
Abstract
Highlights
There is limited evidence on the actual utilization of teledentistry among dental patients during COVID-19.
The purpose of this study was to describe the utilization of teledental services during the COVID-19 pandemic among dental care seekers in Saudi Arabia.
To my knowledge, this is the first report showing that teledental services were weakly utilized by dental care seekers during COVID-19 in Saudi Arabia, although Saudi Arabia has a strong technological infrastructure with a highly ranked health care system.
Introduction
Since the novel coronavirus disease (COVID-19) hit Saudi Arabia in March 2020, 1 the Saudi Ministry of Health (MOH) has taken the lead in controlling the spread of COVID-19 with the collaboration of different governmental and nongovernmental bodies. The MOH and the Saudi Center for Disease Prevention and Control (Weqaya) have released many announcements, protocols, and guidelines to limit and control the COVID-19 pandemic.2,3 These guidelines focus on individuals, communities, professionals, and healthcare workers of different specialties. Many healthcare services were requested to postpone and limit their provided services due to the unurgency of some services, such as radiology, dermatology, ophthalmology, and dental services. Dental care is one of the health services that has been severely affected by COVID-19. Shortly after the first COVID-19 cases were confirmed in March 2020, dental clinics were ordered by the MOH to limit their services to only emergency treatments, 4 and they were requested to follow the dental emergency protocol during the pandemic. 5
The MOH planned and then acted to fully reopen different health services for routine healthcare and treatments under specific protocols according to COVID-19 updates and recommendations from Weqaya. In May 2020, dental clinics were allowed to operate 50% of their operational capacities, but they were requested to avoid cash and to designate respiratory triage areas for COVID-19 infection. 6 Guidance for reopening dental services during the pandemic was released by the MOH. 7 The guidance includes the latest evidence-based recommendations to provide safe dental services such as air control, personal protective equipment (PPE), sterilization, and respiratory triage. 7
Dental services are delivered to dental care seekers mainly through face-to-face dental care. However, many dental clinics around the world were forced to limit their face-to-face services to only emergency dental services, especially during the first months of the COVID-19 pandemic.4,8 As a result, teledentistry was viewed as an alternative by many dental services such as consultation, education, screening, triaging, and monitoring.9–11 Teledentistry application during COVID-19, may facilitate stronger dentist–patient relationships, increases patient compliance, is cost-effective and improves access and other benefits.10,12,13
Currently, the majority of health facilities in Saudi Arabia are supplemented with the required technological infrastructure to support different formats of telehealth, such as telemedicine and teledentistry. 14 Previous studies have presented perceptions and readiness of teledentistry utilization among dental practitioners and dental patients.13,15,16 However, there is limited evidence on the actual utilization of teledentistry among dental patients during COVID-19. Thus, the purpose of this study was to describe the utilization of teledentistry services during the COVID-19 pandemic among dental care seekers in Saudi Arabia. In addition, factors influencing teledental utilization were investigated. Finally, patients’ satisfaction levels regarding the dental services they received through teledentistry were measured.
