
Abstract
This study explored the factors contributing to discontinuation of people who smoke (PWS) from quit smoking clinic prior to achieving 6-month abstinence. Fifteen active PWS were interviewed via telephone and face-to-face. Interviews were audio-recorded, transcribed and analysed using thematic analysis. At individual level, low intrinsic motivation including unreadiness to quit, low self-efficacy and ambivalence on smoking cessation were barriers to attain successful cessation. Influence of extrinsic factors such as work-related factors, social interaction and ill-health burden lead to poor commitment with QSC. At the clinic level, healthcare professional's competency, personal attributes, pharmacotherapy's efficacy, safety and availability were important components that may affect a participant's effort to quit. Working commitment was highlighted as the primary barrier for a successful cessation. Hence, effective intervention and collaborative effort between healthcare facilities and employers are essential to optimise cessation adherence among employees who smoke which subsequently will enhance their abstinence rates.
Introduction
Several control and prevention policies have been introduced in effort to achieve Malaysia's global target for the endgame of tobacco including community empowerment and multi-sectorial collaboration, strengthening the legislation and enforcement of tobacco and other smoking products and enhancing quit smoking services. 1 Quit smoking clinics (QSC) in Malaysia play a critical role in promoting cessation of tobacco use through counselling on smoking and benefits of cessation, assistance on customised quit smoking plan and provision of pharmacotherapy aids to facilitate smoking cessation (SC) with comprehensive follow up sessions by dedicated healthcare professionals (HCP). 2 Currently, there are more than 700 QSCs in Malaysia. 1 Despite the increasing trend of recruitment, high default rate and low abstinence rate were reported. In 2016, Malaysia recorded an overall SC rate of 27.6%, lower compared to the target of at least 35% successful cessation annually at respective public clinic or hospital. In terms of smoking prevalence, a small decline is observed from 22.8% in 2015 to 21.3% in 2019. This limited progress is unfavourable to achieve Malaysia's vision towards becoming tobacco free nation in 2040 with a prevalence of current people who smoke (PSS) tobacco aged 15 years and above of <5%. 1
SC interventions consist of pharmacotherapy and behavioural therapy (brief advice, behavioural counselling, tailored self-help materials). Nicotine Replacement Therapy (NRT) and varenicline are the first line pharmacotherapies recommended in the Malaysian Clinical Practice Guideline (MCPG) for Tobacco Use Disorder. 3 While NRTs are recently exempted (Oct 2020) as non-poison and made available as over-the-counter (OTC) medications, varenicline is still listed in poisons list (Group C) under the Poisons Act. However, varenicline is available as pharmacotherapy offered at the Quit smoking clinic. Systematic reviews and meta-analysis reported that both NRT and varenicline are effective in increasing smoking abstinence rate with low risk of harms.4-6 NRT often causes minor irritation at the site, and in rare cases can cause non-ischemic chest pain and palpitations. 6 Varenicline increased the odds of quitting compared to placebo and was superior to single forms of NRT and bupropion. The main adverse event for varenicline was nausea, at mild to moderate levels and gradually waned off over time. 5 PWS with underlying psychiatric disorder were more likely to experience neuropsychiatric adverse events (NPSAEs) such as hallucinations, delusions, and depressive symptoms.5,7
SC is generally influenced by socio-demographic, smoking and quit attempt history, adverse drug reactions and poor adherence. Currently, there is limited data on factors that contribute to withdrawal from cessation program (CP) among people who smoke in Malaysia. A critical understanding on the relationship between the different aspects involved in SC process is necessary to improve the design and implementation of cessation service. In addition, feedbacks from PWS recruited into SC as the end-recipient of the health service will facilitate understanding on the effectiveness of the service delivered and hence indicate the aspects that require improvement. Thus, this study aimed to explore factors contributing to discontinuation of people who smoke from QSC prior to achieving abstinence
Materials and Methods
Recruitment
