
Abstract
To prepare healthcare organizations and patients/families to be equally ready to become partners in co-designing healthcare policy, practices, and improvements, there is a need to (1) understand how “co-design ready” organizations and their staff and care providers are to co-design health care policies, practices, and improvements with patients and families; (2) understand how prepared patients and families, as users of the health system, are to step into co-designer roles with confidence so that their voices will be heard as they influence the development or changes to improve healthcare system policies, services, practices, and products; (3) anticipate and/or address challenges with meeting the expectations of what is involved with the co-design approach, including with recruiting, preparing, and training care setting leaders, staff/care providers, and patient/family advisors; (4) ensure care settings provided appropriate tools and resources to support co-design; and (5) guide the shift in culture from engagement to co-design. Recommendations for enabling co-design in care settings include providing an orientation and preparation workshop and guide/workbook. An example of an orientation and preparation workshop is shared.
Keywords
Introduction to the Issue
Over the past decade, healthcare services or organizations have been moving towards becoming “co-design capable” environments, 1 with care providers ready and able to partner with patients and families in different ways to be more than recipients of care and supports. The aim has been to shift the healthcare system culture 1 to accept patients/families as active partners in the actual design, planning, decision making, and improvement of healthcare. In other words, patients/families have become part of the healthcare team. They are moving beyond “involvement and engagement” to “co-design” (also identified as co-develop, co-create, and co-innovate), influencing changes or improving healthcare systems, services, practices, and products with the end-user or care recipient in mind. 2 This type of patient involvement is at the upper end of patient engagement continuums which focus on “empowerment” or “partnership and shared leadership.”3–5 Although co-design is not easily defined, those that apply the principles of co-design in healthcare all mention the need to have the health service users (ie, patients and families with lived experiences) become the designers of their health system and its delivery. The motivation of these service users is driven by their intent on improving care and outcomes, or ensuring the best possible care is delivered in the best possible way to the right patient at the right time. 6
The challenge is finding both healthcare systems and care providers which are co-design ready or capable, as well as patients/families who are ready and able to step into these co-design Advisor or partner roles. Most often these patients/families are volunteers within health systems, contributing their time when available to “make a difference.” In many situations, there are assumptions made about the extent of readiness (ie, knowledge/awareness, attitudes/acceptance, openness, skills, capacity, time, etc) of either or both patient/family advisors (PFAs) and healthcare providers in care settings to be involved in co-design practices. So, what needs to be in place to guide and prepare health care teams of care providers, PFAs and others to be co-design ready to contribute to healthcare improvement?
In this perspective article, we discuss what we have learned over 5 years of working with various care setting teams across Alberta Health Services (AHS) that included PFAs. We share some factors that need to be considered for PFAs and care setting teams to be engagement or co-design ready including challenges that need to be anticipated and addressed. We also provide some recommendations, one of which mentions workshops. We share an example of a “Co-design Orientation 101” approach which we implemented and tested over 5 years with various health care teams/settings within AHS. 7 This orientation provides key aspects of what, why, how, and when of the co-design approach, with the intent of preparing both the care providers and PFAs for a culture shift to become capable at co-designing healthcare quality improvement (QI) initiatives. More details related to the implementation and evaluation of the co-design approach with various examples of healthcare QI initiatives are described in other reports. 7
Key Factors for Consideration
In order to apply or implement co-design, and particularly within health care organizations, a clear understanding of potential barriers and facilitators is needed. 8 The first step, often one of the challenges, is bringing together healthcare teams of care providers and PFAs in different acute and community care settings to begin the conversation of how they will work together and what they will do regarding QI, and why. QI discussions often raise debates about some of the existing and anticipated barriers and facilitators related to care settings and care delivery, and therefore, the importance of properly planning, before executing and evaluating their QI initiatives. This also means talking about the PFAs coming in as volunteers and being part of the care setting team—how they are recruited or accessed through dedicated in-house volunteer services. Some organization policies define volunteer PFAs as being entitled to receive reimbursement for expenses but not time, unless external funding exists to support honoraria. It also means connecting with care settings proactively to have safe conversations with care providers and staff about engaging PFAs in QI. There needs to be buy-in for the co-design process from both groups as they are asked to be respectful partners throughout the process and commit to invest their time and effort to achieve agreed on outcomes for their improvement initiatives. 9 Co-design takes more time, patience and open, direct contribution of all involved. Fortunately, our organization, AHS, supports the implementation of co-design through a Patient First strategic plan and principles of Patient-and-Family-Centred Care (PFCC). Across AHS, over 1200 registered and trained PFAs and many other patient/family volunteers were already embedded within various PFCC initiatives, advisory committees or councils, and decision-making committees, some at the provincial level and some specific to one of over 600 different AHS facilities or sites and multiple service programs. 5
The challenge that follows recruitment of the care teams is how best to inform these teams as to what co-design is; why it is of benefit to apply in the development or improvement of healthcare practices, policies, or other initiatives; how it can be facilitated and applied/implemented in a systematic way for QI initiatives; and when it is good timing to apply co-design principles with the QI initiative. Thus, a co-design orientation or workshop is highly recommended, drawing from existing materials, resources, and approaches.
