
Abstract
Patients living with headache diseases often have difficulty accessing evidence-based care. Authors conducted a qualitative research study with 20 patients receiving headache care at seven Headache Centers of Excellence within the Veterans Health Administration to examine their experiences navigating headache care. This study employed thematic qualitative analysis and conducted cross-case comparisons. Several key findings emerged. 1) Most patients saw multiple healthcare providers over numerous years before reaching a headache specialist to manage chronic headaches. 2) Receipt of high-quality and comprehensive headache specialty care was associated with high satisfaction. 3) Patients with headache diseases reported oftentimes they experienced an arduous journey across multiple healthcare systems and between several healthcare providers before receiving evidence-based headache treatment that they found acceptable. Results demonstrate that most patients were satisfied with their current specialty headache care in the Veterans Health Administration. Authors discuss implications for future studies and highlight ways to improve patient satisfaction and timely access to appropriate headache care.
Keywords
Background
Worldwide, nearly three billion people live with either migraine or tension type headache alone (1). Severe headache or migraine are highly prevalent in the United States (U.S.), with the most recently reported age-adjusted prevalence in the U.S. being 15.9% (2). In fiscal years 2008 through 2018, approximately 16% of patients cared for within the Veterans Health Administration (VHA) had a documented headache disease (3). Veteran patients with headache disease are likely to have medical comorbidities that may contribute to their symptoms which add to the complexity and navigation of care, including traumatic brain injury (TBI), post-traumatic stress disorder (PTSD), depression, back pain, and neck pain (4–6). Additionally, many individuals struggle to find the care they need and treatments that provide satisfactory symptom relief from the healthcare system (7–10). In one study, only 25% of respondents with chronic migraine who reported consulting a healthcare professional received an accurate diagnosis, and only 44% received both acute and preventive pharmaceutical treatments (8). Further, healthcare utilization and cost are high for US patients with migraine, who spend thousands of dollars more on healthcare per year than patients who do not experience migraine disease (11,12).
In 2018, the Headache Centers of Excellence (HCoE) program was funded and developed within the VHA as part of a congressionally mandated program to improve care quality and delivery for veteran patients with headache disease (13). To inform HCoE best practices for the delivery of headache care, authors conducted a qualitative stakeholder assessment with veteran patients diagnosed with at least one headache disease for which they received care during the past year in a VHA HCoE facility across the United States. The overall objective of the study was to elucidate the complex navigation of the healthcare system for patients with chronic headache disease seeking symptom management in the VHA. The specific aims of this study were to evaluate how veteran patients with chronic headache navigated both the VHA and other healthcare systems to access headache specialty care; examine veteran patients’ self-reported headache management, preferences, and satisfaction with headache care received; and compare patient characteristics associated with access to headache specialty care and satisfaction.
Methods
Design
The authors conducted a cross-sectional, qualitative, semi-structured interview study among veteran patients with chronic headache disease who had received headache care in the VHA HCoE facilities in 2019. The authors followed the Consolidated Criteria for Reporting Qualitative Studies (COREQ) research guidelines (14) (See Supplemental Appendix 1).
Sample and Data Collection
Authors recruited for a heterogeneous, purposeful sample (15) of veteran patients who were diagnosed with a headache disease and received care at any one of the VHA HCoE sites. The full details of this study's recruitment methods are reported elsewhere (16). Co-authors (JJS, TMD, HML, REG) developed an interview guide with semi-structured questions based on clinical experience and identification of gaps in the literature about headache care navigation, treatment preferences, and satisfaction (See Supplemental Appendix 2). Semi-structured interviews were conducted between June 2019 and November 2019 by three co-authors (TMD, HML, REG) who hold a BA or PhD degree, had experience conducting qualitative interviews, and were coached in the interview protocol. Additionally, a medical chart review was conducted by a co-author (JJS) to collect participants’ demographics, headache diagnoses, medically diagnosed comorbidities, and psychiatric diagnoses. This study used the medical chart review data to characterize the sample and conduct cross case comparisons. Further details regarding data collection are reported elsewhere (16).
