
Abstract
Current pediatric practice guidelines recommend children with complex attention deficit hyperactivity disorder (ADHD) receive a psychological evaluation. However, obtaining such an evaluation in a timely manner can be difficult. The authors present a framework for an economical, efficient, and efficacious approach to diagnosing complex ADHD based on a 5-year project to “fast track” these types of assessments in a tertiary care setting. Patients were triaged to the “fast track” for a streamlined assessment, by a psychologist, within a developmental pediatrics center. Assessment data, diagnoses, and recommendations were recorded for 79 participants. For most of the children, not only was ADHD confirmed, but diagnostic criteria were also met for at least one comorbid condition. For 64% of children the diagnostic picture changed, resulting in an ADHD diagnosis with corresponding changes to treatment planning. Fast track programming cut the wait time for evaluations in half. Preliminary data shows it is possible to clarify diagnoses for this complex population and provide much needed treatment recommendations in a timelier manner through utilization of a “fast track” approach to triage and assessment.
Current estimates indicate that 4% to 12% of all school-aged children may be affected by attention deficit hyperactivity disorder (ADHD), making it one of the most common chronic childhood disorders (1). A national prevalence study, based on data from 2016, found approximately 6.1 million children, ages 2 to 17 (approximately 9.4% of 2-17-year olds) were reported by their parents as ever having been diagnosed with ADHD (2).
Children and teens with ADHD experience significant difficulties in the areas of emotional, academic, social, and familial functioning (3–5). In relation to emotional functioning, they display much higher prevalence of anxiety, relative to the general population, and earlier age of onset of depression (3). In academics, on average, children with ADHD show greater skill deficits and a have a higher likelihood of qualifying for a learning disability (4). In terms of their social functioning, 50% to 70% of children with ADHD experience peer relationship difficulties, resulting in them experiencing higher levels of peer neglect and rejection (5). These difficulties often persist into adulthood and can have a profound negative impact (3). Given the many struggles individuals with ADHD face, it's no surprise that ADHD is considered the costliest chronic health condition for children and adolescents, resulting in an estimated $20.6 billion in health care spending in the United States in 2013.(6) Noteworthy, children with ADHD who do not receive treatment have higher health care expenditures than those who do (6). In contrast, research has repeatedly shown that children who are treated for ADHD, particularly with medication, have a reduced risk for many negative outcomes (7). This data is consistent with past research, indicating the importance of treatment for this population and noting that the first step to treatment is an accurate diagnosis (8).
Pediatric primary care providers are often tasked with evaluating children for a diagnosis of ADHD, with most ADHD diagnoses given by primary care (2, 9). In fact, data from the 2014 National Survey of the Diagnosis and Treatment of Attention-Deficit/Hyperactivity Disorder and Tourette Syndrome revealed that approximately one-half of children with ADHD were first diagnosed by a primary care provider (10). However, primary care ADHD practice guidelines include recommendations for pediatric practitioners to refer patients with complex ADHD (ie, those who present diagnostic challenges due to age or other factors, have failed to respond to treatment, have severe ADHD, or have coexisting disorders or other complicating comorbid conditions) to tertiary care settings for further assessment (11).
ADHD assessments completed in a tertiary care setting are generally rather lengthy in nature and can include multiple appointments. For example, historically at our clinic, the Child Development Center (CDC) at a large Midwest children's hospital, such assessments involved 3 visits on 3 different days. The first visit was a 1 h intake with families, to gather background information on patients. Limited clinical information was gathered before this visit. The second was a 3 to 4 h visit during which the child met individually with the psychologist and was administered a range of normed and standardized measures to assess for ADHD and a variety of comorbid conditions. The final, third visit was a 1 h visit in which parents were provided with results and recommendations based on their child's assessment and child's psychological report. This visit occurred 2 to 3 weeks after the assessment visit.
Unfortunately, long wait lists, a limited population of trained providers/psychologists, and/or the need to travel extended distances to see a tertiary care provider can pose barriers to patients receiving a timely and accurate ADHD diagnosis (11). In Wisconsin this is an issue faced by many patients. Based on data from 2015, 44% of counties did not have a psychiatrist and 39% had 3.5 or fewer psychologists for every 10,000 children (12). Similarly, based on data from 2016 to 2019, in the whole state there were only 4.7 ABP certified developmental-behavioral pediatricians per 10,000 children (13). This resulted in school aged children referred to the CDC at Children's Wisconsin, waiting on average 6 months for an ADHD evaluation.