Potential participants were identified through four QSCs in Kuala Lumpur, capital city of Malaysia. These four clinics are among the early health clinics which started SC program and have a high registration of PWS with a total of 710 registered between January 2016 to December 2018. Furthermore, these clinics have similar annual quit rate of approximately 30–40% and adhere to the treatment protocol recommended by MCPG for Treatment of Tobacco Smoking and Dependence 2003. An annual quit rate for any treatment centre is defined as the proportion of tobacco users who managed abstinent from smoking for at least 6 months, among those who attempted to quit smoking. This is validated by carbon monoxide monitor reading and self-reported non-smoking status. 3 SC program at these QSCs involves counselling, pharmacotherapies and behavioural support by multi-disciplinary HCP such as the doctors, nurses and pharmacists. Duration of the program vary depending on the individual's needs and progress but typically the program may last for several months with one to two pre-visits, first visit to set the quit date and followed by weekly or bi-weekly and monthly follow up visits. As these QSCs are government clinics, cost for the cessation service is provided at a subsidised cost. 3
Current PWS who have defaulted from SC program at these QSCs were approached for interview by using purposive sampling. Participants were considered eligible if they were 18 years old or older, had an appropriate command of spoken English and/or Malay language, ability to give informed consent, active PWS who have attended SC program and withdrawn from the program before achieving 6-months abstinence, have received at least one pharmacotherapy agent and attended at least three clinic appointments. Medical records of selected PWS were obtained from QSCs to select patient with considerable experience in smoking cessation programme and pharmacologic agent prescribed. In addition., pharmacists in-charge of the respective QSC were approached to request for recommendations of suitable individuals to be interviewed.
Semi-Structured Interviews
Data from participants eligible for this study were collected using semi-structured telephone or face-to-face interview comprising of open-ended questions. The semi-structured interview guide was constantly modified following responses from participants. This interview framework allows exploration of each participant's complex and unique experience with SC program, thus providing diverse and significant data to this study. 8 Data collection was continued until point of saturation was reached and no new insights was given from additional participant interviewed. Hence, data collection at this stage is considered sufficient and has answered the research questions highlighted in this study.9,10
Participants were interviewed individually either in Bahasa Malaysia or English with each interview lasted for an estimated 45 min to an hour. The conversation was recorded by using a recorder application installed in researcher's phone used for telephone interview.
Interview Guide
A semi-structured interview template was used to guide the discussions (Table 1). Interview topic guide was developed based on literature review and discussion with research team. Conversations were initiated by asking about the reasons for joining the SC program and quitting it. The participants were then asked about their experiences using NRT, varenicline or other pharmacotherapy agents and whether they had any difficulty using them or experienced any side effects. To understand their perspectives on the counselling sessions, they were prompted to talk about their experiences with the sessions and support provided by the HCPs. Participants were then prompted to talk about the support they received from family and friends upon joining the program.
Interview Guide in English (Top) and Malay (Bottom).

Data Analysis
Content of each interview recorded was transcribed verbatim into transcript. Interview conducted in Bahasa Malaysia was first transcribed into the spoken language before translated into English. All translated transcripts were checked independently against the original transcription as well as the audio recording to ensure accuracy and manually analysed using thematic analysis approach. Thematic analysis was guided by the six phases of qualitative analysis as described by Braun and Clarke. 11 Themes were then generated based on distinctive expression of related code in the interview transcript. Sub-themes were consequently generated for any theme that showed distinguishing data. To comply with the confidentiality and anonymity protocol of this study, each transcript was named with pseudonyms and stored in password-protected computer. This study was approved by the Medical Research Ethics Committee (Reference No: NMMR-19-232-46224) and Research Ethics Committee, Universiti Teknologi MARA (UiTM).
Results
A total of 15 participants were interviewed from the 4 quit smoking clinics. Of the 15, 93% were male, aged between 24 and 71 years (m = 39.6, SD = 14.3), had completed secondary level of education, and were employed. Two-thirds of the participants had moderate to very high nicotine addiction and received combination treatment of either nicotine patch with gum, varenicline with nicotine gum or varenicline with nicotine patch (Table 2). All participants were interviewed via telephone except for one participant who was interviewed face-to-face. The duration of the interviews ranged from 45 min to an hour.
Participants Characteristics and Smoking Cessation Pharmacotherapies Prescribed for Participants. (n = 15).

