
Abstract
Patient experience is globally recognized as an important indicator of health system performance, linked to health system quality and improving patient outcomes. Post COVID-19, health systems have embraced digital health and advanced digital transformation efforts; however, the relationship between digital health and patient experience outcomes is not well-documented. Using HCAHPS hospital survey data to measure patient experience, and HIMSS EMRAM Maturity Model data to measure digital maturity, a cross-sectional design using multivariate analyses examined the impact of digital maturity on patient experience in US hospitals. Our analysis shows that advanced digital maturity in US hospitals is associated with stronger patient experience outcomes, particularly relative to communication with nurses, doctors, and communication about medicines and therapies. The findings suggest that there are significant differences in patient experience associated with teaching versus nonteaching hospitals, urban versus rural hospitals. As hospitals advance and progress digital transformation initiatives, evidence to inform how transformation efforts can engage and advance patient experience will contribute to health system performance well into the future.
Introduction
Patient experience is globally recognized as an important indicator of health system performance, linked to both quality and improved patient outcomes.1–3 Endorsed by the World Health Organization, 4 healthcare systems are now prioritizing patient experience, with the goal of advancing “patient centered care” to ensure patients are at the center of care delivery.
However, despite the importance of patient experience, both scholars and healthcare systems have struggled to define the relationship between patient experience and clinical effectiveness outcomes.1,5–7 Many scholars suggest that digital health is a way to improve both patient experience(8) and clinical outcomes.9–11 However, evidence remains limited regarding the role of digital health in advancing patient experience, with some research suggesting that digital health advances may not necessarily result in effectively meeting patient needs. 12
As digital health transformation continues to progress in the post pandemic era, it is of paramount importance to more fully understand and document how patient experience is influenced by advances in digital transformation. Specifically, the role of digital maturity and how it influences patient experience is critical to understanding how digital health transformation efforts can strengthen and advance patient experience as well as health system performance.12,13
Patient experience measures have evolved over that past 2 decades, where historically patient experience measures focused on satisfaction with care and patient adherence to treatment protocols. Historically, there has been less attention to whether care delivery was meeting the needs of the patient. 2 The term “patient experience” was used to describe the patient's experience with clinical care including patient satisfaction with their care, 14 and patient adherence to prescribed care pathways.15–18 Historically, patient experience measures viewed patients as recipients of care, with compliance with prescribed therapies was a central feature of these measures. 19
More recently, patient experience measures have been conceptualized from the patient perspective, focused on meeting patient needs and how healthcare delivery contributes to patient experience.1,3,4,6,20 It is well-documented that patients value meaningful relationships with their provider teams and these relationships are central to the context of their care experiences.1,2 Patient experience measures have changed to focus more on relationships with care providers that recognize patients as individuals with unique life circumstances and health needs that extend well beyond their clinical diagnosis or health status. 19 Patient experience measures are progressing toward examining experience from the perspective of the whole person, whereby patients are viewed as partners in their health and care, are supported by meaningful relationships with provider teams. 6
A conceptual analysis of current patient experience literature revealed 3 prominent components of patient experience; namely, (1) the focus on the relationship between patient and clinicians;1,3,4,6,20 (2) patient health needs which include services and supportive care that reaches beyond traditional or formal healthcare services21,22; and, (3) the need for patients to have autonomy and control over care decisions to ensure care is individualized and tailored to the unique needs of every individual.2,3,6 To date, patient experience measures and concepts have not fully examined the impact or relationship between digitally enabled care delivery (eg, digital health) and patient experience.
Digital health transformation in health systems has accelerated rapidly since the COVID-19 pandemic. 23 Health systems have adopted a wide range of digital health technologies, wearable devices, and telemedicine models of care to facilitate access to healthcare services while managing heightened demand for care due to COVID19 infections. 24 Rapid adoption of telemedicine and other digital services required policies and operational strategies to manage the surge in demand for healthcare services. 21 Currently, health systems continue to advance these digital health transformation efforts to strengthen system capacity to meet growing demands for care reduce cost and strengthen quality and safety performance.4,10,11 However, the accelerated pace of digital transformation has now created an urgency to examine how digitally enabled care delivery impacts and influences patient experience, particularly given heightened complexity of care needs evident in the post pandemic era. 25 A growing number of digital tools in the consumer market offer patients a more flexible, and potentially cost-effective approach to managing health and care to meet consumer health needs. 26 Patients are able to manage their health and care, determine health goals, and use these digital tools to track their progress toward health and wellness goals.6,20,24,27
The role of “patient” is now transitioning toward self-management, characterized by control over managing their health care and much greater autonomy over making personal health decisions.28,29 Digital technologies may empower patients by enabling greater control over their care (eg, capacity to access information, health data, and scheduling) offering tools to independently assess and track progress toward health goals. 27 Consumer health technologies generate large data sets which enable advanced analytics to inform consumer health decisions and offer more personalized and predictive tools that provide data-driven insights. 30 Experiences of having to manage their health and care during the pandemic, supported by the rapid acceleration of digital technologies in the consumer market now present health systems with an opportunity to integrate digital tools and technologies into care delivery models and approaches that enable meaningful connectivity and person-centric relationships between patients and providers.12,22,27
To date, health systems are advancing digital transformation efforts; however, it is unclear how digital tools and technologies have, or hold the potential to, advance and strengthen patient experience. The purpose of this study is to examine the relationship between digital maturity as a measure of digital transformation in US hospitals and patient experience outcomes. Specifically, this research will examine the relationship between digital maturity and key dimensions of patient experience for the purpose of creating evidence of how, and the degree to which, digital transformation influences patient experience.
