
Abstract
The purpose of this work is to understand Emergency Department (ED) clinicians’ experiences in communicating uncertainty about first-trimester bleeding (FTB) and their need for training on this topic. This cross-sectional study surveyed a national sample of attending physicians and advanced practice providers (APPs). The survey included quantitative and qualitative questions about communicating with patients presenting with FTB. These questions assessed clinicians’ frequency encountering challenges, comfort, training, prior experience, and interest in training on the topic. Of 402 respondents, 54% reported that they encountered challenges at least sometimes when discussing FTB with patients where the pregnancy outcome is uncertain. While the majority (84%) were at least somewhat prepared for these conversations from their training, which commonly addressed the diagnostic approach to this scenario, 39% strongly or moderately agreed that they could benefit from training on the topic. Because the majority of ED clinicians identified at least sometimes encountering challenges communicating with pregnant patients about FTB, our study indicates a need exists for more training in this skill.
Introduction
Unaddressed diagnostic uncertainty can have deleterious effects on patient well-being and satisfaction. Patients of all genders discharged from the emergency department (ED) with persistent uncertainty related to their symptoms report feelings of fear, frustration, and anxiety (1,2). They describe lack of reassurance by normal test results in the setting of ongoing symptoms (3,4), with some patients noting heightened fear of severe medical issues in the setting of ongoing symptoms despite this information (2). As a result, many patients report the intention to continue to seek care until they receive more answers (5). For clinicians, uncertainty has been associated with differing practice patterns (6) including increased test ordering and charges (7).
About one-fourth of pregnant women will experience vaginal bleeding in their first trimester (8). In the US, vaginal bleeding in early pregnancy represented 1.6% of all ED visits over an 11-year period of investigation – nearly 500 000 visits per year nationally (9). Uncertainty is particularly common for pregnant patients who present to the ED with first-trimester bleeding (FTB). While some causes of FTB may be non-obstetric, bleeding may occur with a viable intrauterine pregnancy, an ectopic pregnancy, or a miscarriage (8). Patients who presented to the ED with FTB commonly expected an ultrasound and bloodwork to be performed and wished to understand definitively if they were having a miscarriage (10). Unfortunately, initial diagnostic measures of FTB are often inconclusive, leaving clinicians unable to confirm the location and/or the viability of the pregnancy. Understandably, FTB is often quite distressing to the patient, and uncertainty appears to compound its anxiogenic effect (10,11).
Some research exists on the adequacy of clinician training in managing FTB and communicating a confirmed diagnosis of early pregnancy loss (EPL). Past work has examined shared decision-making related to EPL (12), provider education about the patient impact of EPL (13), training for delivering the news of EPL (14,15), and patient perceptions of optimal EPL communication (16,17). Uncertainty is mentioned explicitly by patients as contributing to self-blame in EPL (18) and is noted to be present during their evaluation (19) and after discharge (20). Uncertainty is also mentioned by patients as a driver for return visits for re-evaluation of EPL (21). To our knowledge, there is a paucity of literature investigating how to communicate with patients experiencing FTB when there is still uncertainty about pregnancy viability.
Similarly, there is little reported in the literature related to clinician experiences managing FTB and EPL. One study focused on the experience of clinicians within the obstetrics community, wherein a doctor-patient relationship and continuity of care often exist (22). Another assessed the experience of ED nurses managing EPL, finding that nurses reported feeling ill-equipped to educate and provide guidance in EPL (23). To date, the experience of clinicians in the ED, a frequent site of first presentation for FTB, has not been explored.
The purpose of this work is to understand ED clinicians’ experiences in communicating about FTB and their perceived need for further training in communication of this topic. To accomplish this goal, we surveyed a national sample of ED attending physicians and advanced practice providers (APPs) across a variety of ED practice settings to assess comfort level and perceived adequacy of prior training for communication in the setting of uncertainty in FTB.