Analysis on Factors Leading to Withdrawal From Quit Smoking Clinics
The findings from thematic analysis were organised into themes, sub-themes and categories. Overall, seven themes were identified as factors leading to withdrawing from QSC: intrinsic motivation, influence of extrinsic factors, HCP's competency, HCP's personal attributes, pharmacotherapies safety and efficacy, pharmacotherapies availability and QSC appointment process (Figure 1). The identified themes can be classified into two levels: individual and clinic.
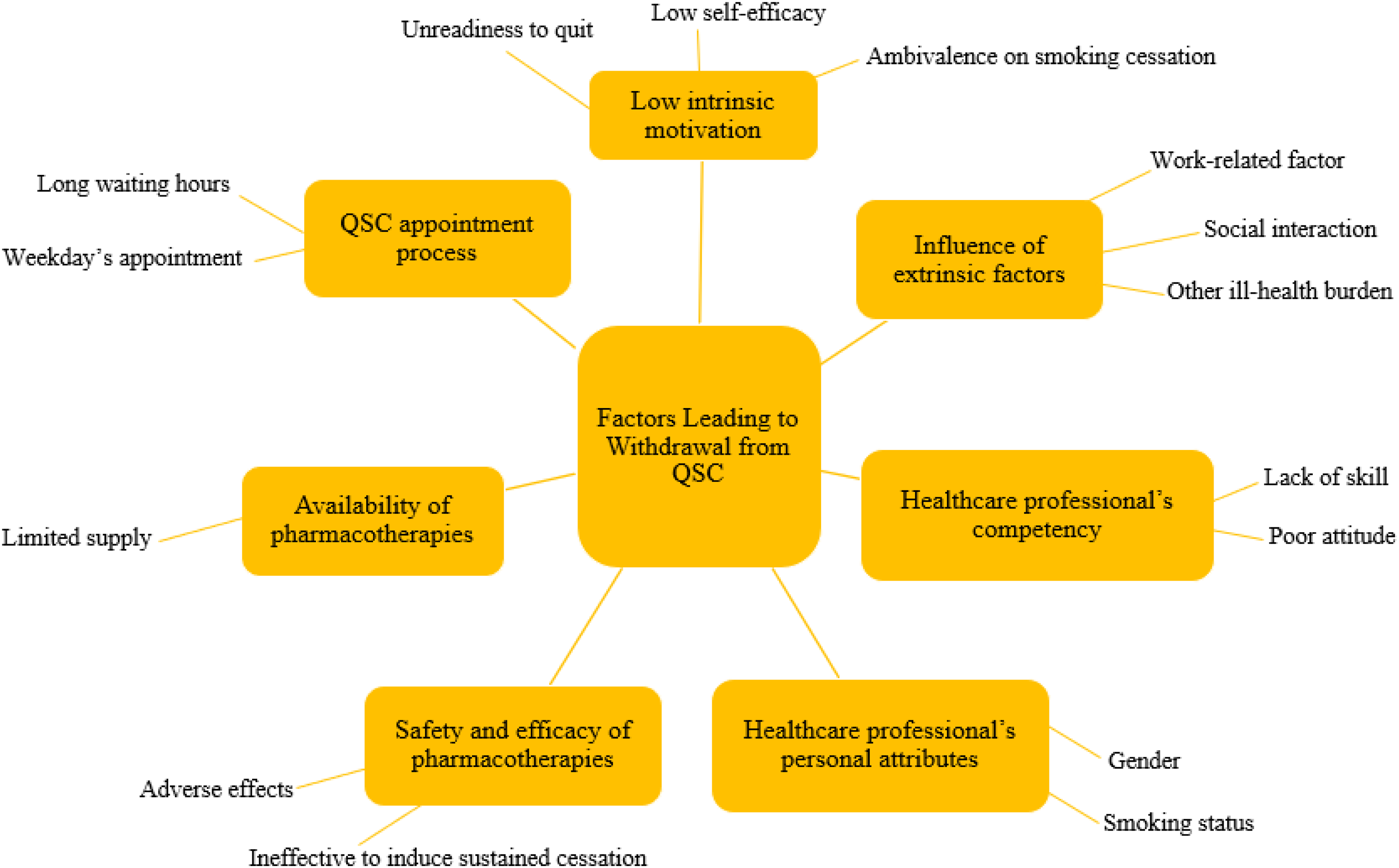
Factors leading to participants’ withdrawal from smoking cessation programme.
