
Abstract
Engaging family advisors in pediatric quality improvement (QI) efforts is well-studied in intensive care but less understood in other settings. The purpose of this study was to assess the perceived impact of including a family advisor as a colead on a QI initiative that successfully improved the family-centered timing of routine morning blood tests performed on pediatric inpatients. Five structured written reflections from core QI team members were analyzed using inductive thematic analysis and 3 major themes were identified. The first found that a family advisor’s presence from the beginning of a QI initiative helps inform project design. The second determined that family partners working with residents fostered a better shared understanding of the role of trainees and caregivers in improving the quality of care. The third found that a family partner is an effective change agent to enact practice improvement, support professional development, and enhance resident education. Our qualitative analysis showed that engaging a family advisor as a colead influenced the design, implementation, and post-intervention impact of the initiative and improved family-centered outcomes.
Keywords
Introduction
The inclusion of patient and family advisors on quality improvement (QI) teams provides a myriad of positive benefits. These include better health care outcomes for patients, reduced medical errors, and perspective into adverse events, as well as increased patient and employee satisfaction (1 –4). Patient advisors are individuals who have previously received health care within an organization, whereas family advisors are caregivers of patients. Both offer unique insights so organizations can better meet the needs of their clients (5).
The use of patient and family advisors in QI work is evolving. In one of the earliest descriptions of this role, Harrison led a group of family advisors in 1993 to author The Principles for Family-Centered Neonatal Care. This defined the need to build partnerships between parents and the health care team, laying the foundation for the role of family advisors in neonatal intensive care unit (NICU) QI work (6). Macdonell et al further described the value of partnering with NICU parents as key stakeholders, encouraging QI efforts to include parents as primary team members at the beginning of a project to apply principles of translational science to put an idea into practice (7). Czulada et al stipulated that including a family advisor as an equal member of the QI team was essential to inform project design and outcomes (8).
Several industry leaders have published guidelines endorsing the use of family advisors in QI work. The Institute for Patient- and Family-Centered Care (IPFCC) proposed 6 key recommendations for creating partnerships within QI organizations, 3 of which focus on the necessary inclusion of patient and family advisors throughout the design, implementation, and evaluation phases of QI projects to optimize outcomes (9). Additionally, the Agency for Healthcare Research and Quality (AHRQ) has published an implementation handbook designed for patients, families, and health care professionals as a guide for incorporating the perspectives that patients and families lend to QI projects (1). Both the IPFCC and the AHRQ recommend inclusion of family advisors on activities such as quality committees, improvement and safety initiatives, and processes for reviewing data related to QI initiatives (1,9).
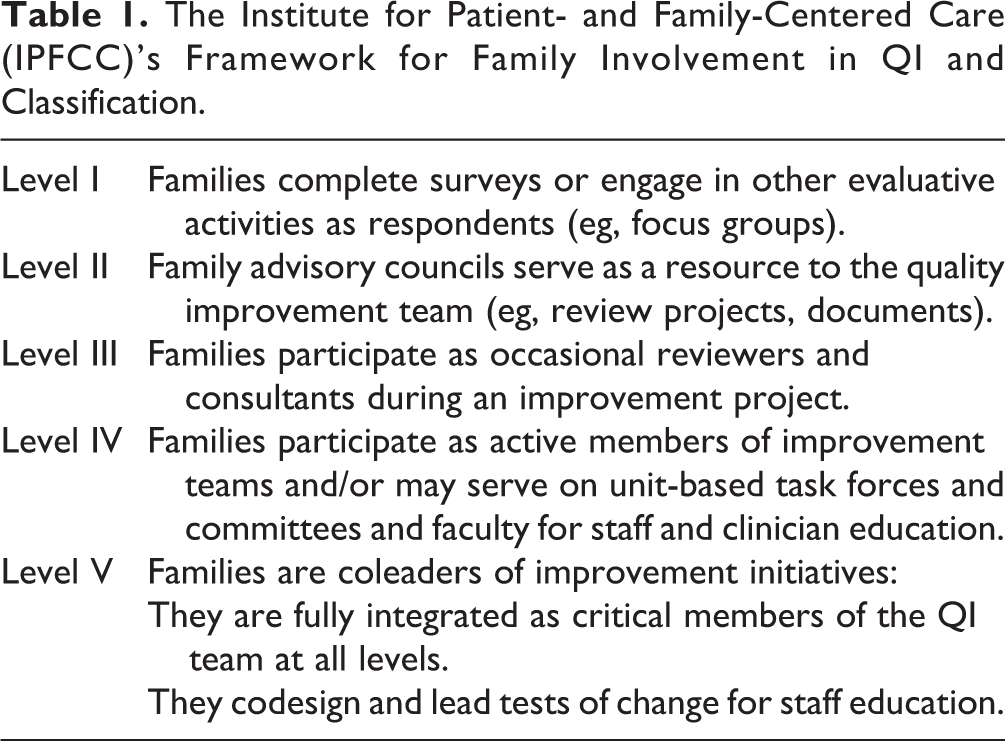
The IPFCC has proposed a framework for classifying the level of family involvement in the QI process, stratifying this into 5 levels: participants (I), advisory board or council members (II), occasional reviewers and consultants (III), ongoing advisors and consultants (IV), and at the highest level (V), coleaders (Table 1) (10). Health care organizations should strive to establish level V family advisor involvement in their QI initiatives (11).