Ethical Considerations
The VA Connecticut Healthcare System Institutional Review Board approved this research study, #JS0006. This study received a wavier for informed consent and waiver of HIPAA authorization. Patients were informed that the purpose of the interview was to learn about their experience with a headache disease to inform the HCoE initiative. Patients provided verbal consent to have the interview audio recorded.
Qualitative Data Analysis
All interview recordings were professionally transcribed, de-identified, and imported into NVivo 12 software (17). Using a template style organizing approach (18), analysis team members (TMD, HML, and REG) created a defined codebook based on the interview guide and trial with a selection of transcripts. Each transcript was then coded independently by two coders (SB, HML, SDR, or LB) using NVivo. The two coders for each transcript reconciled any disagreements with assigned codes until they reached a consensus. Authors then conducted thematic content analyses to identify emergent patterns and themes within and across transcripts related to the patient navigation of the healthcare system for headache care (19).
Authors subsequently conducted case comparisons of participants’ categorized responses to perceived headache treatment received and headache care satisfaction stratified by age or sex. This study utilized these variables in case comparisons because they relate to participant experiences with headache disease and healthcare systems. Several studies suggest that responses to pain, pain expression, and responsivity to pain treatments vary by sex (20).
Results
Demographics
Healthcare providers referred 30 veteran patients for participation in this study. Ten of the referred veteran patients were excluded from this study for the following reasons: eight did not respond to the invitation to participate, one was not a veteran, and one did not have a headache diagnosis. The final sample included 20 (67% recruitment) veteran patients with headache diagnoses from seven VHA HCoE facilities. Sixteen veteran patients were men (80%) and four were women (20%). The mean age of participants was 54 years (SD = 13.77). Participants had a mean of 1.4 (SD = 0.68) distinct headache diagnoses. Fifteen veteran patients had a migraine diagnosis, seven headache not otherwise specified, three tension-type headache, one cluster headache, one post-traumatic headache, and one medication overuse headache (diagnoses were not mutually exclusive). Twelve veteran patients reported that their headache began shortly after a head or neck injury, including 11 men and one woman. Other veteran patients reported that they began experiencing headache after the onset of puberty (N = 1) and following serious medical events (N = 1), while some did not recall when their headaches first started (N = 2) or did not provide contextual information (N = 4).
Thematic Content Analyses
Perceived Navigation Challenges
The identified overarching theme was that veteran patients with headache disease found navigating through the healthcare system to be challenging. Four sub-topics comprised this theme: the pathway to specialty headache care; headache management and preferences; satisfaction with headache treatment; and satisfaction with headache care received from the VHA HCoE. Veteran patients reported healthcare navigation challenges due to debilitating headache symptoms that were often refractory to treatments, multiple medical conditions that required extensive care and were often contraindications to headache treatments, and poor co-management of their headache disease among different providers. Illustrative quotes are presented in Table 1.
Illustrative Veteran Quotes.
