
Abstract
Women with perinatal depression are at a high risk for unhealthy dietary behaviors but whether the coronavirus disease 2019 (COVID-19) pandemic has exacerbated this risk is unknown. Here we report the findings of a qualitative study exploring the impact of the COVID-19 pandemic on nutrition-related experiences of women with perinatal depression. Using a qualitative descriptive approach, in-depth interviews were conducted with 18 women with a history of perinatal depression and 10 healthcare providers. A semistructured format elicited how food and nutrition-related behaviors of women with perinatal depression were affected by the COVID-19 pandemic. Thematic analysis identified 4 themes related to the COVID-19 pandemic: (1) Adaptations in shopping and cooking behaviors; (2) increases in stress and declines in respite; (3) declines in support and increases in isolation; and (4) low levels of breastfeeding guidance. Our findings confirm the importance of resilience among women with perinatal depression and future research is needed to elucidate the mechanisms connecting resilience and dietary behaviors.
Keywords
Introduction
Perinatal depression (PD), the experience of depression during the prenatal and/or postpartum period, 1 affects between 12% and 30% of women worldwide and is associated with a higher risk for poor dietary behaviors.2,3 These dietary behaviors can lead to obesity, which also increases the risk of depression, 4 highlighting the cyclical nature of depression and poor nutrition. Following a healthy dietary pattern, consisting of fruits, vegetables, whole grains, and fish, is associated with a lower risk of depression and a reduction in depressive symptoms. 5 Mothers with PD may also exhibit negative child-feeding practices such as forceful or restrictive feeding.6–8 Hence, the development of behavioral dietary interventions for women with PD is a public health priority.
The COVID-19 pandemic became a worldwide public health concern at the beginning of 2020, prompting social distancing and stay-at-home measures to limit the spread of the virus. As a result, the prevalence of stress, anxiety, and depression increased in the general population and among perinatal women.9–11 In the general population, increases in COVID-19-related depression and anxiety have been associated with increases in emotional eating, fast food intake, and food insecurity; and decreases in fruit, vegetable, and legume intake.12–14
Several concerns for mothers’ nutrition during the COVID-19 pandemic were voiced including food insecurity, poor-quality diets, and unhealthy household environments. 15 These concerns were warranted as mothers’ nutrition and feeding practices were affected by the pandemic. Mothers did utilize more food assistance programs during the COVID-19 pandemic but also consumed a less diverse diet. 16 Moreover, decreased consumption of vegetables, legumes, fruits, and fish was observed among pregnant women. 17 The COVID-19 pandemic also affected mothers’ experience of feeding their infants, as the initiation of breastfeeding was delayed or never occurred.18,19
To the best of our knowledge, the ways that the pandemic has impacted the dietary behaviors and experiences of women with PD, who are already at greater risk for poor dietary behaviors, have not been explored. Understanding how nutrition-related behaviors may have been affected by the COVID-19 pandemic may help health care providers understand how to support women with PD during future personal or public health crises. Therefore, the purpose of this analysis was to explore the impact of the COVID-19 pandemic on nutrition-related experiences of women with PD, including their experiences regarding infant feeding.
Methods
Study Design
Using a qualitative descriptive approach and a phenomenology orientation, we conducted in-depth interviews with women with a history of PD and healthcare providers who care for women with PD. 20 The investigation is a secondary analysis of a larger, multiple methods study that explored nutrition-related beliefs, practices, and challenges of women with PD as related to the mother's own nutrition; and identified the mother's personal, social, cultural, and environmental factors that influence decisions about feeding her child. 21 We used triangulation to compare and contrast different sources of information (e.g., women with PD and healthcare providers) by examining the evidence from these sources to build a coherent justification for themes. 22 This study was approved by the Institutional Review Board at Drexel University.