Given the mismatch between demand and capacity, creating an expedient, efficient assessment process, to better meet the diagnostic needs of children with complex attention related concerns, appeared to be paramount. The purpose of this paper is to describe a 5-year project, known as the Attention Problems and Related Concerns (ARC) screening clinic and its outcomes. The goal of this project was to design and implement a “fast track” for the assessment of complex ADHD. It was hypothesized that this clinic would support timely diagnosis of patients with concerns for complex ADHD, while maintaining patient satisfaction and provision of helpful recommendations for families. Organization of the clinic and data regarding its outcomes are described in this paper.
Method
Project Setting
This project took place from November 2013 to December 2018 at the CDC of Children's Wisconsin. The CDC is a tertiary care pediatric outpatient academic medical setting with a wide referral region. It is a multidisciplinary program consisting of psychologists, speech and language pathologists, developmental pediatricians, and advanced practice nurse practitioners, who participate in diagnostic evaluations and support subsequent treatment. The clinic population includes 60% children who are privately insured and 40% with Medicaid, ranging in age from approximately 3 months to 18 years.
Participants
Children were eligible to participate in the ARC clinic if they were between the ages of 5 and 17 and their primary referral question related to one or more of the following: (1) confirmation of ADHD following unsuccessful treatment and/or to support treatment planning, (2) assessment of ADHD when there were concerns for potential confounding and/or comorbid conditions, (3) confirmation of ADHD when evidence that could be gathered in-clinic by the provider was inconclusive, but suspect for the condition, and (4) assessment of children with severe ADHD whose primary care provider and/or family was looking for more support in treatment planning. Patients were not actively recruited for this clinic. Rather, information related to it was placed on the CDC website and shared with community pediatric providers. This was done as part of the hospital's general communication with the community.
Approximately 209 children and teens participated in the ARC clinic over its 5-year span of operation. Of the 209 children, 79 of them assented and/or parents consented to have de-identified data from their assessment recorded in a Redcap registry. Study protocol approval for collection and analysis of this data was obtained by the Institutional Review Board of Children's Wisconsin.
Procedures
Children were seen through the ARC via 1 of 3 routes. Some were directly referred to the ARC by their primary care provider; some were directly referred by community sources, that is, therapists, school personnel or parents. Others were identified as being appropriate for the clinic when all general service requests referred to the CDC, by either primary care providers or community sources, were reviewed by a triage committee (On a daily basis the CDC receives requests for evaluations that do not specify which provider or program they would like to be seen by. These are referred to as general service requests. These requests are reviewed and triaged by a group of providers on a weekly basis).
For children who were seen through the ARC, a neurobehavioral status examination (CPT Code 96116) was conducted by a licensed psychologist. The exam included a brief history review and approximately 2 h face-to-face examination with patient. Feedback was provided to parents (ie, oral discussion of test results and recommendations and a written summary report) on the same day. Administration of a neurobehavioral status exam allowed the clinician to administer a variety of norm referenced measures. These measures assessed variables found to hold predictive validity in diagnosing ADHD as well as those that screen for differential and comorbid diagnoses. The clinician selected specific measurements for each assessment, based on the child's age and presenting concerns. In-clinic findings from this exam were integrated with the child's history and standardized behavioral data from multiple settings, which allowed for clarification and confirmation of the diagnosis of ADHD and co-morbidities. Parents were later provided with a comprehensive written report outlining diagnostic findings and recommendations.
Measures Used
Areas of functioning assessed included baseline level of cognitive ability using an abbreviated IQ test, as well as, selected aspects of neurocognitive functioning that have been shown in the research literature to hold power in differentiating those with and without ADHD (14–19). Additional measures designed to briefly assess for the presence of common co-morbidities and disorders that may account for a child's attention difficulties, such as learning disorders, depression, and anxiety were also included. All measures were widely employed, standardized, and normed psychological assessments (see Table 1 for a listing of all test measures used in the ARC clinic).