Other considerations include ensuring care settings have leadership support for the co-design approach and have access to or have the resources to support co-design—that is, being able to involve staff with different expertise (eg, experience measurement, QI) to facilitate or champion the co-design work, ensuring time dedication of staff to the process, having access to or open to having PFAs involved in care setting discussions, having clear organization/setting expectations or aims, and having access to existing data sources indicating what care aspects are working well for patients and which need improving.
Just as significant, PFAs, as volunteer co-designers of their health care and/or its improvement need to address “the imposter syndrome.” PFAs know what they experienced in health care and the resulting outcomes. However, sitting at a table of healthcare professionals can be daunting and/or intimidating thus the PFAs may hesitate to share their “voices.” This hesitation to share and explore ideas must be addressed to achieve a co-design approach. As PFAs become true partners, a culture shift may be experienced by all participants.
Recommendations
Readiness assessments and preparation/planning are essential in order to have the discussions and follow through on implementing co-design approaches with care teams. It is fair to say that some care setting staff/care providers are more co-design ready and willing than others. A simple question about the care setting staff/care providers’ level of engagement with patients/families is a starting point. No or little engagement means more work is needed to prepare the care setting before implementation of a co-design approach.
PFAs, too, will need some screening if possible. Recruitment can involve having “job descriptions for PFAs regarding co-designing healthcare QI initiatives,” including what QI opportunities are about or what they involve, how much time is expected or needed depending on type of QI initiative (anywhere between 3 months to 1 or 2 years), and outcomes anticipated. There are opportunities for PFAs with identified experiences, as well as for those with no previous experiences. Regardless of experiences, all PFAs should be provided with training in co-design as part of their care team preparation. This training must offer time to explore the “imposter syndrome” that some PFAs may be experiencing, as well as enhance their interests and retention as active and respected care setting team members.
Finally, the main preparation task can be a workshop to assist PFAs and care teams with learning new co-design knowledge, skills, and dispositions for successful QI work. 10 In our case, we co-developed a 3-hour “Co-design Orientation 101” workshop specifically targeting healthcare QI initiatives. We could deliver this in 1 block of time or 2, in-person or virtually. The workshop and preparation of the care setting team is put into practice during the actual step-by-step QI work. We also built in an evaluation process to determine the experiences of both groups of PFAs and staff/care providers and attempted to make improvements on aspects of the approach and work as we proceeded through the steps of our QI initiative.