Participants
Women with a history of PD (hereafter referred to as “mothers”) and healthcare providers were recruited through Philadelphia-area maternal mental health organizations and ResearchMatch, an online recruitment service (https://www.researchmatch.org/). To maximize participant diversity, participants were purposely sampled (e.g., race/ethnicity, age, parity, history and duration of depression, and specialty of practitioner for healthcare providers). Mothers were eligible if they were 18 years or older, fluent in English, and had been diagnosed with PD in the past 5 years. Healthcare providers were eligible if they were over the age of 18, fluent in English, and work with women with PD.
Data Collection and Analyses
All participants provided informed consent using an online form. Participant descriptive characteristics were collected using a brief structured survey. Descriptive statistics were summarized using means and standard deviations for continuous data and frequencies and percentages for categorical data. All quantitative data were analyzed with IBM SPSS Statistics, Version 28.0 (Armonk, NY: IBM Corp). Data collection occurred between August 2020 and April 2021.
Semistructured interview guides were developed for interviews with both sets of participants (Supplemental material). Interviews were conducted using HIPAA-compliant Zoom, were recorded, and lasted approximately 45 min; participants received a $50 gift card incentivization. Three members of the research team (DS, CK, and BJM), all females with experience in qualitative research, conducted all interviews. Verbatim transcripts were uploaded to NVivo qualitative software (QSR International Pty Ltd. Version 11, 2015) which was used to aid in data management and analysis. During the analysis of the last interview, no new codes were identified, ensuring that data saturation was reached. Initial analyses revealed that although the interview guide did not specifically ask about the pandemic, participants were directly and indirectly sharing their experiences related to the pandemic. Hence, initial coding used a broad general code for the COVID-19 pandemic. For this specific analysis, a second round of coding was used to explore inductively both the impact of the COVID-19 pandemic and responses to the pandemic. Transcripts were analyzed and themes related to the COVID-19 pandemic were identified by 3 researchers and refined by the entire research team.
Confirmability, credibility, dependability, and transferability criteria were used to ensure trustworthiness. 23 Confirmability was established by recording all research-related activities. Credibility was ensured through peer-checking. In peer-checking, the research team assessed the codes and themes and verified the accuracy of data analysis. Dependability was maintained through data analysis by 3 team members. Transferability was supported through the purposive sampling of research participants.
Results
Descriptive Characteristics
Eighteen mothers and 10 healthcare providers completed this study (N = 28; Table 1). The mean age of mothers was 31 ± 6.4 years; 56% identified as Non-Hispanic White; 33% identified as Black or African American; 50% had 2 or more children, 56% were college educated, and 44% were married. All mothers self-reported experiencing PD within the past 5 years; 56% were experiencing current depressive symptoms and undergoing treatment. For healthcare providers, the mean age was 38.7 ± 8.2 years and 80% were Non-Hispanic White. Most of the healthcare professionals were therapists, with 80% who had spent at least 5 years in their profession. See Supplemental Table 1 for individual participant characteristics.
Participant Characteristics.