COVID-19 is one of the diseases that occurs after infection by a member of the family of coronaviruses (CoVs), which may cause mild to severe illnesses.17,18 Symptoms range in severity and may include shortness of breath, fatigue, fever, dry cough, vomiting, diarrhea, sore throat, muscle pain, headache, and confusion.19,20 Respiratory droplets and secretion are the primary channels for transferring COVID-19. In addition, airborne transmission is supported by aerosol generation. 17 The majority of dental procedures generate aerosols, which put dental practitioners and patients at high risk of becoming infected at dental care facilities with CoVs, COVID-19 in particular.17,18 The scientific evidence supporting these risks has pushed the Saudi MOH to release regulations, instructions, and guidelines to limit the spread of COVID-19 among dental clinics, mainly by reducing the number of dental practitioners and patients at dental care facilities during COVID-19 and taking full precautions to control the spread of COVID-19.2,7
Dental services are divided into 4 major services: nonurgent, urgent, emergency, and advice services. Emergency dental care is any potentially life-threatening case, such as uncontrolled bleeding, facial swelling, or trauma. Urgent dental care involves managing severe or uncontrolled symptoms that the patient cannot handle, such as lesions and dental abscesses. Nonurgent dental care involves elective and routine dental services, such as implants and check-ups; and finally, advice dental care aims to manage mild or moderate symptoms, such as antimicrobials, which can be delivered remotely. 7 With the spread of COVID-19, the reduction of face-to-face dental care, and the suspension of some dental services, the existing literature has viewed telemedicine as an alternative solution to deliver some dental services.9,11,13,15,21–23
According to the American Dental Association (ADA), teledentistry is “the use of telehealth systems and methodologies in dentistry. Telehealth refers to a broad variety of technologies and tactics to deliver virtual medical, health, and education services”. 24 Different dental services can be utilized through teledentistry, such as teleconsultation, tele-education, telediagnosis, teletriage, telemonitoring, telesurgery, and teleorientation.9,10,25 Teleconsultation is the most common way of utilizing teledentistry during which dental consultations can be delivered by dental specialists through telecommunication. 25 Teletriage can be used for remote assessment of oral health beneficiaries such as schoolchildren to prioritize urgent and emergent cases without the need to attend dental clinics by using smartphones. 10 Teleorientation and telediagnosis are similar to the way dental practitioners generally screen, diagnose, guide, and refer patients, for example, by exchanging images and photographic control.9,10 Additionally, telemonitoring is a way of following up, continuously evaluating, and managing the progress of specific treatments that require frequent visits, but remotely through phone calls or video sessions. 10 Finally, telesurgery is a service where oral surgeons in rural areas can monitor, direct, and perform oral surgeries in urban areas with the assistance of dental specialists using video and audio telecommunication. 25 In addition, dental practitioners can benefit from tele-education to improve their skills via virtual learning, online learning applications, and videoconferences.23,26
The fundamental element necessary for successful teledentistry services is effective distance communication, which can occur through; first, messaging applications, such as WhatsApp, Instagram, Facebook, SMS, Telegram, and Twitter. Second, video calling applications can be used, such as Teams, Instagram, WhatsApp, Skype, and Zoom. Third, systems and programs have been developed to support telehealth, such as MeMoSA and CellScope.10,26 Currently, the telecommunication industry is witnessing rapid development, and the majority of people are using some sort of telecommunication in their daily lives. In fact, people were forced to use telecommunications during the COVID-19 pandemic to maintain their social interactions as traveling and gathering restrictions were applied.
In Saudi Arabia, teledentistry infrastructures regarding technology, fast internet, and telecommunications options are strong and promising. In addition, practicing dentistry is restricted to only licensed dentists from the Saudi Commission for Health Specialties (SCFHS) to ensure that dentists who practice dentistry in Saudi Arabia are competent and use the best standards and practices. 27 In general, Saudi dentists perceive teledentistry positively, and they believe teledentistry can improve the efficiency and cost-effectiveness of dental care. 16 However, the implementation of teledentistry has not been ideal in Saudi society. 13
During the first few months of the COVID-19 pandemic, many face-to-face dental services were suspended and restricted to only emergency dental treatments. 4 As a result, teledentistry was focally reviewed as a potential alternative for dental care seekers and providers.9–11 Internationally, the majority of dental patients who received dental services during the COVID-19 pandemic via teledentistry have given positive feedback regarding patient satisfaction, ease of use, effectiveness, reliability, and usefulness. 15 This study assessed the utilization of teledentistry services during the COVID-19 pandemic among dental care seekers in Saudi Arabia. In addition, factors associated with teledentistry utilization and patients’ satisfaction levels regarding the dental services they received through teledentistry are described.
Methods
The study was a cross-sectional descriptive study. An online self-administered survey was released publicly and distributed through different social media channels and email invitations. The survey was available during March, April, and May 2021. The targeted respondents were convenience dental care seekers who used any teledentistry services during the COVID-19 pandemic in Saudi Arabia.
