
Abstract
Proactive engagement and care with regular and timely information are required to manage the health and well-being of people in quarantine. At Australia's Howard Springs International Quarantine Facility, a telehealth model was rapidly established using trained non-clinical Customer Service Officers (CSO's) with the aim to provide comprehensive care to residents, maximize staff safety, and reduce clinical workforce capacity pressures. We describe this model, whereby CSO's provided residents with daily COVID-19 symptom and well-being screening, weekly psychological screening, and ongoing linkage to additional clinical and administrative services. In addition, CSO's went beyond these duties to deliver personalized care through delivery of care packages and attendance of the departure point to farewell residents. From October 2020 to May 2021, across 7105 residents, we estimated that CSO's prevented over 75 000 face-to-face resident visits, which reduced workforce requirements and preserved staff safety through minimizing potential COVID-19 transmission and time spent in personal protective equipment in the challenging ambient environment. We share key lessons learned which may inform future telehealth models and guide a positive experience for quarantine residents.
Key Points
Our bespoke telehealth model provided comprehensive case management to residents in quarantine, including COVID-19 close contacts and confirmed cases.
The model assumed a “shared responsibility” between the quarantine staff and resident, whereby residents were promoted to access existing community support, healthcare services, and supplied health promotion resources.
The needs of residents in quarantine ranged from only the required once daily call to contact multiple times a day. Residents that frequently sought support, were most concerned about finances and domestic travel restrictions, rather than other commonly reported concerns of people in quarantine, including infection, frustration, boredom, inadequate supplies, or lack of information.
Telehealth Customer Service Officers went beyond their standard duties to deliver personalized care, such as the delivery of care packages and attendance at the departure point to farewell resident.
There were a range of benefits of the telehealth model that were not quantified, including reduced number of staff required contributing to potential cost savings, reduced face-to-face visits to mitigate potential COVID-19 transmission, and time spent in full PPE in the challenging ambient environment.
Introduction to the Issue
Quarantine is a common control measure used to reduce the spread of infectious diseases such as coronavirus disease (COVID-19). In quarantine, virtual health and support services are recommended to replace face-to-face contact where appropriate, to reduce the risk of disease transmission while maintaining quality care to residents. 1 Negative psychological effects of quarantine are common and there are various well-being strategies recommended to manage mental health.2,3 These strategies emphasize proactive and assertive engagement with regular and timely information, however comprehensive case management with regular wellness checks and linkage to further health services are only described in quarantine for vulnerable populations or residents with confirmed COVID-19.4-7
In the Northern Territory, Australia, the Australian Medical Assistance Team (AUSMAT) established and managed Howard Springs International Quarantine Facility from October 2020 to May 2021. Details on this operation are provided elsewhere. 8 The quarantine facility managed repatriated travellers mandated to complete a minimum 14-day quarantine upon arrival to Australia, including confirmed COVID-19 cases and close contacts. Within 9 days of request by the Federal Government, AUSMAT set-up the quarantine facility with a supporting telehealth call center. The bespoke telehealth model was established based on current literature that described an evidence-based approach effective to reduce the psychological impact of quarantine and cumulative intelligence from lessons learned during AUSMAT quarantine management in early 2020.2,9 Here, we describe the final telehealth model and share lessons learned from the telehealth operations center perspective.
Description of the Intervention
The role of telehealth within the quarantine operation was to be a remote support hub for residents while reducing clinical workforce capacity pressures and preserving staff safety through minimizing potential COVID-19 transmission and time spent in personal protective equipment (PPE) in the challenging tropical savanna climate of the Top End, Northern Territory. 10 Non-clinical Customer Service Officers (CSO's) and Team Leads completed comprehensive training, including 2 days of classroom theory, a 2-day Mental Health First Aid accredited course and 3 days of buddy shifts. The telehealth call center (Figure 1) operated 7 days a week during extended business hours with an average 20 CSO's per day. After hours, residents were able to contact security, an on-call clinician or local emergency services for assistance.

Telehealth governance structure at Australian Medical Assistance Team Howard Springs International Quarantine Facility, May 2021.
CSO's were divided into teams and allocated to a cohort of residents according to their flight and/or physical location at the quarantine facility, where possible. Telephone scripts guided communication with residents, and all telehealth and onsite staff interactions (successful and unsuccessful) were recorded in a custom-built integrated software package, “Covid in Communities” (CIC). Information was used to create a risk profile for each resident in CIC, which was updated by telehealth and onsite staff according to changing needs. Key risk factors were a history of mental illness, drug and alcohol misuse, recent or expected bereavement, travelling with dependent children, physical illness or disability, culturally and linguistically diverse people, confirmed COVID-19 cases and close contacts completing additional quarantine time. CSO's spoke a range of languages (French, German, Hindi, Punjabi, and Telugu), although this was not a requirement for employment as local translation services were available.