Individual-Level Factors Leading to Withdrawal From Quit Smoking Clinics
At individual level, low intrinsic motivation including unreadiness to quit, low self-efficacy and ambivalence on SC were barriers to attain successful cessation (Table 3).
Examples of Individual-Level Factors Leading to Withdrawal from QSCs.

Some participants in this study indicated that they are not ready or committed to quit smoking while others cited not able to quit due to severe addiction. Many participants also reported loss of motivation while going through the cessation process resulting in QSC default. Participants seems to have a low self-efficacy as a consequence of failing previous quit attempt and poor understanding of the objective and process of SC program. These, unfortunately, have led to relapse and defaulting QSC.
Fourteen out of 15 participants claimed health-related concerns as their drive to quit smoking. However, as their health condition improved and they were not experiencing any signs and symptoms of the condition, participants hesitated to continue the CP and subsequently stopped attending QSC. Some participants expressed their lack of confidence on the efficacy of SC aids especially when they are not familiar with the route of administration (ie, patch). On top of that, side effects such as mood swings and poor concentration experienced during the course led participants to quit the program. Consequently, many participants quit without completing the CP.
Influence of Extrinsic Factors
Career, social interaction and other medical conditions played significant role on participant's commitment to QSC. Twelve out of fifteen participants had work commitment on weekdays. Thus, it was difficult for these working participants to manage the overlapped schedules, particularly for a long-term SC program which required a minimum of six months commitment. In fact, this was the primary reason for withdrawing from SC program. Apart from that, stress due to work was another factor leading to relapse and eventually quitting the program. Additionally, smoking culture at workplace has also affected participant's effort to quit and subsequently led to poor commitment to QSC. On a separate note, one of the participants had a history of psychiatric illness (schizophrenia). During her symptoms flare up, she was unable to cope with the QSC schedule leading her to quit the programme. In terms of adverse effect, she reported experiencing mild itchiness with the nicotine patch. However, she did not report experiencing any neuropsychiatric adverse events.
In terms of social interaction, participants cited frequent interaction with friends who smoke compromised their commitments to quit smoking. These interactions had both direct influence in which smoking friends instigated participant not to quit or indirect influence in which participants felt the urge to smoke upon seeing their friends smoking.
Clinic-Level Factors Leading to Withdrawal From QSCs
At clinic level, QSC withdrawal factors are related to the appointment process, HCPs and pharmacotherapies (Table 4).
Examples of Quotes from Participants on Clinical-Level Factors Leading to Withdrawal from QSCs.

Process
Many participants had also reported the process of the QSC appointment as tiresome citing long waiting hours and weekly weekdays visit to the clinic had caused them to give up QSC. This inconvenient process had a significant impact on working participants who had to take leave or time off from work and had to face long waiting hours at the QSC for counselling and collection of medications.
Healthcare Professionals
Some participants claimed that lack of skill and poor attitude of the HCPs led them to withdraw from the program. Participants quoted that the inability of HCPs to provide solutions to their concerns, failure to design an alternative plan in the case of treatment failure, lack of understanding and inconsiderate approach during counselling sessions had discouraged them to continue QSC. Participants voiced their disappointment that the HCPs were not empathetic.
Interestingly, the personal attributes of HCP appear to be an important factor in influencing participants’ confidence on QSC. Participants claimed that female HCPs and those who have not smoked before do not understand the participants’ struggles to quit smoking. One participant quoted that HCPs who do not smoke would merely follow the treatment guidelines due to their lack of experience. In contrast, participants attended by HCPs who had previously smoked reported feeling more comfortable and at ease during counselling sessions.