Methodology
A cross-sectional design using multivariate analyses accessed 2 data sets to examine the impact of digital maturity on patient experience in US hospitals. HCAHPS star ratings reported in 2021 was accessed from the Centre for Medicare and Medicaid Services for this analysis.
31
HCAHPS
Data from the HIMSS electronic medical record (EMR) assessment model were the second data set accessed for this analysis, as a measure of digital maturity in US hospitals. Hospitals complete online EMRAM survey of over 200 indicator statements which measure digital health dimensions such as health information exchange, clinician adoption of EMR, data privacy and security, and governance. An embedded algorithm generates a maturity level score on a 7-point scale of one through 7, which are described in Table 1. Hospitals that do not meet minimum EMRAM requirements are scored at level 0 maturity. Indicator requirements for hospitals to meet level 1 maturity include integration of lab, pharmacy, diagnostic imaging, and cardiology information systems, and resilience management systems such as ancillary systems in the event of a disruption. A detailed assessment of EMRAM maturity levels is provided to each hospital completing the EMRAM assessment. Hospitals which achieve maturity levels of 6 or 7 are further validated by an onsite assessment by the HIMSS team. Hospitals which have achieved level 6 or 7 maturity are validated for achievement of indicator requirements which include patient experience, data exchange, adoption of digital technologies, resilience of information systems, and governance. For this analysis, we focused only on hospitals at maturity levels of 0, 6, or 7. Stage 0 hospitals were classified as low digital maturity and hospitals validated at stage 6 and 7 level of maturity were classified as having high digital maturity for this analysis. Hospital HCAHPS star rating data were matched with hospitals with completed EMRAM assessment data, using the CMS hospital Identification number, and hospital data in the HIMSS's dataset.
Description of the EMRAM Stages of Digital Maturity.

A total sample of 2362 hospitals with complete EMRAM maturity data were linked with HCHAPS star rating data. The majority of the hospitals were either acute care or critical access hospitals, 57.3% and 41.1%, respectively. HCAPS star ratings are only reported for hospitals that have a minimum of 100 completed surveys per year. Critical access hospitals were more likely to be reported as “not available” star ratings for the HCAPS, with only 15% of critical access hospitals having HCAHPS data available, resulting in critical access hospitals being excluded from the analysis. Inclusion criteria for this analysis were acute care hospitals that provide emergency services, report their bed size categories, have available HCAPS star ratings data, and have complete EMRAM maturity level assessments. Based on the inclusion criteria for this study, 1048 hospitals were included in this analysis.
Hospital demographics are presented descriptively using mean, standard deviation, or percentages wherever appropriate. The multivariate analysis aimed to examine EMRAM maturity level assessed for hospitals for the probability of attaining a given number of stars or higher in HCAPS's ratings. A cumulative logit strategy was used to manage outcomes that are multicategory in which the categories are ordered from lowest to the highest. This regression used EMRAM maturity levels (Low = 0 and High = 6, 7) as a predictor variable while adjusting for all hospital characteristics (eg, number of beds, teaching/nonteaching, urban/rural, ownership) and their interactions with the EMRAM maturity levels. The interaction factors were included to check whether or not the impact of digital maturity depended on the subgroups such as hospitals with small number of beds, hospitals in urban or rural settings, or teaching hospitals. A stepwise model selection approach was employed to select the set of factors that (eg, both EMRAM and hospital characteristics) that best predict the probability of star ratings. A separate model was created for each of the 10 measures of patient experience, and the results are presented as odds ratios and their 95% confidence intervals.
Results
The demographic characteristics of the hospitals in this study are summarized in Table 2.
Summary Demographics of Hospitals.

Demographic analysis included the number of beds to examine variation in digital maturity and patient experience in small, medium, and large hospitals.