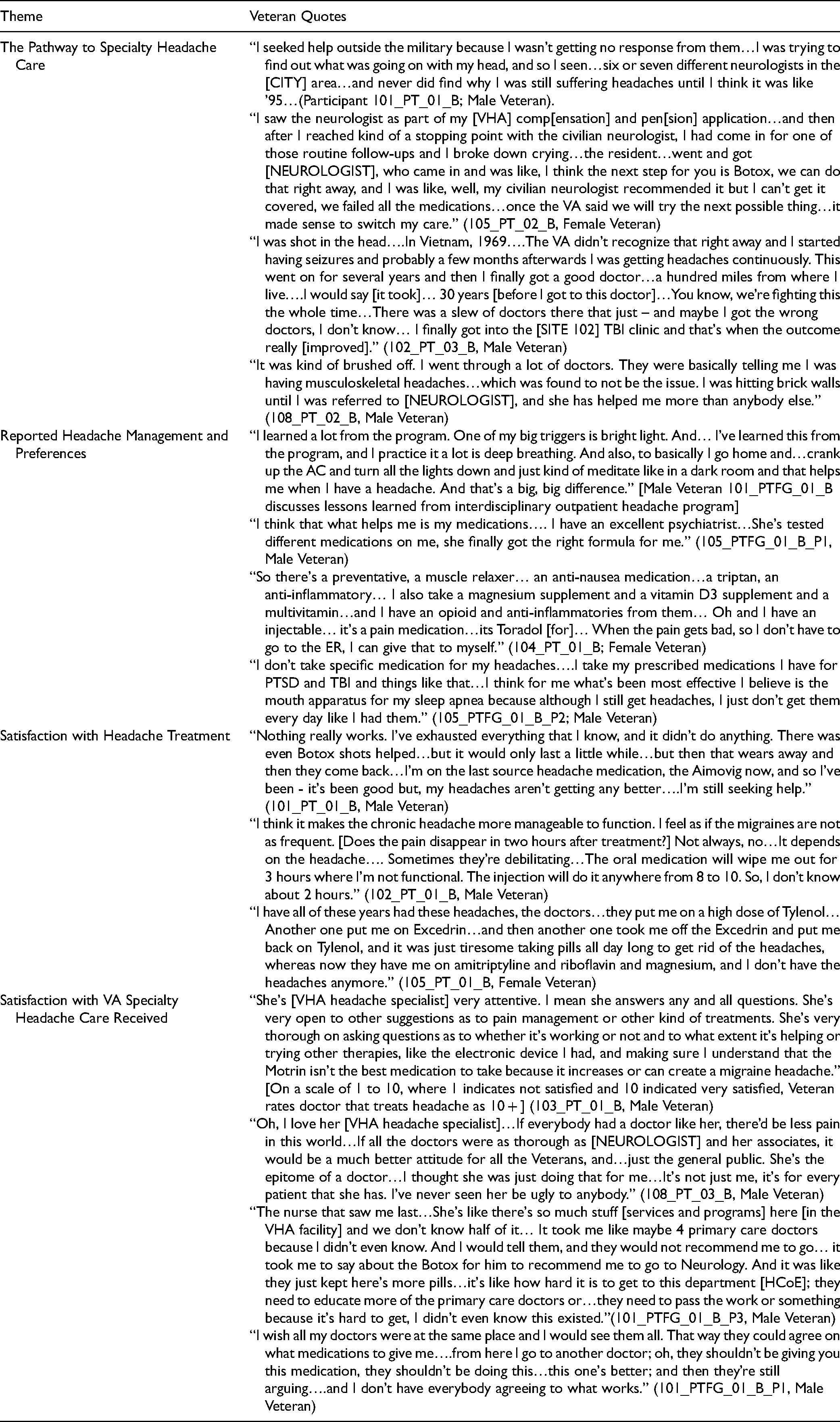
The Pathway to Specialty Headache Care
Veteran patients reported that they consulted multiple providers (upwards of 10 or more providers) over time in the community, Department of Defense (DoD) during active duty, and/or the VHA prior to reaching their current VHA HCoE headache specialist(s) (See Figure 1). Veteran patients traversed various pathways to ultimately arrive at their current specialty VHA headache care. Twelve first sought care in the VHA and were referred to specialty services for headaches or another neurological problem. Five first sought care in the military, later received care in the VHA and were referred to a VHA headache specialist. Three first received headache care in the community and switched to the VHA for better access to headache treatments. Last, 10 veterans exclusively received their headache care in the VHA. These veteran patients were referred for headaches or another neurological problem to neurology and other specialty services by primary care, social workers, and/or members of a mental healthcare team.

Headache care trajectory.
