
Abstract
This study explores the experience of the breast cancer journey for younger women receiving patient navigation services in a healthcare delivery system and any remaining challenges that navigation services may leave unaddressed. In this qualitative analysis, we used a purposeful sampling approach to conduct a semistructured in-person interview with 19 younger women (under 50 years at the time of diagnosis) at various stages of breast cancer treatment and receiving care that included some form of patient navigation services/within the Sutter Health system. Thematic analysis was performed using an inductive grounded theory approach. The patient experience revealed that women receiving navigation services throughout their cancer journey had little concern related to clinical decision-making and treatment. Rather, emotional, and logistical challenges dominate their experience and perceptions of the cancer journey. Managing day-to-day life and the emotional aspects of a cancer diagnosis cannot be disentangled from clinical care. Navigating the emotional and logistical aspects of the cancer journey is an ongoing unmet need for women under age 50, and navigation services can potentially be enhanced to help address these specific needs. Women with breast cancer may benefit from navigation programs focused not only on clinically related challenges but also on recognizing the daily needs of younger women and guiding them through family and job-related obstacles encountered while navigating cancer care. Health systems could enhance existing nurse navigation programs and redesign other aspects of care to focus on meeting these needs.
Introduction
While recent years have seen substantial advances in cancer diagnosis and treatment options, the emotional and logistical journey women undergo when diagnosed and treated for breast cancer remains inordinately complex. Breast cancer patients and their families experience a host of emotional and administrative challenges that unfold throughout the cancer journey affecting their quality of life.1‐4 Additionally, it may be the case that the emotional and logistical challenges experienced vary based on the stage of life. Some studies have examined the challenges experienced by younger versus older women, finding that younger women face a higher degree of stress related to body image, family life and relationships, career, and finances.5‐9 Younger women also face unique challenges associated with fertility, sexuality, and early menopause.10‐12
Among the many strategies sought to improve care coordination and reduce the challenges resulting from these complexities, patient navigation is one intervention shown to provide considerable benefits to patient outcomes for breast cancer specifically.13,14 Patient navigation is a barrier-focused intervention model designed primarily to promote access to timely diagnosis and treatment of cancer and other diseases 15 .
