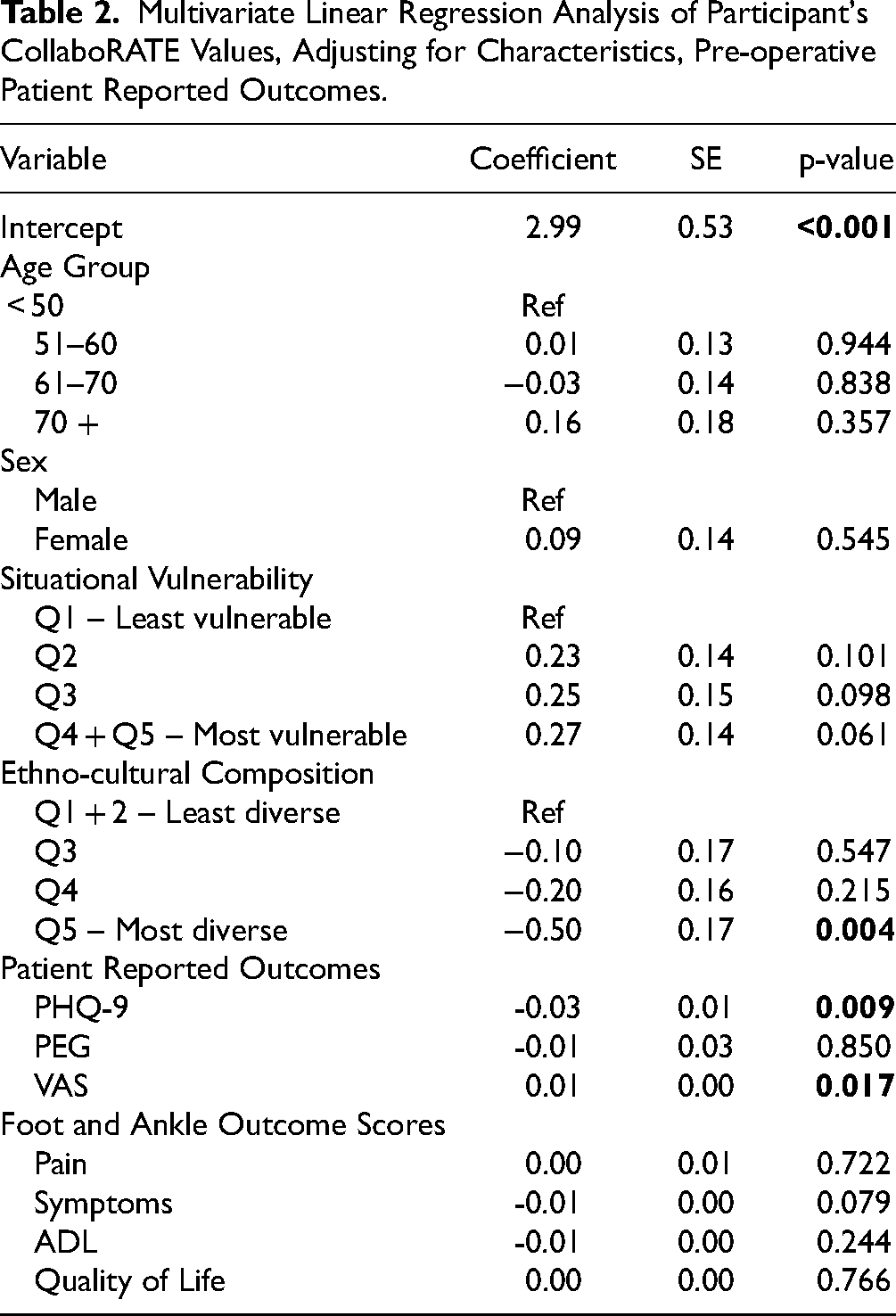
The preoperative regression analysis found a relationship between CollaboRATE scores and PHQ-9 scores. Participants reporting more symptoms of depression reported lower CollaboRATE scores (p < 0.005). Also, higher EQ-5D VAS scores (better overall health) were associated with a higher CollaboRATE score (p = 0.017). Finally, compared to the lowest ethnocultural composition quintile, participants in the highest quintile (more diversity) had lower CollaboRATE scores (p = 0.004). There were no associations found between CollaboRATE scores and age, sex, baseline FAOS scores or the situational vulnerability index as shown in Table 2.
Multivariate Linear Regression Analysis of Participant's CollaboRATE Values, Adjusting for Characteristics, Pre-operative Patient Reported Outcomes.
For those participants who had reached 6-month follow-up all domains of health measured by PROs demonstrated improvements between preoperative scores and postoperative scores (p < 0.05) with the exception of PHQ-9 score (symptoms of depression) which did not show statistically significant change (4.1 vs. 3.9; p = 0.428). See Table 3 for details.
Patient Reported Outcome at Baseline and 6 Months Postoperatively for Surgical Patients.

Finally, multivariable linear regression analyses of postoperative PRO's score found no association across all FAOS subscales (pain, symptoms, ADL, and QoL subscales) with participant's CollaboRATE score, and no differences found in outcomes for sex, or SES. Results are shown in Table 4.
Multivariate Linear Regression of Postoperative Foot and Ankle Outcome Scores, Adjusting for pre-operative PROs, Demographics, and CollaboRATE Scores.

Discussion
This study found that participants’ perceptions of the SDM process in the setting of elective bunion surgery were affected by depressive symptoms, general health and SES. Participants reporting worse symptoms of depression, lower general health, and those in more diverse ethnocultural compositions (higher quintile) reported perceiving less involvement in the decision making around elective HV surgery. This relationship, however, did not extend to functional postoperative outcomes, as measured by the FAOS score.