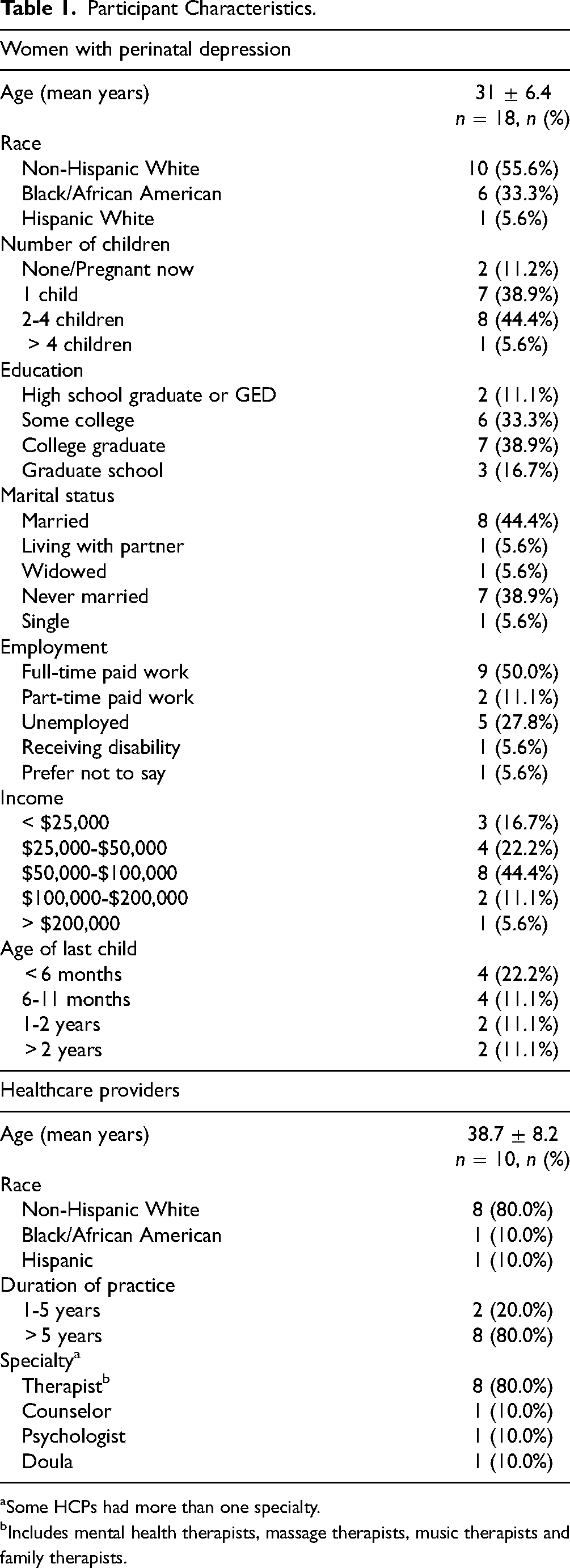
Some HCPs had more than one specialty.
Includes mental health therapists, massage therapists, music therapists and family therapists.
Qualitative Findings
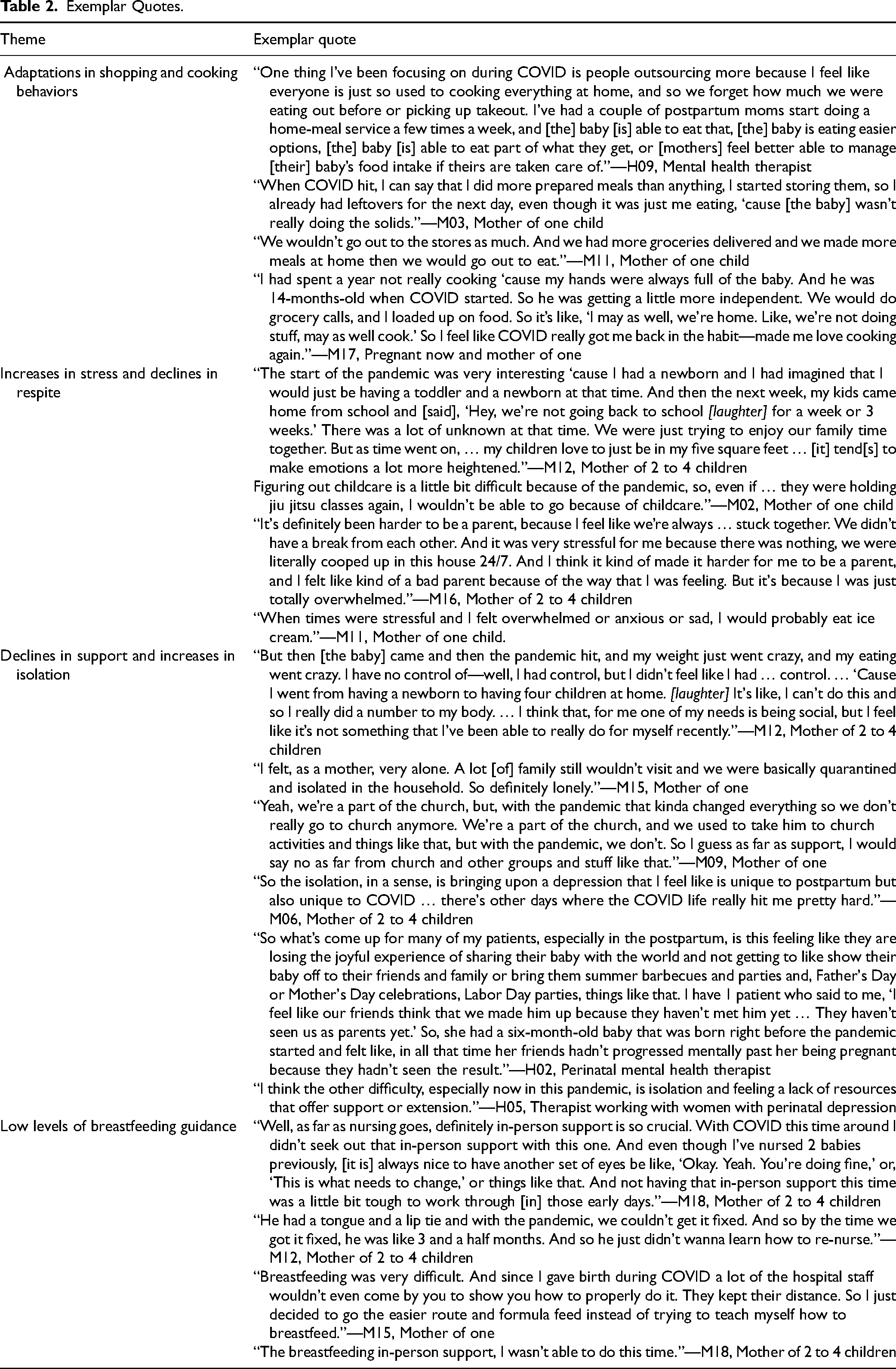
Our study identified 4 themes from the interviews with mothers and healthcare providers: (1) Adaptations in shopping and cooking behaviors; (2) Increases in stress and declines in respite; (3) Declines in social support and increases in isolation; and (4) Low levels of breastfeeding guidance (Table 2).
Exemplar Quotes.
Theme 1: Adaptations in shopping and cooking behaviors
Despite being faced with the pandemic, where stay-at-home measures, low food availability at grocery stores, and other disruptions in the food system created unforeseen changes in the food environment, mothers quickly adjusted their food purchasing and preparation behaviors. For example, M08's husband now assumed the task of food shopping, helping reduce her risk of contracting COVID-19 while she was pregnant. Although time-consuming, mothers also reported visiting multiple stores to ensure adequate food for the household. Many began utilizing grocery delivery services as well. In fact, H09, a mental health therapist, knew of 2 postpostpartum mothers who started a home meal delivery service to help families confined to their homes or those experiencing poor food access. Connecting mothers to food-related resources was a priority for all of the healthcare providers we interviewed. For example, H01, a family therapist, created food resource packets for her clients because she “knew that a lot of kids were now going to lose access to food.”
In many cases, an unexpected benefit of the stay-at-home measures was togetherness in the kitchen and around the dinner table. Mothers began cooking at home more and included their children in the process. For M17, these experiences led her to “love cooking again” and enjoy baking more than before. M12 found herself “constantly in the kitchen” with her children, who in turn, were more “open to trying new things because they were constantly around food.”:
“[We] did a lot more cooking in the beginning [of the pandemic] and we started teaching them how to bake. We went through this whole sweet craze in our house, taught them how to make all different types of cookies, taught them how to make cakes—which was good and bad. [Laughter] Bad for the waistline but good to know.”