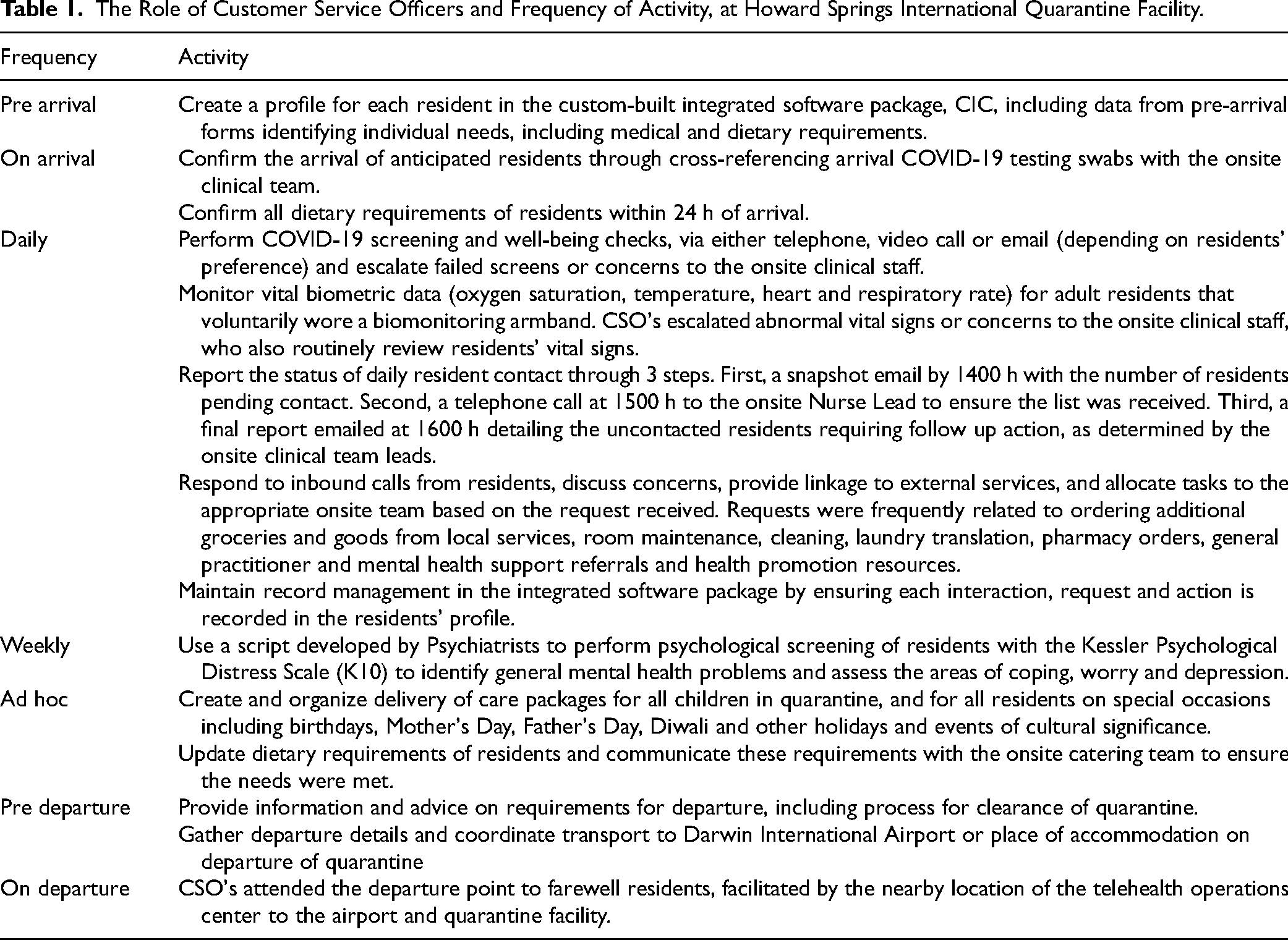
The primary responsibility of CSO's was to maintain daily contact with residents to monitor general well-being, including COVID-19 symptoms, and to complete weekly psychological screening of residents (Table 1). CSO's escalated concerns to their Team Lead who notified the onsite clinical team to determine the required action, such as immediate medical assistance, face-to-face consultation or COVID-19 testing. Onsite support included psychiatrists, medical officers, nurses, midwives, and paramedics. In addition to telehealth screening, residents received a minimum 3 face-to-face clinical visits: once for a welfare check and twice for COVID-19 testing, and all confirmed COVID-19 cases received daily face-to-face clinical visits.
The Role of Customer Service Officers and Frequency of Activity, at Howard Springs International Quarantine Facility.
Evidence of Impact
From 23 October 2020 to 31 May 2021, across 7105 residents, telehealth communications included 85 060 outbound calls, 53 705 outbound text messages, 4356 inbound calls, 1596 inbound text messages. We estimated that CSO's prevented over 75 000 face-to-face visits (Supplemental Appendix 1). Further benefits not quantified were reduced number of staff required contributing to potential cost savings, reduced face-to-face visits to mitigate potential COVID-19 transmission and time spent in full PPE in the challenging ambient environment. Below we provide lessons learned.