The questionnaire was developed in reference to the measuring criteria of teledentistry patient utilization that were stemmed from a study that was conducted by Rahman et al. 15 In addition, questions regarding factors affecting the patient utilization of teledentistry were stemmed from a survey developed by Alsharif and Al-harbi. 16 Participating in the online survey was voluntary, and respondents were given the option of participating in Arabic or English. The questionnaire was available in Arabic and English. The questionnaire was comprised of demographic data, teledentistry-utilized services, factors influencing teledental utilization, and patient satisfaction.
Demographic characteristics included gender and age variables as they were the most reported demographic characteristics in previous studies in the scope of teledental services.15, 16 In addition, self-evaluation of oral health status was a question delivered to participants as it gives a general baseline of oral health measurements. Participants were given 4 classifications to choose from as their self-evaluations of their oral health status: excellent, good, fair, and poor. Furthermore, descriptions of teledentistry and oral health were included in the questionnaire. These descriptions were extracted from the ADA and may help participants fill out the questionnaire accordingly.24,28
The developed questionnaire was scientifically validated. The whole questionnaire was based on the literature review of different articles that were done on similar or related topics. Additionally, the questionnaire was pilot tested among 3 adult individuals to validate the Arabic and English versions for any ambiguity or other concerns.
The responses were recorded, validated, and analyzed using an Excel spreadsheet (Microsoft 365). Descriptive statistics were used to summarize the observations, and the data were expressed as percentages. Comparative analysis was used to measure the association between the utilization of teledental services and different variables. Odds ratios (ORs) were used to determine whether gender, age, and oral health status had an impact on the utilization of teledental services during COVID-19. In addition, chi-square tests (
Results
A total of 242 responses were collected; however, 7 responses were excluded from the analysis because the respondents have not lived in Saudi Arabia continuously from the time the COVID-19 pandemic arrived in March 2020 until the data were collected. As a result, there were 235 responses available for analysis.
Among the 235 responses, 216 (91.91%) did not use any teledental services during COVID-19, while 19 (8.09%) utilized different teledental services during COVID-19. Most responses came from men (54.04%), aged between 25 and 44 (62.98%). Participants who self-evaluated their oral health status as good were 45.96% of all participants (Table 1).
Descriptive Statistics of Teledental Utilization Regarding Gender, Age, and Oral Health status; N (%).

Percentage of column total.
Of the 216 responses from participants who did not utilize teledental services during COVID-19, the majority were men aged 25 to 44 years old, and they described their oral health status as good. On the other hand, different characteristics were observed for the 19 responses of those who utilized teledental services during COVID-19. Approximately two-thirds of dental patients who utilized teledental services were men aged 25 to 44 years old (52.63%) or aged 45 to 64 years old (47.37%), and there were null responses from other age groups. Furthermore, patients who utilized teledental services self-evaluated their oral health status as good and fair for almost 32%, while the majority reported excellent oral health status (Table 1).
Participants who utilized teledental services during COVID-19 used the following services: dental diagnosis, dental consultations, monitoring and follow-ups of previous dental treatments, routine dental check-ups, and finally, triaging dental cases as emergency or nonemergency cases. Figure 1 shows the percentages of utilized teledental services during COVID-19.