All the veteran patients in this sample were referred to additional headache specialists because their referring provider exhausted treatment options or resources, dissatisfaction with treatment, and/or had difficulties with access to treatment such as lack of insurance coverage. One veteran was dissatisfied with headache care he received in the military and sought community care prior to military discharge. Another veteran sought treatment from a community care neurologist after military discharge but ran out of treatments to try that were covered by her medical insurance. This veteran eventually accessed evidence-based headache care within the VHA. Several other veteran patients had medical comorbidities that required care from multiple healthcare providers whose recommended treatments were contraindications to some headache treatments, complicating headache management. Moreover, veteran patients reported delays in referrals to specialty care and prescription of treatments due to poor care coordination between healthcare providers, lack of healthcare provider knowledge about available, evidence-based headache treatments, and healthcare provider prioritization of other medical conditions.
Authors conducted cross-case comparisons and found differences in the pathway to specialty care based on veteran patients’ characteristics. Self-reports of healthcare navigation/pathway from men and women showed that women reported that they saw fewer providers than men did before being referred to a headache specialist. Additionally, veteran patients who reported consulting more providers before being referred to a headache specialist were older on average. Lastly, veteran patients who first sought headache care in the VHA consulted fewer providers than did veteran patients who first sought headache care in the military or community.
Reported Headache Management and Preferences
Veteran patients self-reported trying a variety of headache treatments singularly and in combination. Reported treatments included abortive and preventive oral medications, a selection of complementary and integrative health treatments, and botulinum toxin injections. Nearly half of the sample had tried all or most treatments available to them. Most veteran patients reported using a combination of pharmaceutical and non-pharmaceutical therapies. Several participated in interdisciplinary outpatient headache or pain programs that provided comprehensive care and instruction on self-management techniques and factors that contribute to headaches. Most veteran patients wanted to reduce the number of pills they were taking, preferred treatments that provided relief without major side effects, and were amenable to nonpharmaceutical modalities, while some veteran patients reported that their medications were what helped them the most. Veteran patients found headache education to be helpful, and often continued to practice self-management techniques after the completion of programs or treatments. Cross-case comparisons revealed veteran differences in the self-reported amount of headache treatments tried by sex; women reported trying more headache treatments than men did.
Satisfaction with Headache Treatment
Veteran patients reported mixed results with both pharmaceutical and non-pharmaceutical prescribed therapies that they had tried for their headache disease(s). Six veteran patients described that their overall treatment was not very effective. Some of these veteran patients had tried all or most of the treatments available to them with little relief, and therefore they were skeptical about the potential efficacy of newer treatments and frustrated by the lack of significant symptom resolution. Seven veteran patients described some relief from their treatments. Treatments improved their headache management, but they were debilitated at times due to their symptoms or side effects of treatment. Six veteran patients reported that their headache treatments were very effective in relieving headache symptoms. Some were especially pleased with their current treatments because they experienced significant symptom relief and were able to reduce their medication use.
Satisfaction with VA Specialty Headache Care Received
Thirteen veteran patients were very satisfied with their current headache providers. Veteran patients liked that their providers employed a variety of different headache management approaches, were knowledgeable, and educated them about headache dieases. Some veteran patients were especially appreciative of their provider's attentiveness and caring attitude toward them. However, other veteran patients were dissatisfied and frustrated because they had trialed several treatments without significant symptom relief, and were aggravated by co-management of their headache care at the VHA. One patient struggled to get a neurology referral from primary care, and another patient's providers did not agree on which headache treatments to prescribe. Further, six veterans reported that earlier in their care, it had seemed like healthcare providers had not listened to them and initially had “brushed off” their concerns regarding headaches. Once these veteran patients had reached specialty headache care, they felt more satisfied with their care and that their headache diseases were being well-addressed. Cross-case comparisons showed differences in treatment satisfaction by sex. Women tended to report greater satisfaction with their care than men did.