Theme 2: Increases in stress and declines in respite
Despite new-found joy in the kitchen experienced by many, mothers in our study still reported increases in anxiety and stress they attributed to the pandemic, which have been associated with poor quality and unhealthy diets.24,25 M17's “overall concern” for protecting her child's life was her primary stressor and one that was “uncontrollable” and resulted in “overwhelming fear.” For M16, her heightened stress stemmed from how she and her children “didn’t have a break from each other. It was very stressful for me because there was nothing, we were literally cooped up in this house 24/7..” For M01, her stress affected her health: “I know I’m not eating right … and with being a new mom but then especially with quarantine, we were just all stressed … I have irritable bowel syndrome (IBS) which when I get super stressed it rears its ugly head.” M11 described that when she was stressed, she “would probably eat ice cream.” M11 and mothers like her may have felt guilty after they gave into their stress cravings. H03 detailed that when mothers weren’t being thoughtful of what they ate, they later felt “guilty about it.”
Under prepandemic circumstances, mothers in our study managed their stress through physical activity and connecting with others, activities they no longer felt were safe or possible. For M02, that meant she was no longer able to attend Brazilian jiu-jitsu classes or walk to work, both of which provided her with a needed “energy boost.” Other missed activities mothers in our study discussed were visiting the nail salon and going out to eat with friends and family. According to H02, connecting with others is an important form of self-care. .She added: “Going to mom groups when they're on maternity leave or baby playdates or seeing their family members” are critical self-care activities for mothers with PD, the absence of which perpetuates feelings of isolation.
Theme 3: Declines in social support and increases in isolation
Nearly all of the mothers in our study felt a lack of support during the pandemic, using words and phrases such as “very alone,” “isolated,” and “lonely.” This isolation affected their food intake and their depression. For M07, having support from her husband and family would have been immensely helpful to her being able to have a healthy diet. During the COVID-19 pandemic, they were working a lot, so M07 was “not able to get that much healthy food … then I have to buy junk food.” H01 recognized that asking for support during the COVID-19 pandemic was difficult for mothers: “I think there’s a stigma, especially with social workers, ‘If I ask for food, you're gonna think that I can’t provide it, and you’re gonna report me to [the] Department of Health Services (DHS).’” H01 continued to describe that mothers who did ask her for support were those she had “been working with for a long time.” M06 reflected that “with COVID[-19], I’m not out in the world having lunches at places with people,” further describing that not being able to socialize with friends was a catalyst for her relapse in depression.
For healthcare providers, mothers’ isolation was particularly concerning because research shows that a lack of social support predicts PD,
26
explaining that the lack of support was particularly detrimental to the experience of motherhood for women with PD. For H02's clients, “especially in the postpartum [period], [they have] this feeling like they are losing the joyful experience of sharing their baby with the world and not getting to show their baby off to their friends and family.” Similarly, H04 noted that her patients found that:
“It's a big deal just even to say- negotiate which family members are allowed to [visit] because a lot of the family members, if they’re working, they’re out and then they can’t quarantine to even see them—it's just, it's horrible.”
Theme 4: Low levels of breastfeeding guidance
While mothers are encouraged to breastfeed their child until at least 6 months of age, some women with PD stop breastfeeding before 6 months for a multitude of reasons including experiencing breastfeeding difficulties.
27
From the perspectives of mothers who gave birth during the COVID-19 pandemic, breastfeeding challenges were not adequately addressed because of circumstances caused by the pandemic. Multiple mothers discussed the importance of in-person support, describing it as “crucial.” This lack of breastfeeding support occurred in and outside of the clinical setting. For first-time mother M15,
“Breastfeeding was very difficult. And since I gave birth during COVID[-19], a lot of the hospital staff, you know, wouldn’t even come by you to show you how to properly do it. They kept their distance. So, I just decided to go the easier route and formula feed instead of trying to teach myself how to breastfeed.”
M12 detailed that her son, “had a tongue and a lip tie and with the pandemic, we couldn’t get it fixed,” and while the issue eventually was “fixed,” “he just didn’t wanna learn how to re-nurse.” Not having in-person support also affected M18. Although she breastfed her previous children, not having “another set of eyes” and guidance from a healthcare provider led her to describe “those early days” of breastfeeding as “tough to work through.”
