
Abstract
In response to the rise in mental disorders, psychosocial and community approaches have been proposed, complementing traditional clinical services. The present research aimed to understand the perception of individuals attending community-based strategies regarding mental health services as part of the approach to mental disorders in Colombia. Two workshops were conducted with 30 individuals with mental disorders (depression, anxiety and bipolar disorder), who were members of community strategies. A thematic analysis was conducted. The theme resulting from the analysis shows Community mental health within the healthcare system, which consisted of categories such as Group Amplifying Actions for Health and Groups as Complementary to Other Forms of Care. It is emphasized that the healthcare system should establish bridges with community mental health strategies and actively engage in their strengthening processes to enhance the outcomes of pharmacological interventions and even psychotherapeutic interventions. Bidirectional learning approach is proposed between community-based mental health services and clinical settings within the healthcare system. Community strategies can make an important contribution to complex processes in the health system.
Keywords
Introduction
Mental health has become a priority issue on global public health agendas and in the development of policies that involve multisectoral participation.1,2 Efforts to build socially and culturally appropriate, efficient and effective approaches in terms of resource investment and health outcomes in mental health are directed towards the path of strengthening the community based on strengths, consolidating networks in society and support for mutual aid processes. 3
There is a need to focus the objectives and context of these efforts to achieve a balance between disease management interventions, promotion and prevention through different community-based approaches.4,5 All of this must be done through the lens of public health and global mental health.6-8
The most forceful approaches currently are those that frame their clinical and collective actions in guaranteeing human rights for people with mental health problems. This has led to a gradual shift towards community-based models. 3 Community-based rehabilitation -CBR- adopts the principles of a more comprehensive approach to mental health. 9 It opposes the asylum model and aims to empower people in their relationships with others.
Although community actions in mental health are characterized by autonomy, it has been described that there are greater benefits in recovery when these actions are integrated with the sociopolitical context, in this case, the health sector. 10 These alliances provide meeting facilities, improve contracting mechanisms, strengthen public relations, improve communication of health needs, and exchange information and knowledge. 11 This has even made it possible to raise awareness among health professionals about the mental health approach and their participation in aspects of the quality of health care services.11,12
The most forceful approaches currently are those that frame their clinical and collective actions in guaranteeing human rights for people with mental health problems. This has led to a gradual shift towards community-based models. 3 Community-based rehabilitation -CBR- adopts the principles of a more comprehensive approach to mental health. 9 It opposes the asylum model and aims to empower people in their relationships with others. The positive effects of peer services have been shown to improve hope, quality of life, self-esteem, social inclusion, and commitment to improving services. 10 This last point, is especially given in a human rights framework. 10
In strengthening services, some authors point out11,13 the role of pharmacological treatment in CBR, since it seems that lower doses of medications may be sufficient to achieve therapeutic objectives in people who participate in programs based on community compared to hospital-based programs. In this regard, research indicates that non-adherence rates among people with mental disorders can reach up to 50%, 14 leading to significant personal and social costs. 15 In addition to improving medication adherence, 16 the alliance with community actions turns mental health strategies into opportunities to promote health rights, which leads to conventional medical and psychological treatments having better results.17-20
On the other hand, it has been described that these programs are not articulated with health systems, particularly in Latin American contexts.21-24 In fact, some authors have described that such partnerships may not be appropriate, and that community-based strategies work best when separated from the health system.22,25,26
The Present Study
The history of mental health recovery has evolved from an asylum perspective of mental health to the recognition of communities as fundamental to the recovery process. 9 However, in this theoretical journey both approaches have often been considered as opposites, without fully recognizing the benefits that come from the integration of the biomedical model with the social-community model. 8
Methods
Qualitative study, using thematic analysis to report the data. The interviews focused on a specific topic proposed by the researcher, with the objective of obtaining the attitudes, feelings, beliefs, experiences and reactions of the participants. 30 participants were selected from two peer support groups: 15 were selected from Red Expressarte, a support group located in Caldas, Colombia, made up of approximately 50 people, with community initiatives whose objective is psychoeducation, social entrepreneurship and the formation of networks. The average age of the participants is 31.06 years.
The other selected group was 15 participants from Amucam located in Risaralda, Caldas, a support group whose objective is to support women's entrepreneurship and mutual support, the average age of the participants is 36.6 years.
The selection of both groups was based on their national recognition in social innovation processes and the defense of the human rights of people with mental disorders. This took place at the headquarters of both groups in the last half of 2022.
Process
Data were collected through two focal groups, one for each association, with participants from these two community-based strategies. This took place in the environment in which each group normally operates. In the case of Amucam, it took place in a rural area, while with Red Expressarte, it occurred during a trade fair and a human rights promotion event run by them. During the session, questions were aligned to predetermined categories and a group conversation took place. 27 The interviews were recorded, the focus group was led by a close community psychiatrist who has had previous experience with both groups28,29 the data were analyzed by a community psychologist, without prior knowledge of the group, by a medical epidemiologist and by an expert doctor in primary care and community mental health without much knowledge of the group, but whose reflections on the data allowed the triangulation, construction and saturation of the categories.