The Institute for Patient- and Family-Centered Care (IPFCC)’s Framework for Family Involvement in QI and Classification.
Role of Family Advisors at Our Institution
Patient- and family-centered care has been a core value at our institution and a larger health care system for over a decade (12). Recent efforts have sought to engage family advisors in QI initiatives to enhance patient- and family-centered care and optimize outcomes (13). Standardized practices and specific mechanisms are not yet in place to support universal inclusion of family partners on improvement efforts. Furthermore, family advisors do not generally operate as coleaders (level V).
Study Aim
The aim of this study was to assess the perceived impact of including a family advisor as a colead on a QI initiative to improve the family-centered timing of routine morning lab work performed on pediatric inpatients through a qualitative theme analysis.
Methods
Background: The QI Effort
The QI effort was conducted on the Pediatric Hospital Medicine service at a single-site urban medium-sized children’s hospital in the Northeastern United States from March 2018 to September 2019. The multidisciplinary QI team included 12 hospitalists, a resident physician, 3 nurse practitioners, 2 nurses, a QI coach, an administrative assistant, and a family advisor who was the mother of a long-term patient cared for at the children’s hospital. The effort aimed to ensure that 4 key aspects of medical care were consistently reviewed daily on rounds: intravenous
With insight and guidance from the family advisor colead, a key intent of the Diagnostic testing domain was to address the psychosocial stress of overnight blood draws to improve the delivery of family-centered care. As a result, the percentage of lab tests ordered to be drawn after 7
The QI effort successfully improved the primary outcome: the frequency of blood work ordered to be drawn after 7
Data Collection
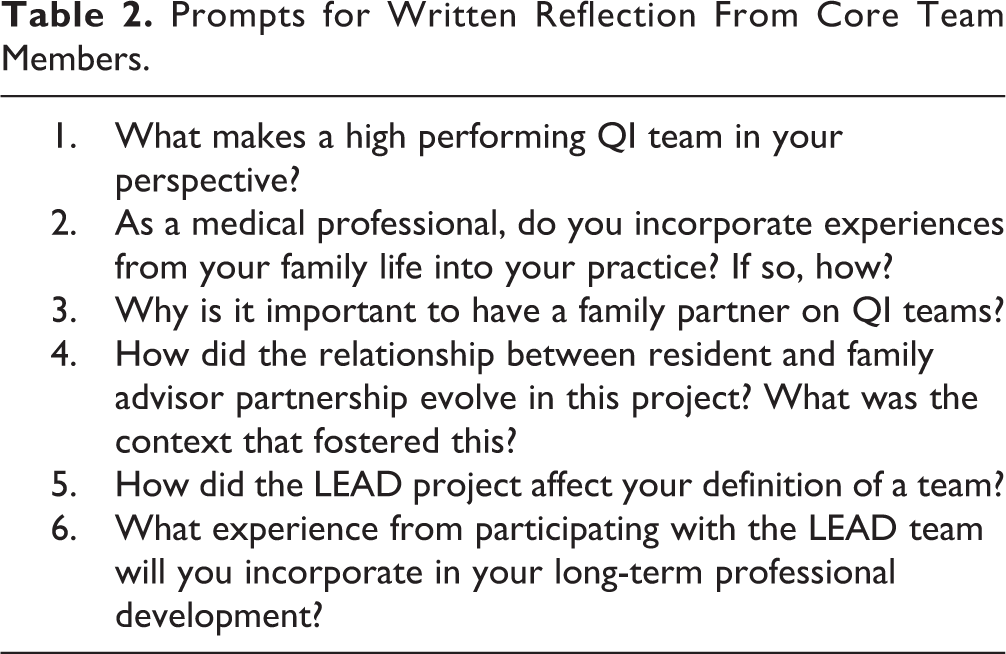