Discussion
This analysis explored the impact of the COVID-19 pandemic on nutrition-related experiences of women with PD from the perspectives of women with PD and healthcare providers who provide care for them. The following discussion will compare study findings to previous research and synthesize the main themes into key considerations.
Our qualitative data illustrate resiliency in food acquisition and preparation among mothers with PD, particularly when faced with the food- and diet-related challenges presented by the COVID-19 pandemic. Resiliency can be conceptualized as a dynamic process that promotes adaptation to aversive situations, 28 and can be protective against depression in women during the perinatal period. 29 We are not the first to report resiliency among mothers during the COVID-19 pandemic. Kornfield et al. 30 identified factors that affect health among postpartum mothers and found that self-reliance, emotional regulation, nonhostile close relationships, and perceived neighborhood safety were protective against postpartum depression during the COVID-19 pandemic. Werchan et al. 31 also reported resiliency among pregnant and postpartum mothers during the COVID-19 pandemic. In their study, resilient coping behaviors included social support and self-care. Social support encompassed talking with friends, family and other pregnant women, helping others, and engaging with family. 31 Self-care consisted of exercising, sleeping, meditation, and eating healthy, among other self-care activities. 31 In our study, mothers exhibited self-reliance, a resilience factor, by adapting their food shopping and food preparation practices.
Our qualitative data also illustrate an unexpected positive effect of the pandemic—increases in home cooking and engaging in culinary activities as a family. Similar patterns have been reported by others. In a number of recent studies investigating the ways that food-related behaviors have changed as a result of the pandemic, findings suggest increases in households’ cooking together.32,33 In addition to increases in home cooking, mothers in our study also described more frequently involving their children in cooking and baking activities, and this too has been reported by others investigating the effects of the pandemic. 33 Parent-child cooking interventions have been successful in promoting healthy dietary patterns within families, such as decreasing the amount of food consumed outside of the home and greater consumption of fruits and vegetables.34,35 If tailored to address the needs of mothers with PD, these findings illustrate the potential acceptability of mother-child culinary nutrition interventions that promote healthy household dietary behaviors and optimal mother-child interaction. 36 This type of intervention may be particularly instrumental in protecting mother-child interactions, which can be negatively impacted by PD. 37
Mothers in this study described how the stress of the pandemic affected their depression and dietary habits. Experiencing stress in the perinatal period has consistently been associated with unhealthy eating behaviors. One study reported that experiencing greater stress was associated with a greater intake of dairy, refined grains, and added sugars. 38 Likewise, during the COVID-19 pandemic, stress and depression were associated with eating fast food and less healthy foods. 39 A qualitative study reported that perinatal women described giving into their cravings when stressed, then feeling guilt or shame over the foods that they ate, 40 which was also described by healthcare providers in our study.
Not being able to participate in respite activities during the pandemic, such as physical activity and social activities, exacerbated the already high levels of stress experienced by the mothers in our study. Across the general population, people who were previously physically active reported significant reductions in their engagement in physical activity during the pandemic.41,42 As well, engagement in physical activity was inversely associated with the perceived amount of stress experienced. 43 For women in the perinatal period, reductions in physical activity have been associated with increases in depressive symptoms and decreases in quality of life.44,45
The lack of social support impacted mothers’ ability to obtain healthy food. Other studies have also described how instrumental spouses are to accessing healthy foods for perinatal women. 46 In addition, having support has been associated with consuming a healthy diet. 47 Social programs such as Supplemental Nutrition Assistance Program have been implemented to aid accessing food. Yet during the COVID-19 pandemic, many food insecure individuals did not know what help they could get for finding food or had difficulty getting food from schools and pantries. 48 Moreover, mothers in the perinatal period have reported multiple barriers to accessing social support programs including lack of awareness and stigma. 49 Our findings indicate that support from social networks and programs are important for accessing food and dietary quality for mothers, which should be explored further.