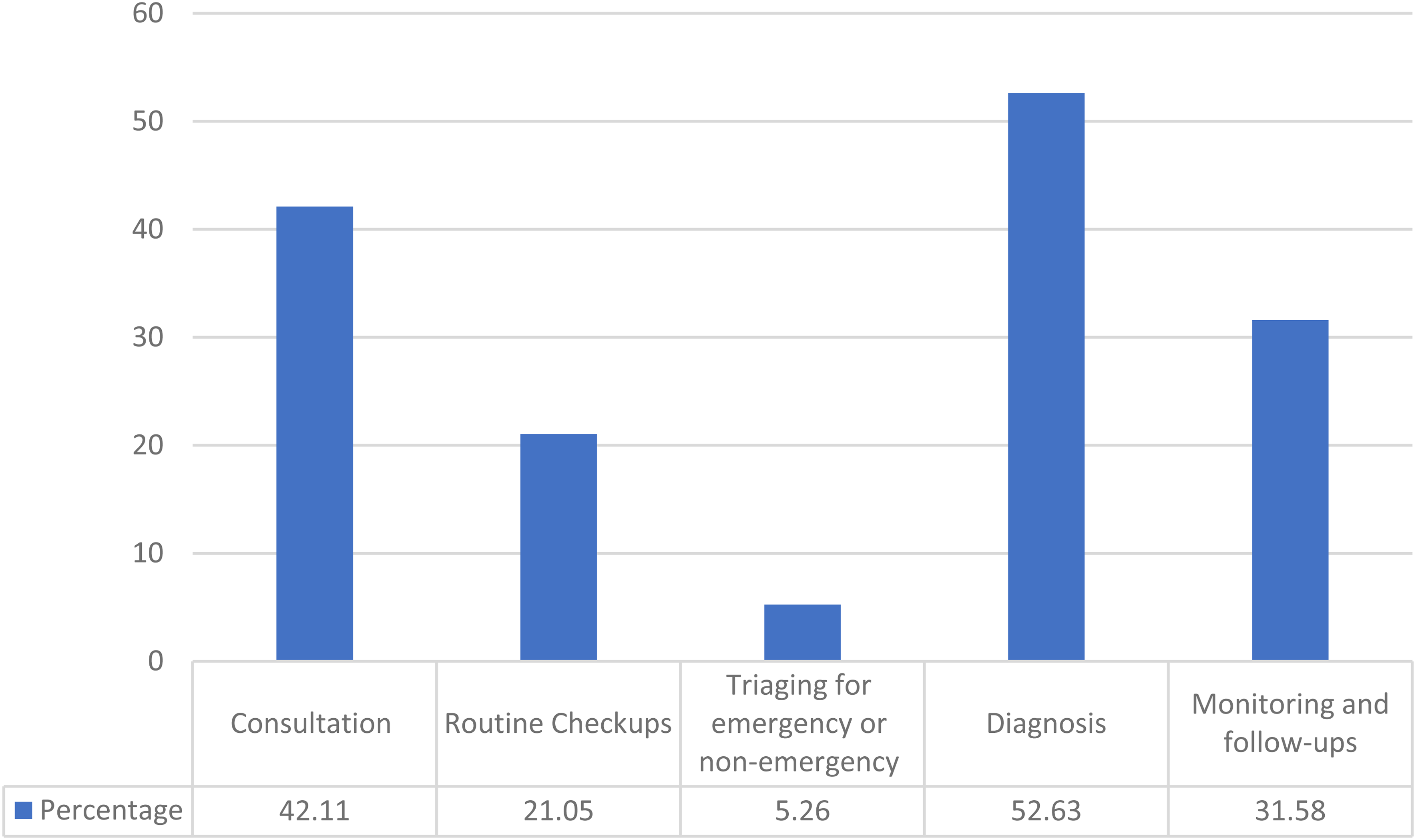
Utilized teledental services during COVID-19; N = 19.
The 19 respondents who utilized teledental services were asked about the factors that influenced their selection of different dental service delivery methods. Respondents evaluated the following as the most influential factors for utilizing in-site physical dental services: time savings, effective communication with dentists, effective explanation of dental problems, and matching their dental and oral needs. In addition, service accessibility, absence of connection issues, and ease of use were the most influential factors for phone dental services use. However, virtual dental services did not score the highest among the different dental service delivery methods (Table 2).
The Utilization of Different Dental Services Delivery Methods, N (%).

Percentage of row total.
Patients’ satisfaction with teledental delivery services was measured through the willingness of patients to reutilize teledental services in the future. Generally, of those who utilized teledental services, and in comparison, of virtual versus phone dental services, patients were more satisfied with phone dental services (57.14%) than with virtual dental services (42.76%) (Figure 2). Association tests of patients’ satisfaction levels regarding the dental services they received through teledentistry were measured, but they were not significant at a p-value < .05.