Despite its demonstrated efficacy for breast cancer patients generally, questions remain around the appropriate role of patient navigation in addressing needs beyond those that fall within the clinical care pathway, and specifically the needs experienced by the unique subset of women who are diagnosed before the age of 50. While some studies look at reducing the emotional and psychosocial impact of cancer through various approaches such as mindfulness-based stress management 16 and social support 12 little research has focused on how to holistically approach supporting both the emotional and logistical aspects of life with cancer with previously established patient navigation services.
In this study, we sought to understand the patient experience, specifically for younger women (≤50) who did have access to patient navigation services at some point in the breast cancer journey. While examining the patient experience, we found that women in this subset have remaining unmet needs related to reconciling their emotional and day-to-day needs with the clinical cancer pathway.
Methods
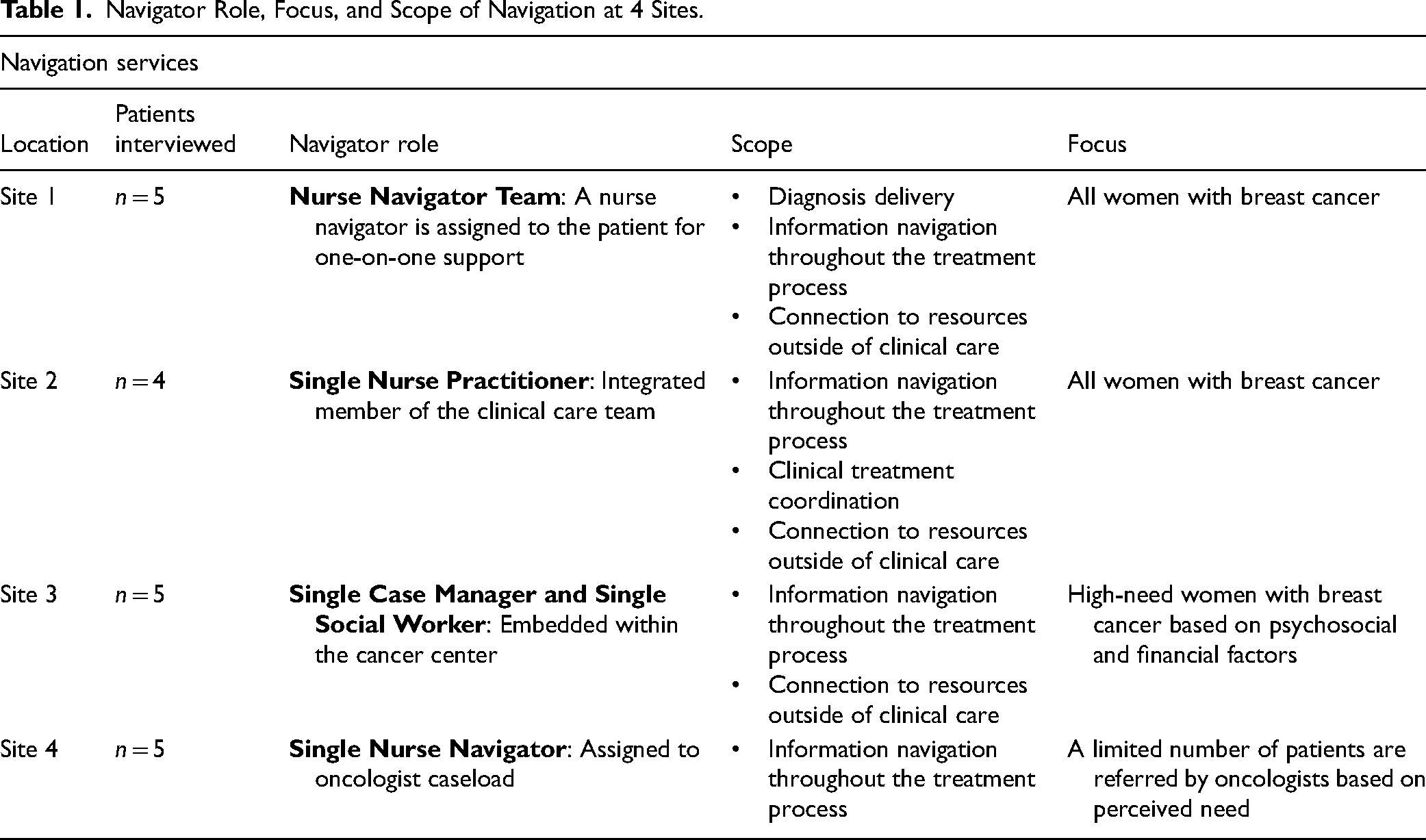
We used a qualitative study design to gain an in-depth understanding of the experience of younger (age < 50) women diagnosed with breast cancer at various phases of treatment, from initial detection and diagnosis through survivorship. Data were collected through in-depth interviews with 19 women diagnosed with breast cancer and currently receiving care within the Sutter Health system, as well as some form of patient navigation service (see Table 1). The study was approved by the Sutter Health Institutional Review Board and informed consent was obtained from each participant.
Navigator Role, Focus, and Scope of Navigation at 4 Sites.
Sampling and Recruitment
Sutter Health is a large not-for-profit health system in northern California that includes 272 outpatient primary care practices and ∼1656 primary care providers serving adult patients. Within the Sutter network, there are ∼15,000 new cancers diagnosed each year. Sites were selected to ensure variation in the availability and/or type of patient navigation services provided and to maximize the variability of patient socioeconomic status and race/ethnicity (see Table 2). We used a purposive sampling approach to identify participants at 4 different sites within the system. Inclusion criteria included: breast cancer diagnosis (any stage), age 50 years or younger at the time of diagnosis, female, and currently receiving cancer treatment at Sutter Health.
Characteristics of 19 Younger Women With Breast Cancer Who Were Interviewed.

1
2. Patient-reported interacting with a nurse navigator at least once while receiving cancer care at Sutter Health.
Recruitment methods were designed to capture the perspective of women with breast cancer at various points in time within the cancer journey and to minimize disruption in the patient care experience. The study team partnered with operational leaders and nurse navigators to invite women with breast cancer to participate. Briefly, eligible patients were identified using Electronic Health Record data; participating clinicians were notified of patients with upcoming visits within a cancer care center. Clinicians and/or staff asked eligible patients if they were interested in participating and provided contact information to the study team, who contacted interested patients, obtained consent, and scheduled and conducted the interview. Participants were given a $50 gift card at the time of the interview.