Pharmacotherapies
Majority of the participants provided positive feedback on the prescribed pharmacotherapies. However, a few participants cited that the therapies failed to induce sustained cessation effect and have caused intolerable adverse effects (AE). These were among the barriers to treatment adherence. In addition, participants also claimed receiving insufficient supply of pharmacotherapies due to limited availability and this affected their quit smoking plan. One participant reported receiving nicotine patch of lower dosage due to the QSC running out of stock of the higher strength and another participant reported receiving insufficient quantity of nicotine gum.
Discussion
Despite the established benefits of pharmacologic and behavioural interventions as well as free-of charge service, PWS in this study withdrew from QSCs prior to achieving 6-month abstinence due to multi-intrinsic and extrinsic factors which vary across the life course of PWS.
Many participants reported low intrinsic motivation due to unreadiness, low self-efficacy and ambivalent thoughts on quitting cigarette. The trans-theoretical model (TTM) of behaviour change is commonly used to assess readiness of PWS to quit including in Malaysia's QSCs. 2 Cessation interventions will be based on stage of readiness of PWS and designed to assist them move forward through the subsequent stages until successful cessation is achieved. 12 Some studies have reported that its limited superiority compared to the non-stage-based equivalents.13,14 However, recent studies showed stage-based interventions are associated with higher continuous abstinence rate, higher probability of forward transition and lower probability of backward transition in the cyclic TTM stages.15-17 Consistent with the TTM conceptual model, our study highlighted that assessment of PWS's readiness to quit is essential to understand their primary barrier and drive to quit as well as to ensure shared decision making on the quitting plan. Following brief assessment, a tailored and effective intervention that match needs of PWS at respective TTM stage should be implemented.
Next, low self-efficacy following failure in previous quit attempt and poor understanding led to participants withdrawing from the program. Self-efficacy has been demonstrated as an important predictor for SC outcome in both aided and unaided quit attempts.18,19 Repeated failures may cause stress and frustration leading to PWS having lower confidence to make or succeed in future attempts. Although a local study showed that quit intent was higher among PWS with past quit attempts, this study findings highlighted retaining high self-efficacy as an essential component for sustained abstinence following quit intent. 20 Due to the dynamic of self-efficacy and smoking urges, HCPs and PWS should work together in maintaining self-efficacy by using effective strategies such as motivational interviewing, cognitive behavioural therapy, health education and intervention to manage withdrawal symptoms. 21 In addition, PWS should be encouraged to reflect on past failed attempt, identifying relapse time points and triggers to work on a customised quitting plan which will increase the possibility of successful cessation in the future. Consistent with previous findings, participants in this study reported ambivalence on SC process following relief of their acute health condition.22,23 Ambivalence is defined as the simultaneous co-occurrence of a strong desire to smoke and a strong wish to quit smoking. Weak initial motivator and incorrect information on cessation process or pharmacotherapies may intensify PWSs’ uncertainty towards achieving successful cessation. 24 Hence, it is important for HCPs to emphasise abstinence as the end goal of CP and educate PWS on correct cessation information and harmful effects of continuous smoking.
Majority of participants in this study reported work commitments as the primary barrier for a successful cessation due to the overlapping weekdays work and QSC schedule and frequent QSC appointments. Finding from this study highlighted the potential role of workplaces and employers to support and promote SC policies. Direct access to large number of PWS and frequent contact due to the long hours at work make workplace an ideal setting for interventions.25,26 In addition, the potential use of peer group support, positive peer pressure and reward system could facilitate cessation interventions.27,28 Workplace-based interventions such as group counselling, pharmacologic treatment and financial incentives have been associated with increased quitting likelihood and long-term abstinence.29-31 Evaluation on cost-effectiveness reported SC measures reduced employees medical care expenditure, lost work productivity and could achieve benefit–cost ratio of up to 8.75, generating 12-month employer cost savings of between $150 and $540 per non-smoking employee.32-34 In view of the sound socio-economic investment, more employers in the United States and European countries have adopted SC initiatives into their health promotion program at workplaces, however, the practice is rather uncommon among employers in the Asian Pacific countries. 35 Therefore, the convenient and strategic framework of workplaces should be utilised to enhance SC effort which is expected to benefits more than 4 million smoking employees in Malaysia. 36
Family members have positive influence on cessation while smoking friends are associated with increased smoking urge leading to relapse and quitting QSC. The effectiveness of family-based interventions has been demonstrated in several studies including higher quit attempt and increased short- and long-term abstinence.37,38 Therefore, involvement of family members in SC interventions should be encouraged as they often drive PWS to attempt quitting and provide emotional support throughout the cessation process. In addition, the stigma of smoking as a sign of manhood, important criterion to be socially connected and valued need to be de-normalised particularly among the young population.