To evaluate the perceived impact of including a family advisor as a colead on a QI initiative, 5 core team members from the larger multidisciplinary group were surveyed and written reflections to structured prompts regarding their experiences were obtained (prompts in Table 2). These included reflections from 2 hospitalist attendings, family advisor, QI coach, and resident physician. Members of the larger multidisciplinary QI team participated at varying levels but did not collaborate with the family advisor as deeply as the 5 core members. The core team consistently attended monthly meetings, codesigned PDSA cycles, educated staff, and were critically involved in the implementation and evaluation of the longitudinal QI effort. The institutional review board of our institution at the University of Rochester deemed the study exempt (STUDY00004219), and a waiver of consent was obtained from participants.
Prompts for Written Reflection From Core Team Members.
Qualitative Data Analysis
Reflections were analyzed for patterns of meaning and areas of interest, representative of each participant’s personal reflection and overall experience. A qualitative theme analysis was conducted using the thematic analysis of Braun and Clarke as a guide (14). Two members of the larger multidisciplinary QI team examined reflections and identified similar responses that were coded as discrete ideas. Inductive coding methods were used to organize codes and quotations from each member’s personal reflections into overarching themes and subthemes representing common perspectives and shared insights; these were collectively analyzed, reviewed, and refined to achieve consensus (15,16).
Results
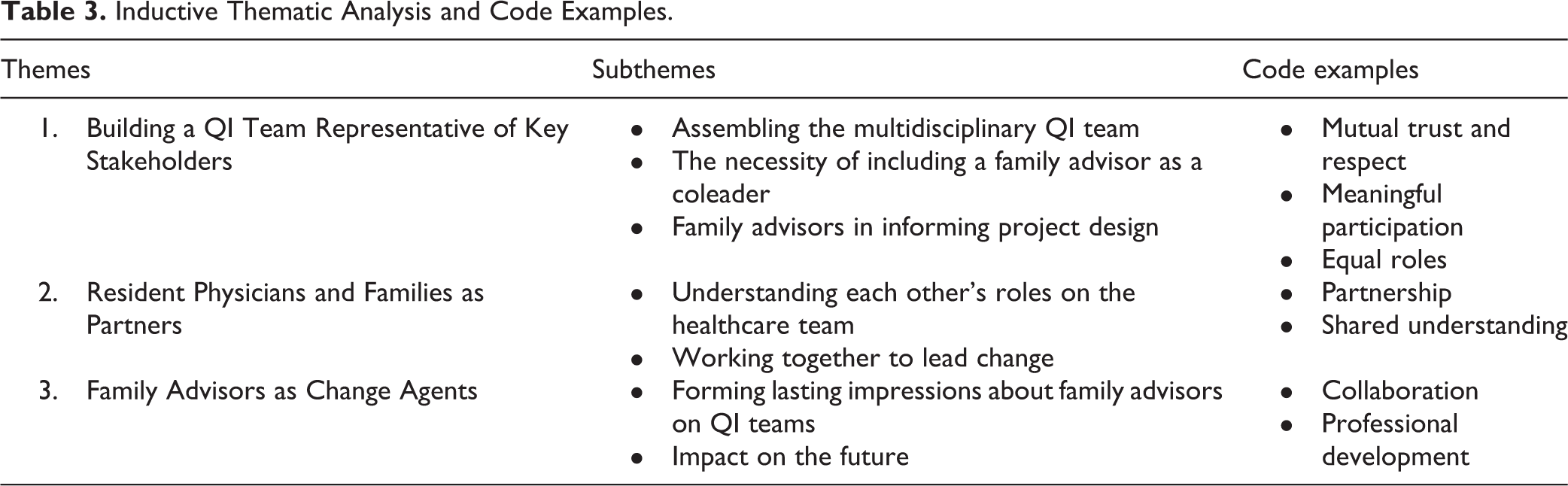
Three major themes were identified, each reflecting the value of including a family advisor on a QI effort and the positive impact study participants expressed (Table 3) (16). Selected quotations from participants relevant to the identified themes are listed below.