Interview Process
One-on-one semistructured interviews were conducted between September 2018 and February 2019 at the location where the woman with cancer received care. Questions were designed to elicit women's perspectives on the challenges they faced at various stages of the cancer journey, including how they think of the phases of the journey, the questions, concerns, and challenges faced at various phases, and the sources of support they encountered throughout the journey. Interviews lasted ∼60 min and were recorded and transcribed (see the Online Appendix).
Analysis
We analyzed the data in multiple stages using an inductive grounded theory approach. 18 Credibility was established by reaching an agreement among investigators and interviewers on the interview questions. The team identified emergent themes to develop a codebook by which all data were coded using the qualitative analysis software Dedoose. Two study team members conducted 4 rounds of coding before a final round of coding to reach a consensus on code application and development. Emergent codes were routinely discussed, and once the reviewers agreed upon new codes, they were documented in the codebook and applied to previously coded data. Coded data were summarized and reviewed by all study team members to reach a consensus about the results. Patients were given pseudonyms to protect their identities.
Results
Interviews with 19 women at various stages of the breast cancer treatment journey (see Table 2 or participant information) who received support in the form of patient navigation services revealed a host of remaining challenges related to the emotional experience of breast cancer and balancing the logistics of daily life with cancer treatment.
When asked about challenges in the overall experience, women primarily discussed topics such as dealing with fears and anxiety, organizing childcare and time off from work, and grappling with questions from the existential to the mundane, eg, “am I going to die” and “where do I park my car” at the hospital or clinic? While most women did mention challenging clinical experiences, eg, decisions about mastectomy or hormone therapy, most of their concerns and the biggest challenges they described did not relate to clinical care itself. When discussing challenges in clinical aspects of their care, women with breast cancer described patient navigators as important sources of support that led to the resolution of these challenges.
Navigation services were also described as a source of support for the emotional and logistical challenges; however, descriptions of ongoing struggles with these aspects of the cancer journey indicated that certain challenges outlined below remained significantly unmet. Table 2 includes the key themes and subthemes associated with emotional challenges and is followed by an in-depth description of these unmet needs. Table 3 includes themes and subthemes for the daily life/logistical challenges and is again followed by an illustrative description.
Key Emotional Challenges Faced by Younger Women Diagnosed With Breast Cancer .

*Sixteen out of 19 women with breast cancer interviewed discussed having emotional challenges during interviews.
Emotional Challenges
Some women described feeling separated and disconnected from others (see Table 3), particularly when they first learned of their diagnosis. The notion that the cancer experience is highly individual was often introduced to women by their providers, accentuating feelings of isolation. At the same time, women expressed a parallel belief that there are many common experiences for women with breast cancer and connecting with other younger women made them feel less alone.
Talking about their diagnosis with others also presented an array of emotional challenges. Women struggled with when and how to share their cancer diagnosis with family, friends, and colleagues, and described a feeling of disconnect when dealing with other people's reactions to their illness. Many women shared stories that emphasized the feeling that they were treated differently because of their diagnosis.
Emotional challenge: Loss of identity and normal life
The overall experience of the cancer diagnosis and treatment changed women's bodies as well as their sense of self, distancing them from their familiar precancer life. Several women expressed that not being ready for a new stage of life, menopause, or felt losing their breasts changed an important aspect of themselves.
Breast cancer also impacted women's perception of themselves as mothers. Some expressed feelings of guilt for missing out on pieces of their children's lives. For example, one mother described the emotional challenge of not being able to support her children. Negative self-perceptions of motherhood were also accompanied by concerns about the long-term impact on the mother–child relationship. For example, one mother worried that her newborn was less bonded with her, “I feel like the diagnosis of cancer took away my ability to be the mom that I wanted to be (Dani, age 36).”
Emotional challenge: Fear and future uncertainty
Some women discussed coping with the feeling of a loss of control over their health and fears about the future. One woman stated, for another woman, this loss of security extended to her family as well: “Our solid foundation was taken away. It was an illusion, but in our mind, we felt safe, and this just added a whole other layer of concern (Pricilla, age 48).” Several women undergoing treatment and awaiting scans to assess disease remission or progression described constant anxiety about whether cancer had spread and described imagining worst-case scenarios while waiting for test results. Women in the survivorship phase described facing a lifetime of worry that cancer could come back.