Methodology
This study was a survey of ED-based healthcare clinicians designed to assess the clinician experience with communication challenges when caring for patients that present with FTB. It was approved by the Thomas Jefferson University Institutional Review Board (IRB) in Philadelphia, Pennsylvania (approval #20E.747). The survey was built in Qualtrix® software (Qualtrix, Provo, UT). A request to participate and a link to the survey was distributed via email to all attending physicians and APPs employed by US Acute Care Solutions (USACS) via the USACS listserv. It was sent to a nationwide group of attending physicians and APPs who work at their 176 clinical sites, with 3309 recipients on the listserv at the time the survey was distributed. Participants provided written informed consent before beginning the survey. Responses were collected over a 2-month-period from August to October 2020. All listserv members received one e-mail reminder to complete the survey.
The survey included basic questions about background characteristics and demographics, including profession (physician, APP), practice setting, and years of experience (Appendix). It also incorporated four sets of quantitative and qualitative questions assessing clinicians’ perceptions about their frequency encountering challenges, comfort level, prior training, prior clinical experience, and interest in training on the topic. These survey questions inquired about clinicians’ comfort levels with discharging patients with uncertainty in the setting of FTB, the type of training that prepared them to have discharge conversations (ie, formal training and informal training), and interest in more formal training on this topic.
In order to draw meaningful comparisons with past literature, survey items assessing clinicians’ perceptions were adapted from prior work by our team assessing experience with diagnostic uncertainty among resident physicians (24). Questions were tailored only to the extent that they became specific to FTB; for instance, “How well do you feel your medical school training prepared you for having conversations with patients about diagnostic uncertainty?” became “How well do you feel your training prepared you for having conversations with pregnant patients who are experiencing FTB or pain for whom there is an uncertain outcome?” Piloting of survey questions was performed among four clinicians not involved with the study to confirm question clarity and coherence. Each quantitative survey item assessing clinicians’ perceptions had response options using a five-point Likert scale (24). An additional qualitative question was included after each of these items to allow for addition of detail to explain the response selected on the Likert scale.
We limited analysis to fully completed surveys. Demographic and background information was tabulated and summarized. To simplify data presentation and interpretation of results, we report five-point Likert responses in three groupings (eg, agree/strongly agree, neutral, and disagree/strongly disagree). Data analysis for the quantitative questions consisted of computing descriptive statistics for each item. Distributions were examined to check for normality. Associations between training interest and gender and profession (physicians vs APPs) were assessed with chi-square analyses (for categorical data). One-way ANOVA was used to compare mean years of clinical experience by training interest level.
A multivariable logistic regression analysis was employed to better understand the relationship between interest in additional training and demographic characteristics. For this regression model, interest in training was dichotomized into a two-category variable coded as “strongly disagree/disagree/neutral” [0], or “agree/strongly agree” [1] to ensure enough participants in each group.
Open-ended responses were analyzed qualitatively. One coder (GN) reviewed all responses and developed an initial code book. A second reviewer (DMM) then applied that code book to all responses and developed (or refined) codes as needed. The final quotes and codes and resultant themes were presented to the research group for review and further refinement.
Results
Participant Characteristics
A total of 402 participants completed the entire survey (response rate of 12.1%). Participants identified primarily as male (54%) and as attending physicians (79%), with a mean age of 42.7 years (SD = 9.5) and mean professional experience of 12.7 years (SD = 9.3). Two participants identified as “genderqueer/nonconforming.” Nearly all (n = 394, 98%) respondents identified the ED as their primary practice setting. See Table 1 for participant characteristics.
Participant Characteristics.