Of the total sample of n = 1048, 246 (23.5%) had EMRAM maturity of levels 6 or 7. Hospital size measured by bed size categories, included large (56%), medium (24%), and small (20%) sized hospitals. Teaching hospitals constituted 58.9% (n = 617) of the total sample, with 57.3% of the large hospitals (n = 600) located in urban areas. The majority of hospitals, 64.7% (n = 678), in this analysis, were reported as not-for-profit ownership status, 21.7% (227) were reported as proprietary (privately owned), while 13.6% (n = 143) were government owned. The majority of the hospitals were reported as referral hospitals, 74.7% (N = 783).
Figure 1 reports the odds ratios of high EMRAM maturity hospitals compared to Low EMRAM hospitals in achieving higher star ratings for each of the 10 measures of patient experience. The odds of higher patient experience ratings are 1.8 to 2.24 folds higher relative to patient experience with communication for hospitals with EMRAM 6 or 7 maturity, compared to hospitals at level 0 EMRAM maturity. This finding was consistent for all hospitals in the study, regardless of the size (eg, number of beds). A similar pattern of effect of digital maturity can be seen with respect to hospital environments, such as cleanliness and quietness ratings, which were, respectively, 1.3- and 1.4-fold higher in digitally mature hospitals (eg, EMRAM 6 or 7), for all hospitals in the study, regardless of the hospital size.

Impact of EMRAM digital maturity on the 10 areas of ratings included in this study.
The effect of digital maturity on patient experience with care transitions and staff responsiveness was similar to patients’ communication experiences; however, results varied with the size of the hospital. EMRAM maturity was a statistically significant predictor of higher star ratings for patients’ experiences with care transitions and staff responsiveness, but only in the case of large hospitals. Although not significant, the direction of the impact of digital maturity was similar for medium and small sized hospitals (Figure 1).
Each of the 10 models fitted to the 10 areas of ratings showed that, in addition to the digital maturity, some demographic factors have a significant impact on the odds of higher patient experience ratings. The effects of these demographic factors on the odds of higher ratings were consistent throughout the 10 models in the same direction and with almost the same magnitude of influence. The effects of demographic factors related to the overall patient experience ratings are illustrated in Figure 2. Specifically, hospitals in urban areas are less likely to have higher patient experience ratings compared to rural hospitals, who are statistically more likely to receive higher patient experience ratings (odds ratio [OR] = 0.61, 95% confidence interval [CI]: 0.46-0.80). Patients are also more likely to report higher experience ratings for Nonteaching hospitals compared to Teaching hospitals (OR = 1.7, 95% CI: 1.32-2.18). Ownership of hospitals also varied, whereby, government owned and Not-for-profit hospitals were similar, and had statistically significantly higher odds of receiving higher patient experience ratings compared to proprietary hospitals (Governmental vs Proprietary: OR = 2.96, 95% CI: 1.96-4.49; Nonprofit vs Proprietary: OR = 3.11, 95% CI: 2.26-4.26). Larger hospitals were associated with lower patient experience ratings (Appendix).
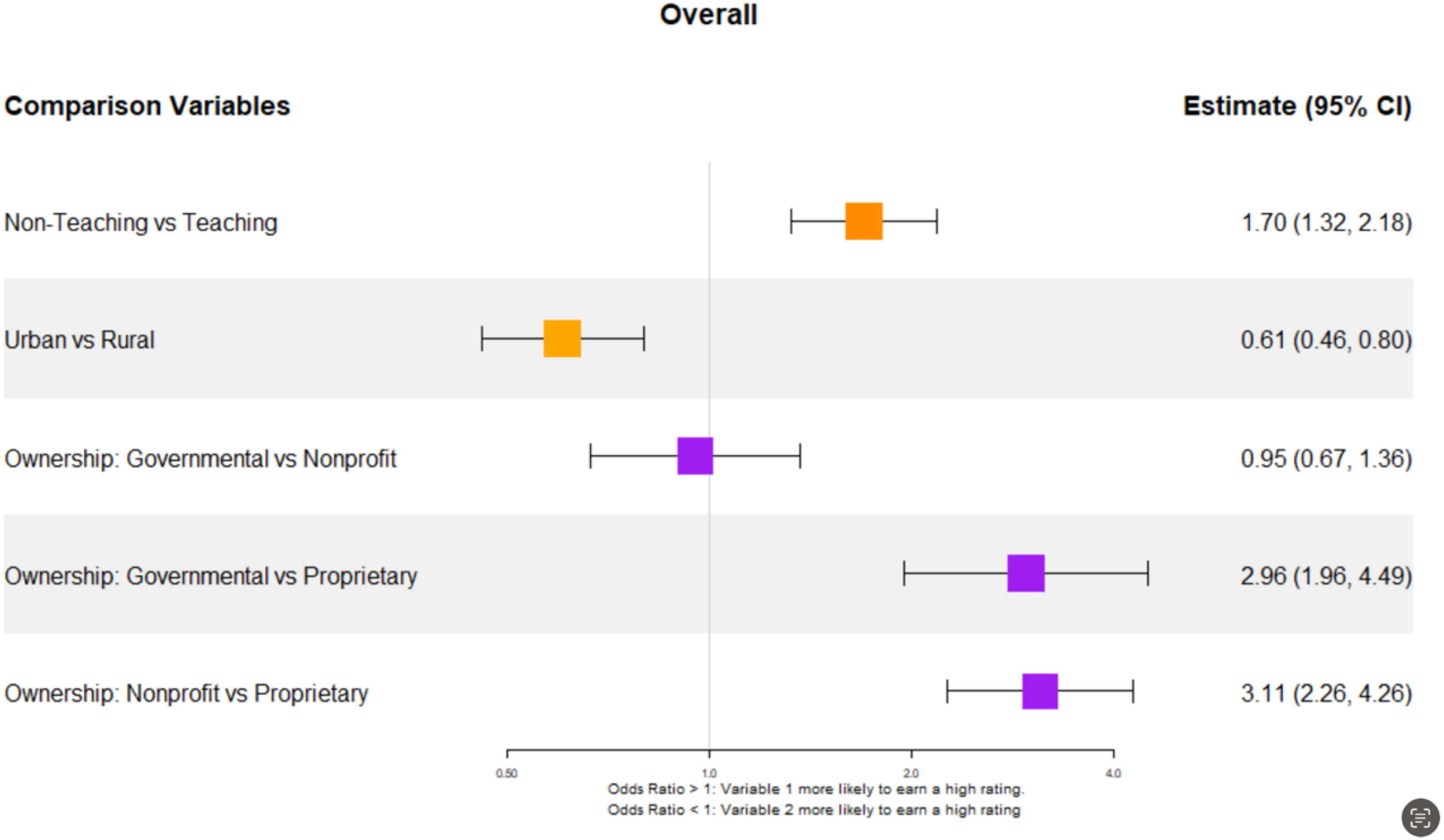
Impact of some hospital demographic factors on patient experience.
Discussion and Conclusion