Anxiety and a fear of the unknown manifested in several different ways. Women without children feared that they would no longer be able to have children, or it would prove more difficult. Women with children feared that they may have passed on an increased genetic risk for cancer to their children. They described a chorus of questions in their minds: Did I do the right thing? Did I do enough? Is it gone? Is it spreading? Additionally, the fear of early death consumed some women early in the treatment journey.
Young women's experience of navigation services related to emotional needs
Despite talking extensively about the emotional challenges of the cancer journey, 9 of the 16 young women with breast cancer describing navigating emotional challenges did acknowledge navigators as a source of empathy, noting a warm and friendly nature that seemed more in touch with the emotional aspects of the journey than other care providers. Navigators helped connect some women to resources for emotional support, including peer support groups and therapists. In some cases, the navigator was described as the primary source of encouragement and companionship during the journey, indicating that navigators are well-positioned to provide additional support to target the unmet needs detailed above.
Daily Life/Logistical Challenges
Daily Life Challenge: Balancing parenting and cancer care
Women juggling motherhood and cancer treatment reported difficulty finding childcare during clinic appointments (see Table 4). One mother noted the underlying assumption by providers that women could pass off parenting responsibilities to receive cancer care: “[Clinical staff] just assume that people have family or a support network.—Ellie” Women also described needing more information about when they would be likely able to resume their responsibilities: “I have kids and I’m running a business and I kind of needed to know how long I am going to be down and out (Kendra, age 44)?”
Key Daily Life Challenges Faced by Women Diagnosed With Breast Cancer Under Age 50.

*Fourteen out of 19 women with breast cancer interviewed discussed having daily life challenges.
In addition to juggling cancer care and family responsibilities, mothers faced the emotional work of helping children handle fears about cancer, and cope with the physical changes and pain they saw their mothers experience. One woman described how hair loss affected her young daughter: “It was horrible for [my daughter] and she doesn’t want me to look like a boy. I’m not sure how the oral chemo is going to affect it, so I don’t want to start growing my hair back, having her get used to me having hair, and then start losing it again (Luisa, age 49).”
Daily life challenge: Balancing work–life, finances, and cancer care
Many concerns revolved around the desire or need to continue working. Two women described delaying school or joining the workforce while going through treatment. Women who worked during their treatment described challenges fitting appointments into their schedule, knowing when and how much time to take off from work, and knowing when symptoms were likely to be the worst to plan around them. Others returned to work before they were ready to pay bills. Some women struggled to manage exhaustion and other symptoms while working.
Young women's experience of navigation services related to daily life needs
Fewer women (4 of the 14 women who mentioned daily life challenges) reflected directly on how navigation services supported them with daily life challenges. In the few mentions of this form of support, women with breast cancer were grateful for nurse navigators who helped schedule appointments or resolve scheduling conflicts. One woman did acknowledge the relief felt when a nurse navigator called to walk her through how to handle parking at the surgery center before her surgery.
Discussion
In this study, we sought to understand the experience of navigating cancer care by younger women who have access to navigation services in a large healthcare delivery system. While some women mentioned challenges to receiving clinical care, little discussion focused on clinical care itself, perhaps because navigation services helped address many clinical care issues. Most women described trusting their doctors and going along with recommended treatments after receiving basic information and discussing care with navigators. These interviews revealed that women's biggest challenges related to reconciling cancer care with their identities as mothers and professionals. While women are sitting in infusion centers and waiting rooms, they are worried about how to schedule cancer care around work deadlines, how to find childcare during appointments, and how to work and parent while sick and exhausted. Outside of the clinical environment, they face emotional challenges related to connection with their friends and loved ones, loss of identity, and fears related to future uncertainties. The cancer care they described receiving prioritized and magnified cancer while diminishing or ignoring motherhood and professional life.
Our findings add to the growing evidence that suggests that younger women and their families need enhanced support during the breast cancer experience,2,5,7,8,12,19,20 and most efforts to improve care have fallen under the umbrella of navigation and survivorship care.14,21,22 Additionally, there are significant variations in the navigator's role and responsibilities. 23 An area of opportunity for health systems is to improve patient navigation support by explicitly tackling the emotional and daily life challenges by addressing the emotional and logistical needs in 1 overall journey. Future research may explore how these challenges vary by socioeconomic status, race/ethnicity, and social support.