As a focus group procedure, and as part of the checklist proposed by Escobar and Bonilla-Jimenez, the minutes were shared with both groups, writing the contributions in the analysis that each group had with the final results. 30 To ensure transparency and reliability, participants’ quotes were systematically organized into a matrix for categorization, forming themes based on the degree of saturation. The analysis concluded when no additional elements related to the objective of the study emerged.
Analysis
After completing this phase, the data was analyzed using thematic analysis. 31 However, it frequently goes further and interprets various aspects of the research topic. This method has the possibility of discovering themes and concepts contained throughout the interviews, which reaffirms the value of the people interviewed and, at the same time, the role of the researcher in identifying patterns or themes.
In the data collection stage, the immersion crystallization process was used, which includes reflexivity, that is, the subjectivity of the researcher is recognized, which influences the collection and analysis of data. In addition, patterns were identified and articulated during the analysis process.
Ethical Considerations
This study was adapted to the recommendations for biomedical research of the Declaration of Helsinki of the World Medical Association and was approved by the Ethics Committee of University of Manizales with act CB_022/2022. The names of the study participants were kept in strict confidentiality.
Results
Table 1 describes the characteristics of the participants in each group. The theme of Community Mental Health in the Healthcare System emerged from the analysis. This theme encompasses categories such as Amplifying actions of the group for health and Groups as Complementary to Other Forms of Care.
Focus Group Participants.
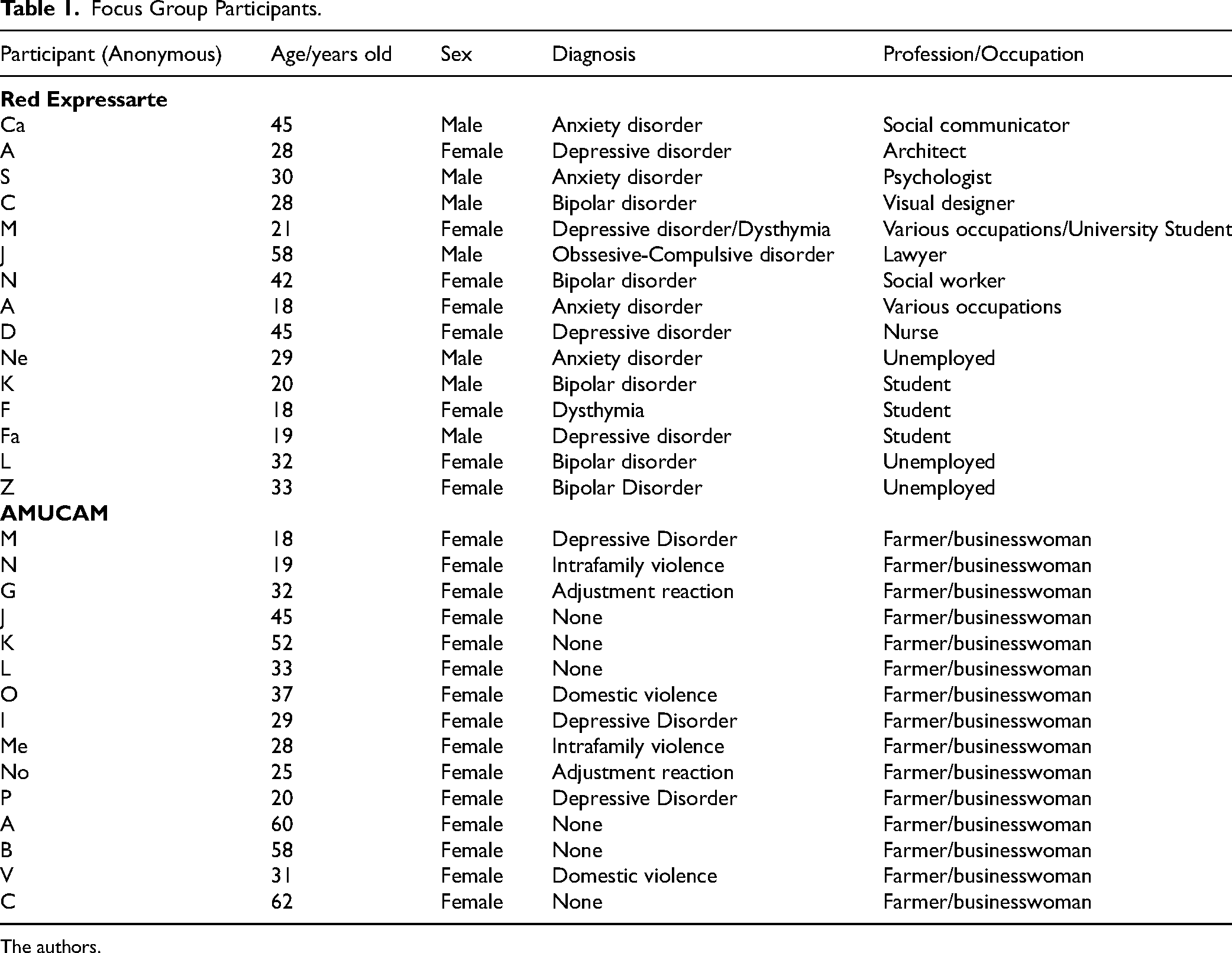
The authors.