Listing of Constructs Assessed and Associated Measures Utilized by the ARC.

Key to measure abbreviations: a Wechsler Abbreviated Scale of Intelligence 2nd Edition; bStanford-Binet Intelligence Scale-5th Edition; cWide Range Assessment of Memory and Learning-2nd Edition; dStanford-Binet Intelligence Scale-4th Edition; eNEuroPSYchological Assessment-2nd Edition; fKaufman Assessment Battery for Children-2nd Edition; gTrail Making Test from Halstead-Reitan Neuropsychological Test Battery; hThe Stroop Color and Word Test; iGordon Diagnostic System; jContinuous Performance Test-3rd Edition; kContinuous Auditory Test of Attention; lSelective Reminding Tests; mRey Complex Figure Test; nDevelopmental Test of Visual Motor Integration; oWide Range Achievement Test-5th Edition; pChildren's Depression Inventory-2nd Edition; qRevised Manifest Anxiety Scale-2nd Edition; rScreen for Child Anxiety Related Emotional Disorders; sBehavior Rating Inventory of Executive Function.
Other data sources (collected prior to the patient's in-clinic examination) included symptom inventories and broad band standardized behavioral checklists. These measures assessed for attention difficulties across environments and presence of comorbid disorders. A comprehensive history form (an adaptation of Michael Gordon's ADHD Screening Form (20)) was completed by the patient's parents or major caregivers, prior to the patient's exam visit. A brief interview with the patient and the patient's primary caretaker(s) was conducted at the time of the in-clinic evaluation. During this interview the comprehensive history form was reviewed and family relationships, in the context of each child's broader culture and community, were assessed.
Statistical Analyses
Sample characteristics were described using summary statistics appropriate for continuous and categorical data. Statistical analyses were performed using Redcap reports and excel formularies.
Results
Demographics
In its most recent year of operation, 10% to 20% of children referred to the CDC for psychological assessment, were triaged for evaluation through the ARC.
Of the 79 children and teens seen through the ARC clinic, who assented and/or whose parents consented for their data to be stored in the Redcap registry, 59 were boys (74.7%) and 20 were girls (25.3%), with ages ranging from 5 to 14 (mean age 8). Three families declined to report their race and the remaining reported the following racial backgrounds: American Indian-1 (1.3%), African American-6 (7.9%), Asian-4 (5.3%), White-61 (80.3%), and Multiple-4 (5.3%). Approximately 41 (52%) of this data sample of 79 children and teens were referred by pediatric care providers while the remaining 38 (48%) were community referred.
Pre-Existing Diagnoses
From the sample of 79 school aged children in the registry, 21 (27%) had an ADHD diagnosis from another setting and 45 (57%) had no diagnosis (for a complete listing of initial diagnoses, see Table 2).
Frequency of Incoming Primary Diagnoses, Exit Primary Diagnoses, and Comorbidities.

Diagnostic Outcomes
After their evaluation 72 (91%) children met criteria for a diagnosis of ADHD. Only 5 (7%) met diagnostic criteria for a primary diagnosis of adjustment disorder; 1 (1.3%) met diagnostic criteria for a primary anxiety disorder; and 1 (1.3%) met diagnostic criteria for attention/concentration deficit secondary to parent-child problem (see Table 2).
In 57 (79%) of the 72 children who met criteria for a primary diagnosis of ADHD, diagnostic criteria were also met for comorbid conditions. Of these 57 children, 43 (60%) met diagnostic criteria for one comorbidity; whereas, 14 (19%) met criteria for 2 or more comorbidities (see Table 2 for a listing of comorbid diagnoses).
Pre-Existing Treatments
Prior to undergoing their ARC assessment, 8 (10%) children in the sample were participating in psychotherapy and 3 (4%) families reported participating in behavior management training. Twelve (15%) children had Individual Education Plans (IEP)s, 3 of these were under the domain of Other Health Impairment, for previously diagnosed ADHD. The domains for the remaining IEPs were as follows: Specific Learning Disability-2, Speech and Language-6, and Emotional and Behavioral Disability-1. A large number of the sample had a 504 plan in place (58, 73%), due to attention-related concerns in the school setting. Finally, 12 (15%) of the patients were being prescribed medication to treat previously diagnosed ADHD (10 prescribed psychostimulants and 2 prescribed anti-hypertensive medications). Of these 12 patients, 3 were prescribed a combination of stimulants and hypertensive medications and one was also prescribed an anti-depressant.