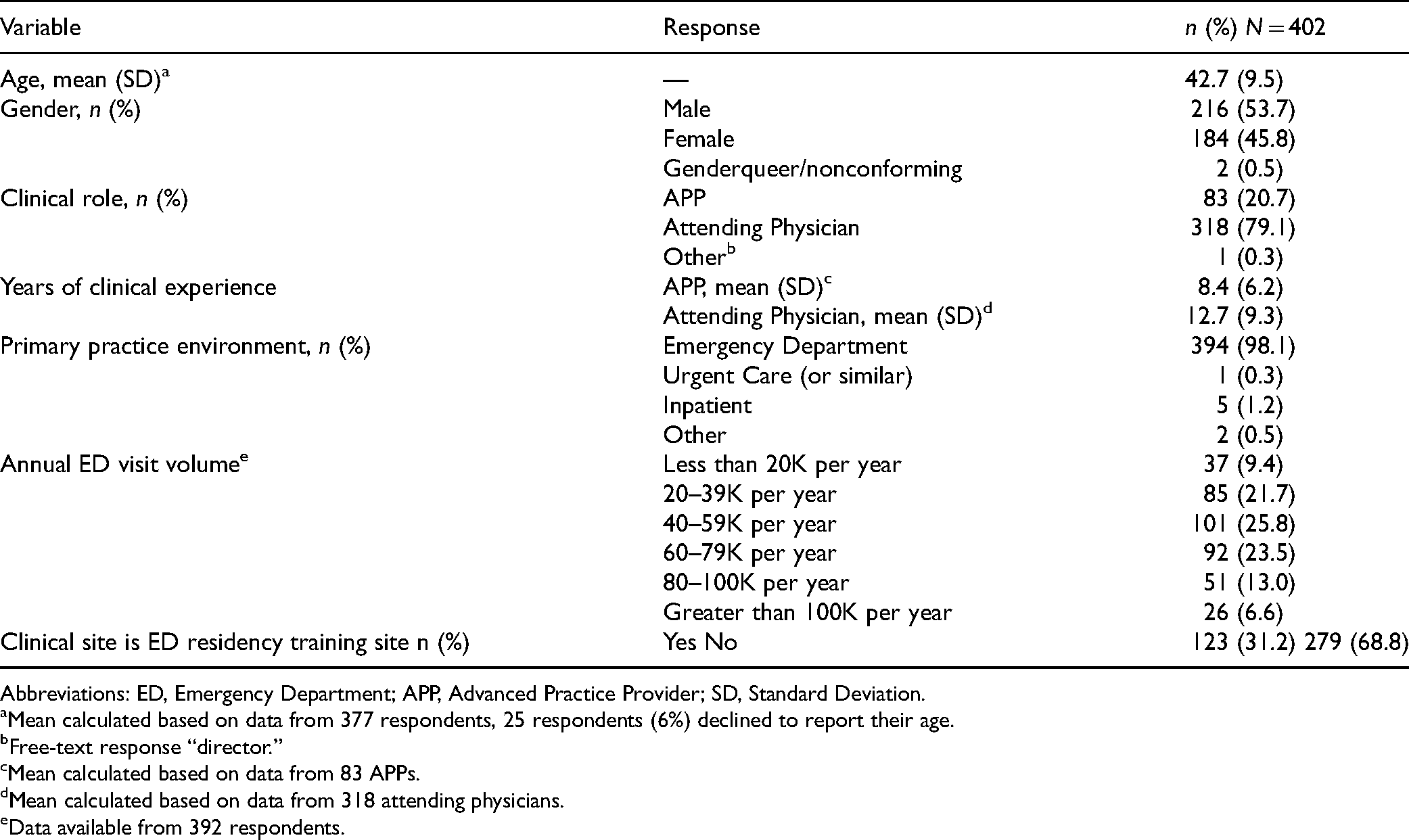
Abbreviations: ED, Emergency Department; APP, Advanced Practice Provider; SD, Standard Deviation.
aMean calculated based on data from 377 respondents, 25 respondents (6%) declined to report their age.
bFree-text response “director.”
cMean calculated based on data from 83 APPs.
dMean calculated based on data from 318 attending physicians.
eData available from 392 respondents.