Discussion
This study presented findings about the perspectives of veteran patients on their experiences navigating healthcare systems, and receiving headache care. Most veteran patients in this study had suffered from headache disease for years, saw multiple providers, and tried numerous treatments before finding their current care at a VHA HCoE. Some had found symptom relief through pharmaceutical and/or non-pharmaceutical therapies, while others continued to have debilitating symptoms and sought additional treatments and management strategies. Many reported receiving multiple headache treatment options and high satisfaction with specialty headache care within the HCoE program.
In studies outside of the VHA, patients with headache diseases also struggled to find appropriate medical care, and described arriving at their headache diagnosis as a long and tortuous process (8,9,21). In this study, veteran patients’ difficulties finding specialized headache care may be due to delays in getting a headache referral, a lack of non-specialist provider education about headache diseases, and/or complex medical histories that complicate headache care. Additionally, transitioning from one healthcare system to and through another healthcare system may contribute to delays in patients receiving high-quality headache care. In other studies, patients reported that some of their providers, most of whom were general practitioners, were dismissive or uninterested in their headache disease (21–24). This prior research greatly contrasts with the current study's findings of high veteran patient satisfaction with specialty headache providers, but is similar to veteran patient reports of feeling unheard earlier in their headache care (24). It is possible that struggles experienced by patients differ depending on their level of care (e.g., general practitioner, specialty care) or care setting (e.g., VHA, military, community). Further research is necessary to explore factors that are associated with patient satisfaction and barriers to accessing specialized headache care.
Broader headache education among non-specialist providers may reduce knowledge gaps and in turn, facilitate headache-specific treatment and patient headache education earlier in care and referrals to headache specialists where appropriate (25–29). Authors suggest that education include the topics of headache evaluations and diagnosis, older and new treatments available for various headache disorders, treatment contraindications, and when and/or how to make referrals to headache specialists. Means of delivering headache education should be multimodal, including brief didactic videos, and written headache care summaries, where providers can also receive continuing medical education credit for staying current on advances in headache management. Additionally, more comprehensive education on available headache treatments and self-management strategies provided to people living with headache diseases could potentially facilitate earlier treatment seeking and increased utilization of evidence-based headache care. There is evidence that therapeutic patient education alone can improve quality of life and levels of disability, and decrease the frequency of headache episodes (30). Further, a better-defined headache care pathway from primary care to headache specialty care may especially help facilitate appropriate referrals and make healthcare navigation easier for patients with headache diseases. Clinical care pathways focusing on care quality and safety in headache management for national healthcare system models have been proposed elsewhere (31). Clear and timely communication between providers who care for patients with headache is essential to improve care coordination and expedite treatment referrals and prescriptions.
Men in this study as compared to women reported that they tended to see more providers before they reached a headache specialist, had tried fewer headache treatments, and perceived less satisfaction with their headache treatments received and care provided. A greater percentage of men than women had headache diseases that were temporally related to accidents and therefore, they may have had more complicated health histories and treatment contraindications related to the injury, such as TBI, back, and neck injuries. Moreover, there may have been differences in care-seeking between men and women. Prior studies found that men are less likely to seek help for headache diseases and other medical conditions than women due to a perceived need for autonomy and control; negative emotions about seeking healthcare; not recognizing their need for health services and delaying medical care; workplace factors; and gender role norms (32–35). Additional research is needed to better understand why differences were found between men and women in this study, and the role of head and neck injuries.
Most veteran patients in this study were looking for symptom relief to improve functioning and quality of life. Many veteran patients discussed the self-management techniques they used for symptom relief, such as meditation. Patients’ desire to be involved in their care and use of multiple self-management techniques has been observed in previous research (9,21,23,24,36,37). Patients preferred a patient-centered approach with their providers and were willing to test any strategy or treatment their providers thought might help (9,21,23,24,36,37). Veteran patients in this study especially appreciated providers who were attentive, showed that they cared, and took the time to educate patients about headache disease and self-management techniques.