Mothers in our study reported elevated isolation and both mothers and healthcare providers described how the inability to interact with friends and family contributed to worsening depression in the perinatal period. These findings are similar to previous research evidence that has shown that social support for mothers during the pandemic is critically important. Terada et al. 26 reported that among Japanese women, those who had less support during the pandemic were at greater risk for developing PD; and conversely, Lebel et al. 50 found that having more social support during the pandemic decreased the odds of experiencing depression, anxiety and stress for pregnant women. As in earlier studies, mothers in our study who had children before the pandemic felt they had less support during the pandemic than before; 51 and for many, being separated from family as a result of the pandemic left them with no one to connect with or rely on. In other studies, mothers were not able to rely on family because of distance, 52 and this separation caused distress. 53
Mothers identified that breastfeeding support was lacking from healthcare providers during the pandemic. They illustrated that the lack of support was specifically due to social distancing measures. These experiences align with other research outcomes that have identified a lack of breastfeeding support during the pandemic.54–56 Taken together, these findings are particularly alarming because poor communication with lactation specialists is associated with early breastfeeding cessation. 55
Limitations
This study offers key insights into the challenges women with PD faced in their attempts to consume a healthy diet during the COVID-19 pandemic. Additional strengths were the inclusion of both mother and healthcare provider perspectives and the use of triangulation. While qualitative studies provide rich detail into patient experiences, these findings are not generalizable to all mothers with PD. Our findings are limited by the sociodemographic characteristics of the group, which included well-educated, English-speaking women, and healthcare providers who were primarily therapists. Despite these limitations, this research was undertaken during the COVID-19 pandemic, limiting recall bias of experiences. Nonetheless, we note that some mothers did not experience PD during the pandemic but did so previously. Therefore, their recollections of the pandemic may not align with their PD timing.
Conclusion
Understanding the lived experiences of mothers with PD and how the COVID-19 pandemic has impacted their nutrition-related practices can yield multiple benefits. First, researchers and educators can continue to prepare healthcare professionals to adapt and support mothers with PD during a crisis by identifying innovative ways to source healthy food, developing and promoting coping skills to manage stressors, and establishing ways to receive appropriate social and breastfeeding support. Second, this study confirms the importance of resilience among women with PD. Despite being faced with unique challenges and stressors, mothers were able to create positive moments and move forward, exhibiting resiliency. Moreover, future research is needed to elucidate the mechanisms connecting resilience and dietary behaviors. While engaging mothers with PD and their children together during culinary interventions is a promising avenue for future research, strategies for maximizing the quality of mother-child interactions should be addressed and integrated.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231199818 - Supplemental material for Nutrition-Related Experiences of Women With Perinatal Depression During the COVID-19 Pandemic: A Qualitative Study
Supplemental material, sj-docx-1-jpx-10.1177_23743735231199818 for Nutrition-Related Experiences of Women With Perinatal Depression During the COVID-19 Pandemic: A Qualitative Study by Dahlia Stott, Cynthia Klobodu, Lisa A Chiarello, Bobbie Posmontier, Mona Egohail, Pamela A Geller, June Andrews Horowitz and Brandy-Joe Milliron in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735231199818 - Supplemental material for Nutrition-Related Experiences of Women With Perinatal Depression During the COVID-19 Pandemic: A Qualitative Study
Supplemental material, sj-docx-2-jpx-10.1177_23743735231199818 for Nutrition-Related Experiences of Women With Perinatal Depression During the COVID-19 Pandemic: A Qualitative Study by Dahlia Stott, Cynthia Klobodu, Lisa A Chiarello, Bobbie Posmontier, Mona Egohail, Pamela A Geller, June Andrews Horowitz and Brandy-Joe Milliron in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Drexel University College of Nursing and Health Professions.
Ethical Approval
Ethical approval to report this case was obtained from Drexel University (Protocol # 2005007825).
Statement of Human and Animal Rights
All of the research activities were conducted in accordance with the Institutional Review Board of Drexel University (Protocol # 2005007825) approved protocols.
Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.