Treatment Recommendations
In 58 of the 79 (73%) cases recommendations for amendment of a 504 plan were provided and in 14 (18%) recommendations for an IEP were made (either implementation of one or adjustment to an existing one). In 47 (59%) recommendations for individual cognitive behavioral therapy were made, in 58 (73%) recommendations for parent behavioral management training were made, and in 35 (44%) recommendations for participation in social skills training groups were made. Finally, in 70 (89%) recommendations for medication evaluation/re-evaluation were made.
Patient Satisfaction and Scheduling of Assessments
A review of all patients seen through the ARC clinic in 2018 revealed that, on average, these children and teens were seen for their assessment approximately 3 months sooner than those triaged to the CDC's general school aged assessment clinic (3 months vs 6 months). Review of data, collected via NRC's Real Time Survey (a patient feedback collection system utilized by Children's Wisconsin), indicated high satisfaction levels across all parameters (see Figure 1).
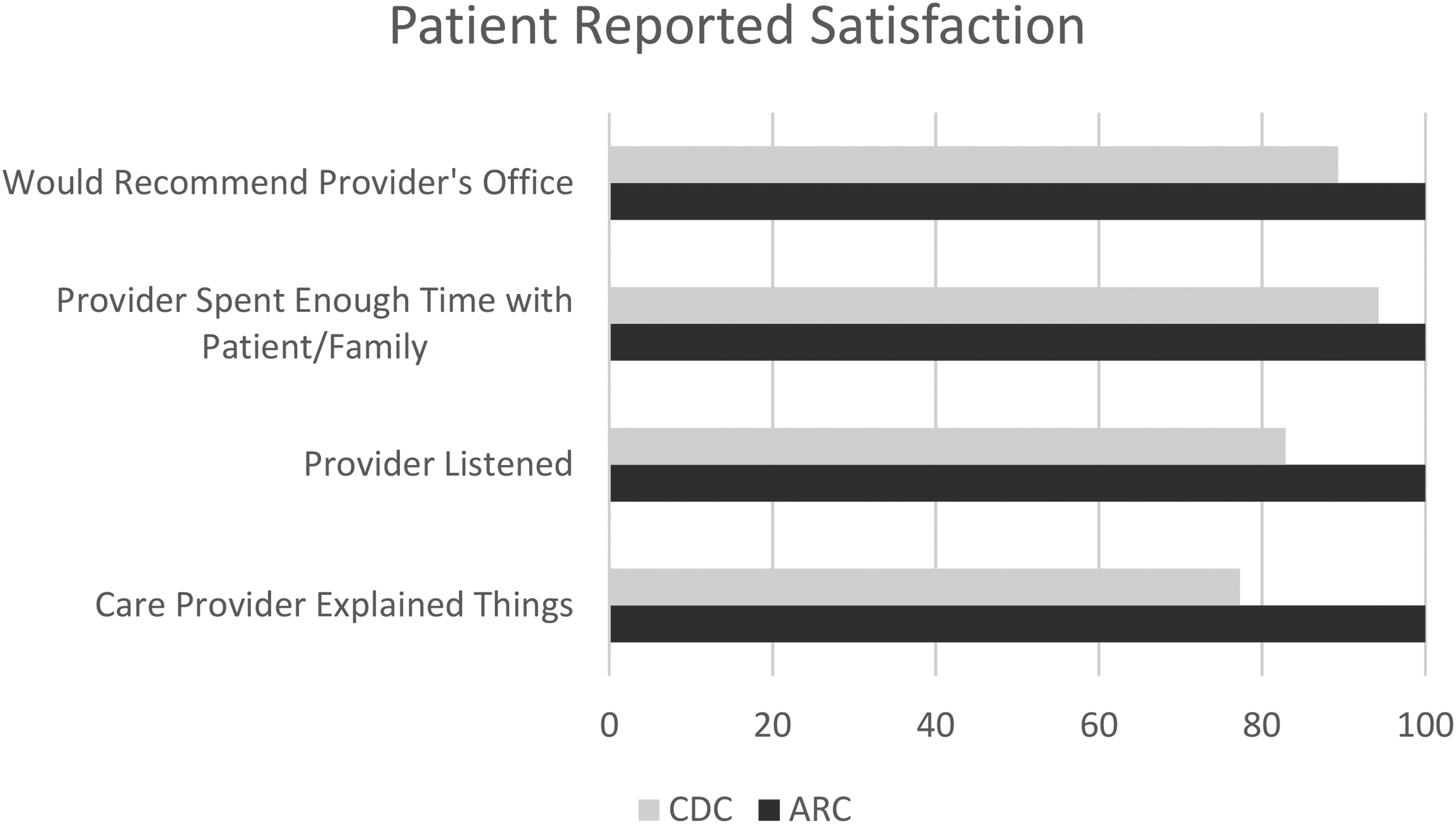
Bar chart: patient reported satisfaction with the ARC in comparison to patient reported satisfaction with all other assessments completed at the CDC.