Enhancing existing navigation programs could include incorporating women's professional and parental responsibilities into initial navigation encounters. A more radical approach to supporting emotional and daily life challenges would involve changing the structure of how health systems provide cancer care, for example, by having more flexible scheduling and weekend/evening hours for appointments, childcare on-site during visits, and preemptively recognizing that younger women (not on Medicare) will have specific insurance and financial questions and initiating education and counseling to address these concerns. Peer support groups, classes, and shared medical appointments may be appropriate venues for addressing concerns common to young women with cancer, including the nuance of finding wholeness within the seemingly split nature of clinical treatment and the day-to-day life of the cancer journey. Other concerns expressed by women we interviewed revealed complex emotional needs that suggest that proactively screening women for emotional health needs and distress is critical. Given the challenges of accessing specialty behavioral health clinicians, 24 integrating behavioral healthcare into cancer centers is a patient-friendly way to ensure women's emotional needs are addressed.
Many of the issues these women faced are likely faced by women of all ages, some are dependent on age and stage in life and represent an additional burden younger women face when dealing with breast cancer. However, much of what these women shared is likely neither exclusive to breast cancer nor women, eg, a 40-year-old father with lung cancer will face many of the same issues as these women. We explored challenges faced by younger women with breast cancer but continuing to understand the patient experience is crucial to improving care across all different cancer types and the continuum from detection to survivorship.
This research was limited to 19 women in a single health system in Northern California. The sample is skewed toward individuals with higher household income, and higher education and is too small to draw reliable conclusions. Only 8 women were in the survivorship phase of their journey. Most of these women had health insurance and access to the care they needed. It is possible that women without satisfactory access to cancer care would be less concerned with the emotional and logistical challenges, however, it is also possible that these challenges would be compounded for them. Although each recruitment site had navigators, we did not ask participants detailed questions about the frequency, nature, or duration of navigation services they received. We used a purposive sampling approach that does not allow us to account for differences across sites or between specific subgroups of women. The themes we identified in our interviews may be sensitive to the nature of these navigation services, as well as the setting and sample.
The major takeaway from our findings is that life cannot be disentangled from clinical care. Patient navigators may be the key people women with cancer interact with along the journey that can offer the time and level of empathy needed to support and advocate for younger women with cancer who experience these nuanced challenges. Evolving and expanding the role of navigators to explicitly address these challenges can help women more effectively overcome these emotional and logistical challenges.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231171126 - Supplemental material for The Unmet Needs of Breast Cancer Navigation Services: Reconciling Clinical Care With the Emotional and Logistical Challenges Experienced by Younger Women with Breast Cancer in a Healthcare Delivery System
Supplemental material, sj-docx-1-jpx-10.1177_23743735231171126 for The Unmet Needs of Breast Cancer Navigation Services: Reconciling Clinical Care With the Emotional and Logistical Challenges Experienced by Younger Women with Breast Cancer in a Healthcare Delivery System by Chelsea Lunders, Ellis C Dillon, Diamonne Mitchell, Cynthia Cantril and JB Jones in Journal of Patient Experience
Footnotes
Acknowledgements
CL oversaw study design, ensured that the study passed the Institute Review Board review and adhered to ethical standards, led efforts to recruit participants, conducted data collection and analysis, and lead the writing of this manuscript. ED participated in research design, data collection and analysis, and drafting and editing of the manuscript. DM participated in the design and coordination of this research, carried out data analysis, and drafted the manuscript. CC participated in the design of the interviews and recruitment strategy, analysis and interpretation of data, and review of the manuscript. JBJ was responsible for funding acquisition, overall study design, and execution, and participated in data analysis and interpretation, and review of the manuscript.
Author Contributions
The authors gratefully acknowledge Jennifer Pearce, MPA, for revising the interview guide to ensure it was consistent with principles of plain language communication, and Hans-Peter Goertz for providing helpful feedback on data analysis and interpretation.
Availability of Data and Material
Data can be shared upon request.
Code Availability
Not applicable.
Consent for Publication
The authors confirm all patient/personal identifiers have been removed or disguised so the patient/persons described are not identifiable and cannot be identified through the details of the story.
Consent to Participate
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
All procedures in this study were conducted in accordance with the Sutter Health Institutional Review Board (2018.057EXP) approved protocols.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was funded by Genentech, Inc., a Delaware corporation, South San Francisco, CA.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.