Patients' satisfaction of teledental delivery services (N = 19): phones vs. virtual.
Regarding the support of technology and applications for teledental utilization, participants used smartphones (84.21%), social media (58.89%), dental clinic websites (47.37%), dental applications (31.58%), and laptops or computers (21.05%). Figure 3 shows the technological use for seeking teledental services. Most respondents did not need laptops or computers, but they did need smartphones to utilize teledental services.
Furthermore, the respondents mostly preferred to utilize future phone dental services if they were looking for general dental services, dental consultations, or dental education. They mostly preferred to utilize future on-site physical dental services if they were seeking a dental diagnosis, dental monitoring, or dental triaging services. On the other hand, virtual dental services were not among the highest-scoring for preferable dental services (Table 2).
Discussion
This study applied descriptive statistics to the utilization of teledental services during COVID-19 as self-reported by the study's participants. COVID-19 has influenced individuals’ behaviors towards the utilization of health/medial services. Dental care is one of the fields with services that have been affected by the pandemic internationally.15,20 The literature recommended utilizing different dental services through teledentistry during COVID-19, such as dental consultations, dental diagnosis, dental triaging, and other dental services.10,15,20,21
In this study, more than 91% of respondents did not use teledental services during COVID-19. Reasons for not utilizing teledental services may include reasons related to the technical necessity of telehealth services. 5 In addition, oral health status affects the use of dental services in general. Despite factors that may affect oral health status, unhealthy oral health status may be related to the underutilization of dental services.29,30 Also, urgent dental services were the most requested dental services during the pandemic, which required face-to-face dental care. 31
On the other hand, most dental patients who received services through teledental services were men, from middle-aged groups, and had excellent oral health status. The teledental services that were used the most during COVID-19 were dental diagnosis, oral health consultations, monitoring and follow-ups, dental check-ups, and triaging for emergency and nonemergency dental care. These findings are consistent with previous recommendations regarding recommended services for teledentistry. 21
Regarding the factors that influenced patients to utilize dental services through different delivery methods, the observations were supported by dentists’ perceptions of teledentistry in Saudi Arabia. 16 The factors that influenced the use of teledental services were service accessibility, the absence of connection issues, and ease of use. Additionally, respondents showed a willingness to utilize teledental education in the future. The insignificant association of different study variables with patients’ satisfaction levels of teledental delivery services was expected due to the small sample of participants who used teledental services during the pandemic.

Patients' use of different technologies to seek teledental services (N = 19).
The availability of technology support, such as smartphones, social media, dental clinic websites, and dental applications, was another aspect that respondents viewed as an important element to in enhancing teledental services. The literature has examined the important role of technologies and applications for teledental services.11,16
There are several limitations to this study. First, the small sample of respondents who utilized teledental services may affect the significance of some statistics and tests that were performed. Second, the convenience of online sampling may also have affected the accuracy of some observations and resulted in nonrepresentative samples. Finally, recall bias might have occurred as a result of self-reported answers. Despite these limitations, the study is unique in its goal and purpose. Few studies have been performed on the utilization of teledental services during COVID-19 among dental care seekers, especially in Saudi Arabia. This research has explored the percentages of different aspects of teledental service utilization as reported by teledental care seekers.
Conclusions
Saudi Arabia has a strong technological infrastructure with a highly ranked healthcare system. However, teledental services were weakly utilized by dental care seekers during COVID-19 in Saudi Arabia. Awareness, education, and promotion efforts are necessary to enhance and support the importance of using teledental services among the Saudi community.
Footnotes
Acknowledgements
I would like to thank the Deputyship for Research & Innovation, Ministry of Education in Saudi Arabia for funding this research work through project number 7866.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deputyship for Research & Innovation, Ministry of Education in Saudi Arabia (grant no. 7866).