Survey Responses
Survey responses are summarized in Table 2. Over half (54.0%) of respondents reported that they encountered challenges in communication at least sometimes. The majority (84.1%) of respondents indicated that they were at least somewhat prepared for these conversations as a result of their training, with nearly two-thirds (63.9%) describing their prior training as a combination of formal training (eg, didactics, simulation) and informal training (eg, bedside teaching and mentorship). Most formal training about FTB was focused on the diagnostic evaluation of the patient, rather than on communication skills. Almost all (96.3%) reported that their personal clinical experience (eg, on-the-job training) had “Somewhat” (11.7%), “Fairly well” (55.0%), or “Exceedingly well” (29.6%) prepared them for these discussions. Respondents were split on the desire for more training to aid communication in this patient scenario: while 39.1% strongly/moderately agreed that they could use formal training, 60.9% were neutral, or strongly/moderately disagreed that they need for formal training.
Survey Responses.

aData available from 392 respondents, 10 respondents (2%) declined to respond.
The evaluation of the relationship between demographic characteristics and desire for additional training showed that female clinicians were more likely to desire additional training compared to males (X2 = 5.86, P = .016). APPs were more likely to desire additional training than attending physicians (X2 = 11.63, P = .001). The mean years of experience for those desiring more training was 10.1 years, compared to 12.9 years among those who did not favor more training (F(1400) = 9.43, P = .002).
In multivariable analysis, APPs were almost twice as likely to agree/strongly agree that they needed additional training compared to attending physicians (OR = 1.93, 95% CI [1.13, 3.30], P = .016). For each additional year of training, the odds of agreeing or strongly agreeing with the need for additional training slightly decreased (OR = 0.97, 95% CI [0.95, 0.99], P = .023). There was no statistically significant difference by gender (OR = 0.88, 95% CI [0.56, 1.39], P = .58).
Qualitative Results
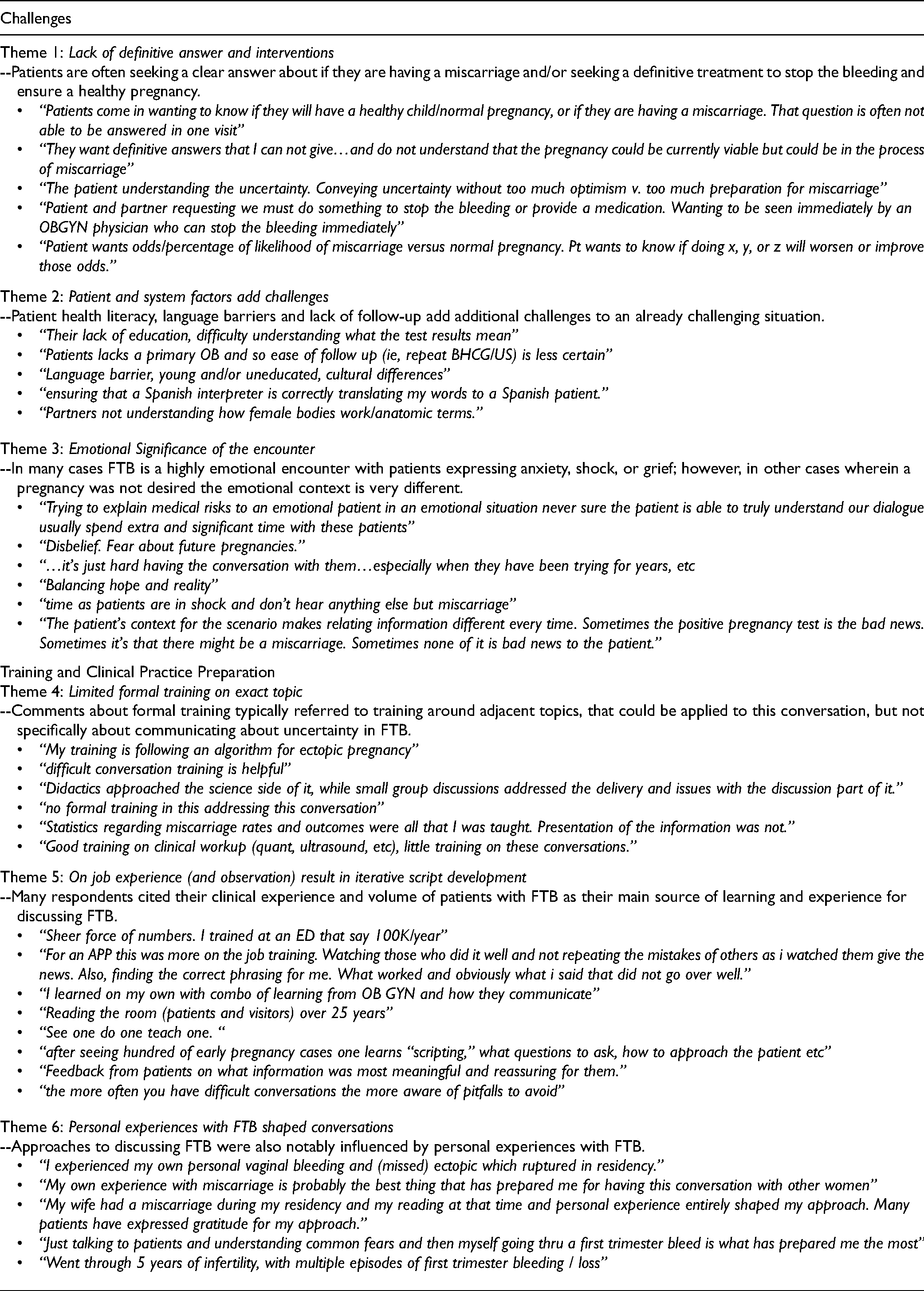