Poor QSC commitment among ill PWS in this study is consistent with previous studies. Stress, low level of motivation, weak support system and limited coping mechanism led to lower quitting rate and increased likelihood of relapse in PWS with psychiatric disorders.39,40 In addition, established data has highlighted increased likelihood of varenicline and NRT NPSAEs in PWS with psychiatric illness at baseline. 7 Therefore, close monitoring is imperative to avoid unwanted event and to ensure adherence to treatment. Collaborative work between HCPs running QSC and psychiatrists is essential to provide intensive and integrative treatment plan which will enhance quitting rate and at the same time allow adequate control on mental health.
The competency, gender and smoking status of HCPs influenced cessation behaviour of PWS in this study. The possible reasons for low competency are the deficiency in cessation training, lack of manpower and limited social and financial support. 41 This is in line with a study by Lee et al where pharmacists highlighted not trained as counsellors for addiction problem. Physicians also emphasised running QSC is an additional work commitment due to the shortage of dedicated staffs. 23 Thus, findings from our study indicated strong need for the inclusion of teaching and training of SC among HCPs including exposure in degree programmes. Practicing HCPs should receive ongoing training to ensure their knowledge and skills are keeping abreast with the latest advancement in SC. Mixed findings were reported for gender influence. Female HCPs are thought to be less experienced and lack understanding in running QSC. 23 In contrast, study by Moxham et. al. demonstrated that gender is irrelevant to successful cessation, however, HCP's smoking status has slight influence on the outcome. 42 Ineffective pharmacotherapies and experience with AEs have been highlighted as reasons to quit CP. Hence, despite the rare occasion of failure to induce cessation and incident of ADR, close monitoring, and timely treatment alteration where necessary are essential for cessation treatment adherence.
Due to participant's preference, majority of the responses in this study were collected via telephone interview. This interview tool result in limited visual communication cues such as participant's facial expression and body language that were important to provide greater understanding on the intended meaning and depth of issues discussed than from verbal answer of the interviewee. However, greater anonymity in telephone interview allowed extensive exploration into the sensitive issue as respondents felt more comfortable to share their responses. As this qualitative study focuses on perspective of PWS, further study may explore other stakeholders’ perspective to present a more comprehensive findings on SC program.
Conclusion
Our study highlighted factors motivating and demotivating PWS to quit smoking particularly work commitment and effectiveness of SC program components including the involvement of HCPs, pharmacotherapies, and the process. Working commitment is one of the major barriers for a successful cessation, and it is imperative to optimise strategies to sustain motivation to quit among this group of PWS . Strategies based on workplace interventions and collaborative effort between healthcare facilities and employers may be considered as this is expected to have a valuable impact on SC outcome.
Footnotes
Acknowledgements
We would like to express our gratitude to all staffs at the quit smoking clinics in which the study was conducted for their kind assistance and valuable insights. We would like to also thanks all participants who have kindly shared their experiences and recommendations for future improvements of smoking cessation programme in Malaysia.
Author Contributions
All authors contributed in designing the study. ZNM analysed and interpreted the data and was a major contributor in writing the manuscript. MK and CFN supervised the research, analysis, interpretation of data and writing of the manuscript. NHI supervised the research at the field. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study received ethical approval from Medical Research Ethics Committee (Reference number: NMMR-19-232-46224) and Research Ethics Committee, Universiti Teknologi MARA (UiTM) (Reference number: 600-IRMI (5/1/6) and REC/297/19).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human and Animal Rights Statement
All procedures in this study were conducted in accordance with the Medical Research Ethics Committee (Reference number: NMMR-19-232-46224) and Research Ethics Committee, Universiti Teknologi MARA (UiTM) (Reference number: 600-IRMI (5/1/6) and REC/297/19) approved protocols.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.