Inductive Thematic Analysis and Code Examples.
Theme 1: Building a QI Team Representative of Key Stakeholders
Crucial to the success of the QI initiative—titled “LEAD the Way”—was the focus on a model of improvement that aimed to engage patients and families in hospital-wide QI efforts. To achieve this, the team assembled representatives from various health care professions.
Assembling the multidisciplinary QI team
The team felt strongly that the inclusion of multidisciplinary members was essential to aligning goals and creating a shared agenda dedicated to improving the patient and family experience of care. The attending physician lead explained: Ideally, a team should be multidisciplinary because different perspectives and skillsets allows a team to implement a QI project with success. QI is intended to improve a complicated system with many stakeholders, so the team needs to have representatives from varied levels of the healthcare system to be able to disseminate and conduct PDSA cycles. A high performing QI team has team members that come from different backgrounds. This is important for team members to bring different ideas and perspectives…
The necessity of including a family advisor as a coleader
From the beginning, the team recognized the importance of partnering with patients and families at an individual and institutional level to improve patient and family-centered care. The family advisor’s role was fundamental. The QI coach explained: The presence of patients and families on our QI teams ensures system design and changes are patient and family-friendly. We often talk about patients and families as intangibles; however, by having a family member as a colead on a QI project, they offer their own perspective and experiences to help shape medical care because they are the ultimate recipients. In each QI project, the patient and family are the ultimate key stakeholders. Despite well-intentioned efforts, those in administration, those at the bedside, and those guiding research do not possess the perspective of a patient or family. There needs to be involvement from a family advisor.
Family advisors in informing project design
The family advisor brought a critical and unique perspective to the team by sharing her experiences as a mother of a long-term patient cared for at the children’s hospital. She explained: A family partner has personal experience to bring to the team to help others understand how an idea for improvement may affect future patients and families. They help the team understand exactly what a patient and family may be going through.
Theme 2: Resident Physicians and Families as Partners
Having a family advisor share her personal experience with the QI team and with resident physicians enabled health care personnel to better understand and empathize with the parent perspective.
Understanding each other’s roles in the health care team
Knowledge gaps can exist between resident physicians and families due to confusion about the roles and responsibilities involved in caring for a child in the inpatient setting. By listening to and recognizing family needs, residents and families can work together to improve care. The resident physician stated: “By having a family advisor share their perspective, residents can see how patient-family experiences might be improved in the hospital.” “The resident and family partnership continued to grow as just that, a partnership with each contributing to the project based on their experiences and perspectives. This project can be used to show involvement of residents and to help those in training understand by experiencing different ways of working with families…”
Working together to lead change
To improve outcomes, the QI committee enacted several PDSA cycles, one of which involved the family advisor educating residents at 2 noon conferences about the QI effort and its focus on enhancing the patient and family experience in the hospital. This example demonstrated the importance of resident–family collaboration to improve patient care. The family advisor stated: This speaking opportunity helped residents identify with the family perspective and gave them a better sense of how to approach patient-families in the hospital setting and build the families’ trust. It also helped residents understand what a family may be going through. I think the context that fostered such strong resident and family advisor collaboration in this initiative was the support of team leaders, the open and supportive personality of our resident and family advisor, and the evidence that supports family involvement in QI…
Theme 3: Family Advisors as Change Agents
By partnering with a family advisor as a colead, our QI team better understood the value of incorporating the beliefs and preferences of patients and families into improvement efforts. Our family advisor’s voice helped define the goal and purpose of the initiative. Her role also influenced the professional development of the team both individually and as a whole.