There were 334 free text responses. The initial code book had a total of 19 codes, which ultimately resulted in six themes. Three themes related to the challenges of discussing uncertainty in FTB: (1) Lack of definitive answer and interventions; (2) Patient and system factors add challenges; (3) Emotional significance of the encounter. The remaining three themes related to how training and clinical experience had prepared clinicians for discussing FTB: (4) Limited formal training and simulation; (5) On job experience (and observation) result in iterative script development; (6) Personal experiences with FTB shaped conversations. Table 3 further defines these themes and provides representative quotes.
Emerging Themes from Qualitative Analysis.
Discussion
In this survey of a national sample of ED attending physicians and APPs, most participants reported at least sometimes having challenges communicating with pregnant patients about uncertainty related to FTB. Clinicians indicated that most formal training related to FTB was focused on the diagnostic workup rather than on communicating and interpreting findings. For the communication training that did occur, it was in the form of general communication skills and “breaking bad news” training. Multiple qualitative comments noted that trial and error played a major role in developing clinical approaches. While learning and refinement from experience are necessary, we propose that formal training in this communication skill could improve overall patient experience in this sensitive clinical scenario.
While responses regarding the desire for further formal training on this topic were mixed, almost 40% of respondents agreed that they would benefit from more formal training in this specific area of communication. The significantly higher desire for training among female respondents noted in the univariate analysis does not ultimately appear to reflect differential desire for training based on gender, but rather appears to be driven by APPs in this sample (who have fewer years of clinical experience) desiring more training.
The qualitative themes highlight potential areas for training on the topic that extend beyond the more generalized “difficult conversations” training mentioned by respondents. For example, training could teach the best approaches for explaining the lack of definitive answers and available treatments, as well as an approach for handling the emotional context of the encounter. There is overlap with general uncertainty communication, and existing educational materials related to other, non-obstetric situations could be leveraged and adapted to the FTB scenario. These might include, for instance, the Uncertainty Communication Checklist or simulation-based mastery learning geared towards uncertainty (25,26).