Amplifying Actions of the Group for Health
The community mental health strategy groups are initially understood here in a broad sense as collections of individuals who share a common spirit. This includes objectives, beliefs, standards, norms, practices, limitations, history, and so forth, as long as the members are willing to function as a group. This implies, at a minimum, a shared goal or belief. Among what is shared in these actions, “C” acknowledges: “In the group, we always provide feedback on each other's cases, whether they are successful or not. We encourage each other, rejoice when someone is doing well or had a positive outcome, and feel sad together. Additionally, we support each other in moving forward”. Adding “E” about the importance of the group in recovery: I have been through all kinds of medications. I'm an agronomist, working in agriculture, but I can tell you about the side effects and how these medications work. I can also say that only a few of them worked for me when I first joined the group. That's why I tried to stop taking them, but I started again because they caused insomnia, which is a symptom of bipolar disorder. However, the effect I was hoping for on my mood, tranquility, joy, motivation, and irritability emerged with the group, with the activities, with being part of something… The group did what neither my family nor the healthcare system has done. It made me feel like I am not alone. Knowing that if I speak, I will be heard and responded to. It greatly helps alleviate the discomfort caused by loneliness, which I had always believed was impossible to overcome. The group is where we, tired individuals, come without fear, to be ourselves and more than just ourselves. They care about our existence beyond the symptoms and the infamous diagnostic criteria. Here, I am more than just a collection of symptoms.
Groups as Complementary to Other Forms of Care
The group emphasizes the difference between community-based and clinical processes, as highlighted in the statement, “Here, I am more than just a collection of symptoms.” This opens up the discussion about the relationship between individuals and the healthcare system. “A” mentions, “The healthcare system may not consider the individual's unique way of solving problems.” However, in community-based mental health actions, “understanding and humanity can confront the difficulty of having psychological problems and being surrounded by people who see you only as just another patient, just a person with one more issue,” as noted by “M.”.
When exploring other aspects of the relationship with the healthcare sector, “F” emphasizes, “I don't take medication, not because it's harmful - I've read that it's safe… It's because of the role that medication plays in the doctor-patient relationship… It's a power dynamic, and that doesn't help.” “J” adds, “Control is achieved not so much through an individual but through respect, unity… respect among equals, not just between doctor and patient”.
Expanding on “D's” perspective, they state, “A psychologist from the healthcare provider is just going to give me advice. I have two options: an argumentative approach and the approach of sharing experiences, but they are not mutually exclusive.” When delving into the relationship that can exist between healthcare personnel and community-based mental health actions, “O” describes: I arrived at the group exhausted from going around in circles with appointments, therapies, and medications. Nothing was working. Until I joined the group, putting my all into it. But there, it worked. Finally, there was someone who showed me like a light, and I thought, “Yes, yes, that could work for me.” They advised me in the group to make an appointment with a psychologist and then with a psychiatrist for medication. They motivated me to schedule an appointment with the healthcare provider. And that's when things started to work… It's a bit of everything… bipolar disorder is too complex to be treated in just one way, but if we need to focus on something, it's on recovering our support networks, even more than relying solely on medications. But it's not entirely their fault either. We need to look at the healthcare system itself. They are exhausted, given only 20 min to address everything. It's logical that they reduce our existence to a prescription when they have just a few minutes to provide a solution to such a complex problem.
One of the final statements in the group, before the closing process, reaffirmed the theory proposed by the thematic analysis. “J” mentioned: I am 59 years old, and I have had depression since I was 15. It has been many years dealing with this. I have learned a lot, both as a patient and even more as an active participant. That's why the healthcare system, with its administrators and scientists, should learn more from support groups or mutual aid groups, like the one with my peers… They should learn about treatment goals, how to cope with pain… Professionals are the ones who read the books, but we live life. We need that knowledge, therapies, medications, whatever it may be… in life, not in sometimes abstract categories. In this, they, us, they who sometimes become us when they become tired and sick, we are part of the same team.
The theme and categories formed by the results are indicated in Figure 1. Additionally, the definitions constructed and agreed upon within each group are provided.