An Iterative Model—“Learn As You Go”
The telehealth model was iteratively adapted throughout the operation due to the rapid nature of the request for AUSMAT to establish and manage the quarantine facility. As the operation progressed and expanded, the telehealth model was adapted to changing risk and needs, such as the employment of an on-site psychiatrist to provide immediate clinical mental health care.
Build a Skilled Workforce to Address the Gap
With local and global healthcare workforce shortages, our strategy was to build a workforce to address this gap. We used non-clinical CSO's, with minimal experience in healthcare or quarantine settings. The CSO key selection criteria focused on “flexibility, adaptivity and interpersonal skills,” resulting in employees from a variety of backgrounds, from truck drivers to teachers. We focused on equipping staff with the required training, while providing adequate support and escalation through a command-and-control structure. There was benefit to coincidentally have 2 clinical staff within the telehealth team, however the non-clinical background of CSO's assisted them to remain within scope of their role and escalate concerns to the onsite team for all clinical decision-making.
Varied Utility of Technological Tools
We utilized a custom-built integrated software package, CIC, to manage the resident's journey from pre-arrival to departure to enable real-time systems adaptability to meet operational needs. While this may not be feasible in all contexts, the custom-built software had high utility to improve workflow between telehealth and onsite staff. Conversely, we found the monitoring of vital signs to have overall low utility because our population were, in general, physically well. The monitoring of vital signs would be more beneficial for residents at higher risk of illness, such as COVID-19 confirmed cases or close contacts. Furthermore, we did not use landlines to contact residents due to cost, no text message capacity and infection prevention control concerns. While we offered free SIM cards to residents on an as needs basis, we recommend telehealth services provide all residents a free SIM card on arrival to mitigate potential connectivity issues with residents existing SIM cards.
Implementation of Various Well-Being Strategies
The telehealth model assumed a shared responsibility between the staff and resident, whereby residents were promoted to access usual community support, engage with existing relationships, utilize supplied health promotion resources, and utilize telemedicine with existing general practitioners and mental health services. This contributed to the protection of resident well-being, along with operational decision-making to permit family cohorting, provision of a detailed welcome pack with information on what to expect and how to get assistance, ability to use an outdoor balcony to access fresh air, and frequent COVID-19 testing to ensure infection was detected early and quarantine duration was minimized. We also found the simple act of providing care packages made residents feel connected and in receipt of personalized care.
Recurrent Patterns of Resident Needs
While all residents had unique needs, recurrent patterns of resident needs were evident. Reoccurring concerns were finances, domestic travel restrictions, and food preferences, which differ from frequently reported concerns of people in quarantine including infection fear, frustration, boredom, inadequate supplies, and lack of information.4-7 Financial concerns often stemmed from residents returning to Australia out of necessity due to overseas job loss during the pandemic, and the compounding concern of quarantine costs. Residents also returned to Australia out of necessity due to unwell or dying family members; and many were impacted by domestic travel restrictions within Australia. CSO's were able to use their training to provide immediate emotional support and were adequately informed to provide referrals to mental health and financial support services. The multicultural nature of our residents increased demands made around food preferences. As food plays an enormous role in experience, CSO's spent a large proportion of their time working to meet all requests, however we would not recommend this approach, particularly in lower-resource settings.
Early Intervention Facilitated by Building a Bond Between Staff and Residents
The cohorting of CSO's with residents for their quarantine period facilitated rapport building and led to improved opportunities for early intervention in health needs. The non-negotiable daily check-in by method of resident's choice permitted residents to engage with support services at the level they needed. Regardless of the level of engagement, there was a universal appreciation to have a centralized service readily available for assistance. While there was no formal evaluation of the telehealth model performed, residents regularly communicated appreciation by telephone and email. The personalization of telehealth services resulted in the formation of a strong bond between staff and residents, leading to CSO attendance of the quarantine departure point to farewell residents, which was very much appreciated by residents.
Conclusions
The telehealth model implemented by AUSMAT at Howard Springs International Quarantine Facility provided comprehensive care to residents while preserving clinical workforce resources and prioritizing staff safety through minimizing potential COVID-19 transmission and time spent in PPE in the challenging ambient environment. The quarantine experience will be different for everyone, however the described model and lessons learned may inform the establishment of future telehealth models and guide a positive experience for quarantine residents.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231183669 - Supplemental material for Telehealth for Comprehensive Care to Quarantine Residents: A Novel Approach and Lessons Learned
Supplemental material, sj-docx-1-jpx-10.1177_23743735231183669 for Telehealth for Comprehensive Care to Quarantine Residents: A Novel Approach and Lessons Learned by Stephanie J. Curtis, Ronnie Taylor, Lynette Perry, Abigail Trewin, Karen Were, Nick Walsh and Kathleen McDermott in Journal of Patient Experience
Footnotes
Acknowledgments
We thank all residents and staff at Howard Springs International Quarantine Facility for their contribution in creating a safe and successful operation. NCCTRC are funded by the Federal Department of Health and Aged Care, the operation at Howard Springs International Quarantine Facility was funded by the Australian Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.