A previous study assessing emergency medicine residents’ experience with general diagnostic uncertainty provides a comparator for this study (24). In that study, 96% of residents encountered challenges at least “sometimes” when discharging patients with uncertain diagnoses, compared with 54% for the study herein. Desire for additional training on general diagnostic uncertainty was 51% for the residents in the prior sample, compared with 39% of study recipients herein. These differences may reflect the more advanced career station and accompanying clinical experience of clinicians in this sample, as well as the more specific scenario being evaluated. While the magnitude of the perceived challenges and desire for training is less than that studied in residents, the challenge and interest in training remain—demonstrating that learning to effectively communicate uncertainty exists at all levels of training to some extent. The disparity in challenges encountered and perceived need for training between these samples suggests that training might be tailored to differing levels of experience with communicating uncertainty. For adept communicators of ambiguity, more nuanced portrayals of uncertainty within a lesson could provide more value.
It is also imperative to consider how training providers to communicate uncertainty improves the patient experience. A recent systematic review of 27 studies on patient experience with early pregnancy complication identified how disparities in provider communication skills can be a detriment to patient experience. It furthermore identified communication and educational gaps for which training could be implemented to improve the patient experience (27). The systematic review described patients frequently expressed a desire to be “treated as an individual person experiencing a significant life event rather than a common condition.” The review also identified potential interventions such as “Understandable information provision about the etiology of pregnancy” and “Staff discussing patients’ distress” that align with the qualitative findings within this study. By constructing a training module around these empirically identified knowledge gaps, we can increase the likelihood that providers are prepared to address these common communicative quandaries in practice.
Interdisciplinary guidelines for care of patients with confirmed EPL (rather than undifferentiated FTB) in the ED have been developed to improve patient care (28,29). These guidelines recommend specific training for ED personnel surrounding assessment of the meaning of the pregnancy, grief counseling, and providing culturally competent and compassionate care. These guidelines do not address early pregnancy complications where there outcome is uncertain. While confirming an EPL can be devastating to the patient, we recommend that providers in the ED also be specifically trained to communicate uncertainty about the status of a pregnancy in response to FTB. To our knowledge, there has not yet been any formal training developed that is specific to this topic.
Our study has several limitations. The study may be subject to self-selection bias since clinicians who were more invested in this topic were more likely to participate. This bias could have skewed our results toward a stronger sense of lacking training and a greater perceived need for training than exists across the population as a whole. The survey was also specifically focused on comfort and training with FTB conversations and did not assess clinician knowledge or patient outcomes related to FTB. In addition, this was a mostly closed-ended survey by design with only a few free-text response boxes, thus limiting our ability to gain a more in-depth understanding of participants’ perspectives. Further, there is an absence of the resident viewpoint, from whom we would anticipate capturing a much higher need for training as they have had limited opportunity to learn through the trial and error of their own experience. Notably, however, almost 40% of independently practicing clinicians, who had practiced for a mean of 12 years, still report a perceived need for more formal training in this specific communication skill. While the survey received over four hundred responses, the 12.1% response rate introduces the risk of response bias, making the results less generalizable to the larger community of emergency clinicians. Finally, the study was deliberately designed to obtain the ED viewpoint; however, in some systems, obstetrics practices and hospital systems have dedicated clinics for urgent OB/GYN complaints that might otherwise go to the ED. Prior studies of FTB reported that the experience of care was different when presenting to an OB/GYN dedicated care environment rather than an ED setting (30,31).
Conclusion
In this study, the majority of ED clinicians identified challenges in communicating with pregnant patients about FTB and had received minimal training on this topic. Many desired more training, with that desire being more pronounced among individuals who were less experienced and APPs. While there has been some attention to communication with patients in the context of miscarriage or EPL (where the outcome is more certain), we suggest that work is needed to incorporate FTB as an area of focus for future training as well as to ensure clear and compassionate communication. Future research can combine existing strategies for general uncertainty communication with patient-identified priorities in FTB to develop a curriculum to guide ED clinicians through these difficult conversations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.