Discussion
Given the increasing prevalence of mental disorders and the psychosocial disability associated with them, complementary and integrative approaches are becoming increasingly necessary for addressing mental disorders. 8 In line with this, the present study has focused on understanding the relationship between community-based strategies, particularly group-based ones, and mental health services from the perspective of individuals who are part of these strategies.

Configuration of community mental health in the healthcare system. Note. Configuration of the Group as a Health Option. The authors.
In the groups of this research, the advantages of such a connection are reaffirmed, where one way to enhance the positive effects of community-based mental health actions could be through the integration with the healthcare system. Other studies have pointed out that while groups offer many potential benefits, their implementation capacity will depend on local realities, including the differential approach mentioned in the results.25,32
In Latin American contexts, other authors have pointed out, referring to community-based initiatives in Peru, that these represent less than one-fifth of what is required in the country, where budgetary constraints remain a common denominator.5,21,22 This is reaffirmed by the participants, who describe ineffective previous treatments, the stigma of mental illness, and the role of groups as complementary to the healthcare system. They also highlight issues such as lack of service continuity, limitations in accessibility to mental health services, deficiencies in timely mental health care, and the fatigue experienced by healthcare personnel.
The manner in which a healthcare professional communicates with and perceives a person with a mental disorder may also be influenced by intrinsic factors related to the professional's repeated experiences with certain types of patients, their care philosophy,33,34 as well as socialization factors linked to gender, culture, and medical training. 35
Regarding this last point, it has been described that exhaustion can manifest as emotional exhaustion, apathy towards work, patients, or colleagues, and feelings of personal inadequacy. 36 These attitudes are not only seen in users but also in health personnel, and this has had an impact on the attitude of seeking help for mental health disorders. 37
As affirmed by the group members, it is found that the perception of control by healthcare professionals can impact agreement with recommendations. This perception can impact their recovery by diminishing the perception of internal locus of control and increasing the perception of stigma.15,38
Similarly, within the support strategies provided by other group members, it was crucial to share guidelines for managing the illness (eg, medication adherence), as also noted in other studies. 39 Supportive interaction, through the communication of feelings and experiential knowledge among group members, tends to have a positive influence on treatment adherence among the members, as it facilitates the acquisition of knowledge and skills that are useful for coping with chronic conditions. 32
Beyond adherence to management, in terms of well-being, Seebohm et al. 19 found that the majority of the groups promoted a healthy lifestyle, exercise, and diet both within and outside their meetings. This included access to complementary therapies, walking groups, and sexual education, creating a perception of the groups as safe spaces where members felt cared for and learned to take care of themselves.
In addition to the significant gaps highlighted in accessing essential clinical care. 10 There are also barriers to accessing psychosocial recovery settings. This could be related to governance difficulties such as limited research resources, functional fragmentation of mental health systems, lack of a national healthcare system, lack of policies directly impacting the organization and provision of services, or misguided policy management. 23
The predominance of the biomedical approach, and the excessive medicalization of mental health contribute to an inequitable assessment of services. 22 It is necessary to redirect state spending towards community services that guarantee citizens’ rights and promote well-being. 40 As the participants point out, the above is directly associated with the creation and sustainability of community mental health strategies, as well as the connection with the healthcare system that validates health rights and respects autonomy. 6
One of the objectives described in CBR is to create bridges in dissent. 41 Therefore, this research proposes, through the voice of the individuals, a dialogue between their own knowledge and the knowledge of healthcare professionals. This approach has significant benefits in improving well-being, including behavioral changes and increased medication adherence, to name just a few aspects.
One limitation of this study is that it did not include the perspective of healthcare professionals. As the participants acknowledge, factors related to work overload and administrative aspects of the healthcare system could play a role in the perceptions of healthcare providers. Future studies could utilize quantitative and longitudinal methods, as well as conduct focus groups involving mental health professionals and individuals with psychiatric diagnoses.
People point out in the present study that partnerships with other sectors from the health sector could provide legitimacy in the broader institutional sphere. This must be reinforced by improved mechanisms for reliable funding and substantial protection against the disruptions often associated with leadership changes in these groups. 31
This association must be carried out without compromising the principles of community action, which means preserving the freedom of decision-making and maintaining horizontal relations between its members.11,41 In the case of Mutual Aid Groups, they determine their own ethos and appoint their own leaders and are generally able to promote the ethos of the group by virtue of their collective nature.
It is concluded in this research that there are important comments from people who attend mental health services about the care process, especially about the attitude of health personnel and about administrative barriers that could hinder the recovery process. It is also proposed that the voice of the people could be taken into account in the design of treatments and health services. The above could contribute to reducing disparities, protecting human rights and shortening the path to recovery.
Footnotes
Acknowledgments
To the masters who make up the mutual aid groups in Colombia and to Gloria Inés Saldarriaga Toro.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.