One of the key findings of this study was that more severe symptoms of depression and lower general health were associated with a perceived lack of engagement in SDM by patients undergoing elective HV surgery. SDM relies on the patient-physician interaction which can be impacted by mental health disorders and has been studied in the setting of non-elective surgeries such as cancer.25-27 Mental health disorders can lead to discordant expectations of surgical management between surgeons and patients and impact the SDM process. 27 In a recent study by MacMahon et al., 28 patients had different expectations of foot and ankle procedures compared to surgeons if they had worse baseline mental health scores. 28 In a complementary study among colorectal surgery patients, CollaboRATE scores were lower among patients with higher baseline depression scores. 29 However, there has been a paucity of literature evaluating the role of depression on SDM in elective orthopaedic procedures and what impact it can have on health outcomes. This may indicate a role for a mental health evaluation in the elective surgical consultation to improve understanding and the SDM process.
This study found that participants who had a more diverse ethnocultural composition status on average have lower perceptions of the SDM process. Similar findings have been addressed in existing literature where disparity in the quality of the SDM process for different socioeconomic groups is evident, citing that those with lower socioeconomic status often have poor interactions and less trust with health care providers.30,31 A recent review, however, demonstrated that in over half of studies examining the role of socioeconomic factors on the SDM process, there was no significant associations. 32 There was no association between the CollaboRATE score and the situational vulnerability indices. Awareness of these disparities may help better inform the treating surgeon on how to alter their communication approach with different groups to improve the SDM process. There are several interventions that aid in the SDM process, and a recent review has identified that these can help to improve patient outcomes for socially disadvantaged individuals for conditions including surgical procedures. 33 Further research is needed to evaluate the role that socioeconomic status can have on the decision-making process in HV correction surgery.
To our knowledge, there has been no other published research that has evaluated the role of SDM in HV surgery outcomes. We found no evidence that higher preoperative SDM scores had an impact on postoperative self-reported outcomes in HV correction surgery at six months follow up. This finding was somewhat surprising given that participating in SDM during the consent process is a fundamental teaching dogma for clinicians across all specialities. 34 There is evidence in the orthopaedic literature that better SDM is associated with improved postoperative PROs, a recent study by Chrenka et al., 35 found that patients undergoing total joint arthroplasty with higher pre-operative SDM scores (using the CollaboRATE instrument) led to better functional outcomes and higher patient satisfaction scores. 35 Further, a study by Sepucha et al., 10 concluded that those who perceived better pre-operative SDM experienced better postoperative quality of life, higher satisfaction, and less regret when undergoing elective surgeries for hip and knee arthroplasty, spinal stenosis or disc herniations using a derived score from condition specific knowledge. 10 It is possible that outcome measures related to HV correction may not reflect the impact of SDM processes on patient outcomes. A more relevant measure of SDM may include the patient experience in the postoperative period such as patient expectations and satisfaction with surgery.2,6,7 Further, it has been demonstrated that orthopaedic procedures which have more variation in post-operative clinical outcomes (such as total knee replacement and spine surgery) are more likely to show that the SDM process has a greater impact on both satisfaction and clinical outcomes when compared to procedures that have overall better clinical outcomes (such as total hip arthroplasty). 36 Given that HV correction has high clinical satisfaction and overall good outcomes it may be less responsive to changes in the SDM process as measured by the CollaboRATE instrument.
There are several limitations to this paper, the first being that this is a single centre study of four surgeons in a group foot and ankle surgical practice, where residents and fellow training occurs. This aspect of the study's design may result in similar practice styles and surgical decision making that leads to similar SDM discussions between surgeons and patients. Consideration should be given to multi-centre studies with greater practice variation to evaluate the impact of SDM on clinical outcomes in different settings. Second, patients’ perceptions of the SDM process were captured in this study by using the CollaboRATE tool but no qualitative assessment of the clinical encounter was used to identify other communication techniques used by the surgeon to facilitate patient's involvement in the decision-making process. Further, the surgeon's perspective regarding the SDM process was not evaluated at the same encounter making it difficult to comment on the physician-patient interaction. Future research is required to evaluate the correlation between clinician and patient with regard to SDM and whether this impacts outcomes, satisfaction, and other metrics of surgical success using both quantitative and qualitative methods. Finally, patients were excluded from this study if they were non-English speaking, possibly excluding patients with lower SES scores or differing cultural perceptions of the SDM process. Further work is needed to be able to include these patients in research on SDM in elective surgical outcomes.
Conclusions
In this study, participants with greater symptoms of depression, lower general health, and residing in neighborhoods with higher proportions of visible minorities or recent immigrants were found to have lower perceptions of the SDM process for HV surgery. Further, there was no association found between perceived SDM and postoperative outcomes. In orthopaedic consultation for HV correction, careful attention and discussion with patients who have concomitant depression symptoms and are of lower SES should be considered to improve the SDM process. Further research is needed in the foot and ankle literature to evaluate the role of SDM in patient reported outcomes and how tools or decision aids can be used to improve the SDM process.
Footnotes
Conflict of Interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Ethics approval for this study was obtained by the Behavioural Research Ethics Board of the University of British Columbia (REB#: H22-01846).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded through in-kind contributions by Vancouver Coastal Health Authority (VCH) and Providence Health Care (PHC; Vancouver, Canada). VCH and PHC had no role in the study design, data collection, statistical analyses or interpretation. There are no other funders.