This study provides evidence that advanced digital maturity in US hospitals is associated with significantly stronger patient experience outcomes, particularly relative to communication with nurses, doctors, and communication about medicines and therapies. Although many hospitals in the US have adopted EMR information systems, the majority (73%) of hospitals in this study remain at level 0 for digital maturity. For patients accessing care in hospitals at level 0 maturity, access to data regarding diagnostic tests (lab, imaging), and access to information about their medicines (pharmacy), has not been integrated into their patient record. Typically, patients can access their data through patient portals, however, when digital maturity is at level 0, patients are challenged by having to access multiple and different sources of data due to the lack of integration of pharmacy, lab, and imaging data into the EMR system. Communication about medicines, therapies, and discharge transitions in digitally mature hospitals (EMRAM level 6 or 7) more readily supports dynamic engagement with patients who can not only access their data and health information but can also access to digital tools to support self-management of their health and care. Research suggests that patient experience is an essential indicator of health system performance and patient outcomes in particular1,3,19; however, research has not yet examined how digitally advanced organizations vary relative to how patients communicate with doctors and nurses in hospitals, and how access to and use of data contribute to these stronger patient experience ratings. These findings suggest that advanced digital maturity in hospitals may offer patients greater access to their health data and information about therapies to support health literacy and to enable more informed discussions and decisions between clinicians and their patients. More timely receipt of information for patients may also be a factor that contributes to stronger scores on patients’ experience with responsiveness. Patient experience ratings were not as high in larger hospitals that tend to be more digitally advanced, teaching hospitals, or hospitals in urban centers which suggests that patient experience ratings vary with respect to demographic and geographic features of hospital settings which requires further investigation. As hospitals continue to advance digital transformation, these findings suggest that digital health may be a strategy to advance and strengthen the hospital's capacity to support patient experiences. For example, integration of digitally enabled tools into hospital care workflows to support patient centric care, with the support of clinician teams, may serve to enable and support patients to have greater engagement, autonomy, and control over health decisions, as partners in their care with clinician teams. The findings in this study are limited to examining patient experiences in 2021, when the US health system was experiencing significant challenges in managing the COVID19 pandemic, including workforce shortages and high demand for acute hospital care. Future research will be required to examine whether patient experience is significantly stronger in digitally mature organizations in the post pandemic years, in order to more fully examine causality of digital maturity on patient experience and better understand the role of digital maturity in advancing patient centric models of care in hospital settings.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241228931 - Supplemental material for Digital Maturity as a Strategy for Advancing Patient Experience in US Hospitals
Supplemental material, sj-docx-1-jpx-10.1177_23743735241228931 for Digital Maturity as a Strategy for Advancing Patient Experience in US Hospitals by Anne Snowdon, Abdulkadir Hussein, Ajetunmobi Olubisi and Alexandra Wright in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.