Forming lasting impressions about family advisors on QI teams
The resident physician described her experience as follows: Our family advisor influenced me to listen to the patient-family story and to incorporate the family voice into my own future practice. As a family advisor, I was able to see what goes on “behind the scenes” of a hospital. This solidified my decision to return to school so I can use my experience to help focus on patient safety and improve the patient experience.
Impact on the future
Having a family advisor on the QI initiative inspired members of the team to partner with families for future hospital-wide QI projects and expand their individual career goals. The QI coach stated: The next stage of my professional development is to create programs that support family involvement in QI efforts and on high performing teams. I will continue to advocate for and include family advisors in future QI efforts, recognizing that they bring the same value to other efforts such as research. A next step in my career development may be to have a patient/family mentor to help improve my clinical skills, education, and work within the community. Something I will take with me into my future career from being on the QI team is the understanding that it does not matter where you come from or the title you have. Everyone has an important place in improving the quality of care.
Discussion
There is increasing evidence that involving patients and families in QI is essential to enhancing outcomes and enacting sustainable change (9,17). A growing number of institutions have followed the IPFCC’s recommendations to engage patients and families in the QI process at various levels (10,11).Example initiatives include work by Taff et al utilizing family advisor surveys to elicit feedback and gather perspectives from patients and families primarily in an ambulatory setting to improve health care experiences (18). Members at Stony Brook University Hospital developed a family advisory board to assist in providing more comprehensive patient- and family-centered care in the pediatric intensive care unit (19). Atwood et al described a family advisor’s involvement to improve the family experience during newborn hospitalization for neonatal abstinence syndrome (20). A study by Rosenberg et al incorporated a family advisor to assess the provider–family dynamic as it applies to the safety of pediatric inpatients (21). While these studies highlight the value of family advisors as key stakeholders in QI efforts, none engaged family advisors as level V participants.
Our QI team implemented a novel approach by establishing a family advisor as a level V coleader on an improvement initiative. From the beginning, our family advisor was fully integrated as part of the QI effort, and team members viewed her personal experience and unique perspective as critical to the QI effort’s codesign and patient- and family-centered aim. Across the core team, her inclusion was perceived as essential to its success.
Strengths and Limitations
As a colead, our family advisor contributed to the design, development, and evaluation of our initiative and contributed to a cultural shift within the residency program and hospital system that improved patient- and family-centered care. Our team identified opportunities for improvement in hospital practice from a parent perspective and enacted change because of this insight (22).
This analysis revealed that the relationship that developed between family advisor and residents seemed to impact both parties positively. The team structure of engaging family partners on a QI initiative demonstrated the value of families and residents as partners to initiate change within the health care system. The model of coleadership for a quality and safety effort with family advisors and resident physicians showed promise for advancing improvement science and project management.
This study has several limitations. First, the small sample size of 5 study participants may have resulted in minimal variation and may not have allowed for saturation. However, these team individuals had the most experience as core members of the QI effort and were from multiple disciplines, providing the most detailed accounts. Future studies should consider increasing the sample size and surveying individuals in the QI effort with varying level of involvement to evaluate whether findings remain consistent. Second, the intervention was conducted at a single-site medium-sized university hospital in an urban setting within 1 QI team. The transferability of these data to other institutions in different settings is uncertain. Lastly, researcher bias may have influenced the results, as themes were chosen subjectively based on common ideas and overarching themes, though attempts were made to mitigate this with group review and independent analysis. For future studies, computer-aided qualitative data analysis software should be considered, as well as theme identification by noncore team members and open reflection as opposed to structured questions.
Conclusions and Recommendations
Our qualitative theme analysis suggests that the inclusion of a family advisor as a coleader on an improvement effort is critical to ensuring efforts are patient- and family-centered and optimizing outcomes. We urge improvement teams to fully embrace family advisors as level V coleaders to transform health care delivery.
Footnotes
Acknowledgments
The Division of Pediatric Hospital Medicine, Department of Pediatrics, University of Rochester, Rochester, NY, for collaborating on this initiative. Frances Cartella, study team member, for data collection, analysis, and innovative contributions crucial to this effort’s success.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.