Financial Reimbursement
In the tertiary care setting, with one pediatric psychologist dedicating approximately 1/4 to 1/3 of her clinical time to providing assessment services through the “fast track” ADHD assessment program, revenues were collected as depicted in Table 3.
Revenues Collected by Service Provided.
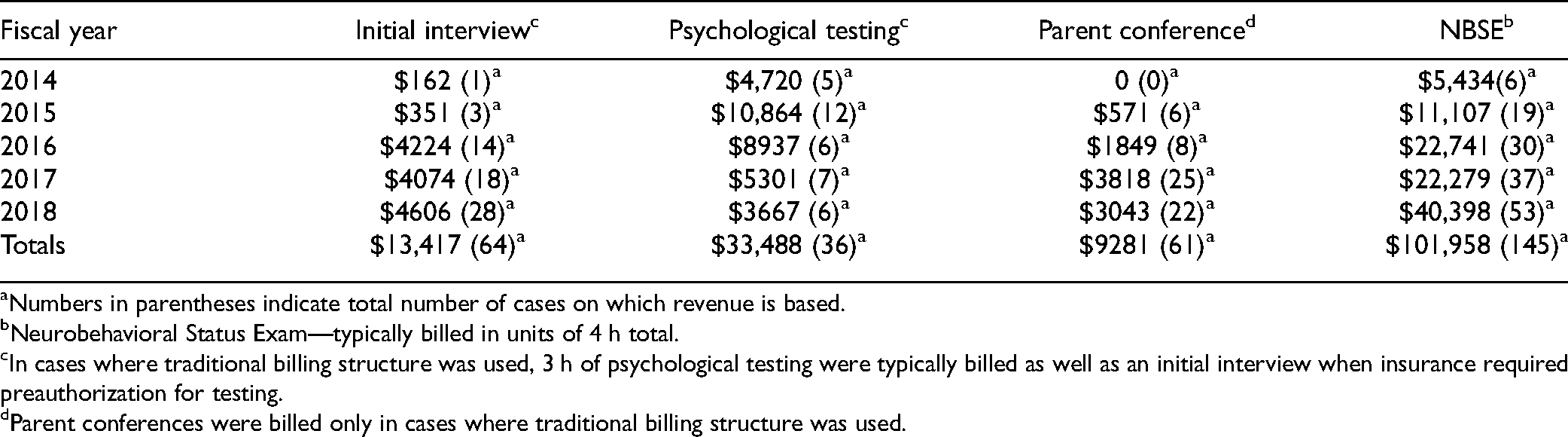
Numbers in parentheses indicate total number of cases on which revenue is based.
Neurobehavioral Status Exam—typically billed in units of 4 h total.
In cases where traditional billing structure was used, 3 h of psychological testing were typically billed as well as an initial interview when insurance required preauthorization for testing.
Parent conferences were billed only in cases where traditional billing structure was used.