Veteran patients in this study described difficulties establishing care for their headache diseases, which reflects findings from prior research. The current study highlighted findings that suggest that there are differences in healthcare utilization and satisfaction between men and women, which contributes to emerging literature on the healthcare experiences of men with headache diseases. Enhanced patient and provider education initiatives could potentially improve access to and utilization of various evidence-based headache treatments. Veteran patients reported seeking multiple treatment modalities and strategies to support their headache management. Once veteran patients had access to and received comprehensive headache care, they reported high degrees of satisfaction with treatment and their headache care providers.
Limitations
Authors interviewed a small, purposeful sample of veteran patients who were referred to this study by their VHA HCoE providers and received most of their headache care in a VHA HCoE. Non-VHA patients may have different experiences due to the unique characteristics of VHA patients and the system of care. Additionally, as is typical of small qualitative studies, this study was unable to make more definite associations in analyses. Since specialized headache centers typically see patients with more refractory headache, some of these findings may be less applicable to patients with less severe headache diseases (38,39). The sample in this study mostly consisted of non-Hispanic, white men, and a small number of women, which limited comparisons between genders. Another strength of this study is that it elucidated experiences of veteran patients in their own words about their headache care over time. Future studies should explore the experiences of headache care with a broader sample of participants, and examine potential differences across demographic groups, in individuals with injuries temporally related to headache development, across non-veteran and veteran populations, and within different healthcare delivery systems.
Conclusions
Veteran patients with headache disease experienced difficulties navigating through headache care services across healthcare systems throughout their lifespan in community care settings, DoD, and within the VHA integrated healthcare system. Most veteran patients reported they were satisfied with high-quality and multifaceted care as well as their headache care providers. However, some described frustrations with coordination of care across services. Further research on improved headache care pathways and care coordination is needed to improve patient access to high-quality and guideline-concordant treatments for headache diseases.
Supplemental Material
sj-doc-1-jpx-10.1177_23743735231151547 - Supplemental material for Complex Patient Navigation by Veteran Patients in the Veterans Health Administration (VHA) for Chronic Headache Disease: A Qualitative Study
Supplemental material, sj-doc-1-jpx-10.1177_23743735231151547 for Complex Patient Navigation by Veteran Patients in the Veterans Health Administration (VHA) for Chronic Headache Disease: A Qualitative Study by Hayley M Lindsey, Roberta E Goldman, Samantha D Riley, Sean Baird, Laura Burrone, Amy S Grinberg, Brenda T Fenton, Jason J Sico and Teresa M Damush in Journal of Patient Experience
Supplemental Material
sj-doc-2-jpx-10.1177_23743735231151547 - Supplemental material for Complex Patient Navigation by Veteran Patients in the Veterans Health Administration (VHA) for Chronic Headache Disease: A Qualitative Study
Supplemental material, sj-doc-2-jpx-10.1177_23743735231151547 for Complex Patient Navigation by Veteran Patients in the Veterans Health Administration (VHA) for Chronic Headache Disease: A Qualitative Study by Hayley M Lindsey, Roberta E Goldman, Samantha D Riley, Sean Baird, Laura Burrone, Amy S Grinberg, Brenda T Fenton, Jason J Sico and Teresa M Damush in Journal of Patient Experience
Footnotes
Availability of Data and Materials
The data used and analyzed during this current study are not publicly available because they must remain on the Department of Veteran Affairs (VA) servers. A limited de-identified data set may be available upon request and fulfillment of the VA data use agreements.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the VHA Headache Centers of Excellence
Ethical Approval
This study was approved by the VA Connecticut Healthcare System Institutional Review Board, West Haven, CT (#JS0006).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the VA Connecticut Healthcare System Institutional Review Board (#JS0006).
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained because we received a wavier for informed consent and waiver of HIPAA authorization.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.