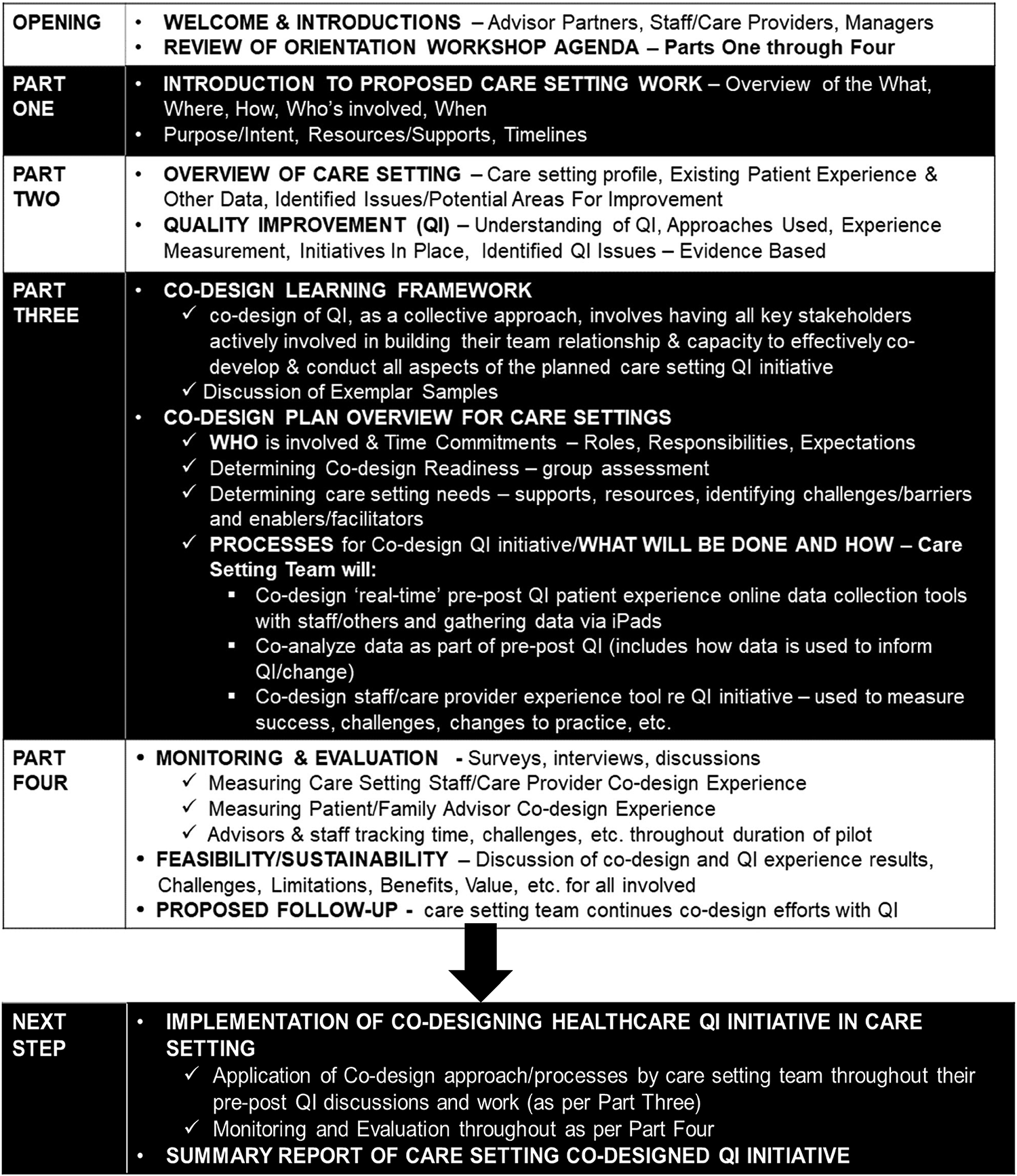
The intent of the workshop was to facilitate relationship building among the participants and help them to understand, implement, and influence the co-design process throughout the QI work. An orientation workbook or guide, agenda, and session power point slides were provided to each participant at the workshop. The agenda and orientation guide followed the same discussion items (shown in Table 1), so participants could take notes, identify questions or issues and use these as part of the follow-up QI work and evaluation of different aspects.
Workshop Co-Design Orientation Agenda and Guide—Preparation of Care Setting Teams to Understand and Implement the Co-Design Approach for Healthcare Quality Improvement (QI) Initiatives.
Conclusion
As healthcare organizations and care teams move into co-designing health care initiatives including QI, it is imperative not to make assumptions that care teams including PFAs know what co-design means, or naturally accept the expectations involved with co-design work and capable of doing such work. It is more appropriate to be proactive and to provide all individuals involved in care setting QI work including PFAs, the appropriate orientation, training, and preparation for co-design work. This ensures success of care setting teams building their capacity to implement co-design in QI and meeting expectations and outcomes. This also enhances the championing, spread, and sustainability of the co-design approach across care settings within healthcare organizations and reinforces the recognition of PFAs not only as “advisors” but more as key partners in making a difference for “what really matters to patients.”
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.