Discussion
Results from our project indicate that it is possible to provide families with a “fast track” for the assessment of complex ADHD and receipt of a brief yet comprehensive evaluation can support timely diagnosis and treatment planning for this patient population. The “fast track” was achieved by increasing the amount of information gathered before the clinic visit, use of a slimmed down testing battery informed by research, and provision of feedback to families on the same day as the child’s assessment. Evaluation through the ARC not only led to substantial changes in the number of children diagnosed with ADHD (from 27% to 91%, a change of 64%), but also the number of comorbid diagnoses identified. These findings are consistent with research conducted in other developmental clinic settings, that has found high rates of ADHD and comorbidity, in comparison to community samples (21). They also support the benefit of recommended comprehensive evaluations for this patient population. Such assessments are clearly needed for clarification of the complex diagnostic picture with which many of these patients present.
For most participants in the ARC, receipt of timely diagnostic clarification led to changes in treatment recommendations. As was noted earlier in this article, this is critical as application of best practice treatments can help to reduce negative outcomes for children/teens with ADHD (7). Many participants in our study already had some support in school (most through a 504 Plan), even though they did not have a medical diagnosis of ADHD. After receiving their diagnosis, patients were provided with treatment plans in-line with best practice guidelines, which included recommendations for both medication and parent behavioral management (7, 11). The low number of children who were receiving these services, prior to evaluation, is concerning and further points to the need for access to timely assessment services. Consistent with the large percentage of patients diagnosed with a comorbid adjustment, anxiety, or depressive disorder, many patients were also referred for individual psychotherapy. This is a critical point as without such additional treatments, less than optimal response to treatment for the child's ADHD is likely to be seen (21).
Finally, and importantly, analysis of billing and collections data suggests that assessment efforts alone can generate a good portion of the funding needed to financially support a pediatric psychologist's time in a specialty care setting. This is the case regardless of whether a neurobehavioral status exam (CPT 96116) billing structure is used, or the more traditional diagnostic psychiatric interview (CPT 90791), psychological testing (CPT 96136, 96137, 96130), and interactive feedback with family/caregivers (CPT 96131) billing structure is used. In addition, survey data shows patient families were consistently satisfied with the brief yet comprehensive assessment. Finally, the number of children who went through the clinic over its 5 years would suggest that such assessment services were desired by providers and patient families.
Future Directions and Limitations
While our program took place in a tertiary care setting, this model could easily be accommodated to other settings, such as primary care offices with collaborative care (integrated or co-located models). Directions for future research include determination of pediatric health care settings in which it is most likely to be effective and appropriately utilized, and replication of the current study with a larger sample. Continued refinement of efficient and efficacious assessment batteries, allowing for accurate yet brief assessments could also be explored. Additionally, consideration could be given to evaluation of reduction of patient burden for other providers, in the tertiary care setting. This could include examination of impact on waitlist for general services in the clinic and reduced pressures faced by clinicians (both psychologists and medical providers) within and outside the clinic, as their patients are seen faster and updated treatment plans are received in a timelier manner, etc.
Limitations of the current project include the low number (79) of children and teens who gave assent or whose parents gave consent for storage of their data in the Redcap data registry. This limited number resulted in our data sample representing only a small portion of the children and teens actually assessed through the fast track clinic and likely impacts generalizability of our findings to similar clinics. Likewise, treatment recommendations may vary based on clinical judgement and accessibility of support services, thus affecting generalizability of the findings. Other limitations include the lack of inclusion of follow-up data regarding follow through with recommendations and corresponding change measures on behavior checklists.
Conclusion
Implementation of a fast track assessment model for assessment of complex ADHD in tertiary care settings holds the potential for improving access to care. As noted in the recent AAP Guidelines for ADHD diagnosis and management, ADHD is one of the most common childhood neurobehavioral disorders; however, there are numerous systemic barriers that profoundly impact a family's ability to secure timely and efficient diagnosis and treatment planning (11, 22). In the current medical environment in which prompt, evidenced-based treatment and successful patient outcomes are being incentivized, it makes sense that organizations would consider systemic and programmatic changes to support access to timely diagnosis and treatment recommendations for complex ADHD.
Footnotes
Authors’ Note
Ethics approval to report this case was received from Children's Wisconsin's Institutional Review Board (approval #38425-15). All procedures in this study were conducted in accordance with the Children's Wisconsin Institutional Review Board's (approval #38425-15) approved protocols. Written informed consent was obtained from patients and/or legally authorized representative(s) for anonymized patient information to be published in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.