
Abstract
Introduction
During the ‘Circuit Breaker’ period of the COVID-19 pandemic in Singapore from April to June 2020, governmental policies restricted the practice of dentistry nationwide to the provision of emergency treatment only, regardless of the patient’s COVID status. As such, teledentistry was used as an alternative means to continue providing some form of dental care to COVID-19–positive patients who were admitted to a COVID-19 Community Care Facility.
Description
The patients were physically triaged by physicians who would send clinical photos to the author via a messaging application, who would in turn triage the patients and assess if they required referral for emergency dental treatment. For patients who did not meet the criteria for referral, the author would advise the physicians on the subsequent management plan which included, but was not limited to, the provision of symptomatic relief.
Conclusions
This article shows the feasibility of undertaking teledental consultations using clinical photos transmitted via a messaging application. The practical implication is a reduced barrier for patients and healthcare professionals to access teledentistry, without having to resort to sophisticated equipment. Hopefully, this will translate into the continued provision of some form of dental care to patients during the ongoing pandemic as opposed to no care at all.
Introduction
At the point of writing (10 Jun 2021), Singapore experienced more than 62,200 cases of COVID-19 and fortunately only 34 fatalities. 1 During the ‘Circuit Breaker’ period from April to June 2020, where various measures were imposed to reduce the rate of community transmission, a total of four purpose-built Community Care Facilities (CCFs) were built outside of hospitals to care for COVID-19 patients who were clinically stable with mild or no symptoms, had no significant co-morbidities and with lower risk factors. The patients in these CCFs were monitored closely by physicians and nurses/paramedics in case they needed to be transferred to hospitals for specialist management, and most of these patients recovered and were discharged from the CCFs with minimal intervention after serving the minimum 21 days isolation. The purpose of these CCFs was to preserve the capacity of public hospitals to focus on patients who required emergency and intensive care.2,3
To minimise COVID-19 transmission risks, the Ministry of Health Singapore had placed nationwide restrictions on the practice of dentistry during the COVID-19 pandemic, regardless of the patient’s COVID status. For example, during the ‘Circuit Breaker’ (7 Apr to 1 June 2020) and earlier phases of ‘Safe Reopening’ (2 June 2020 onwards), dental services were limited to the provision of emergency services only, and all other forms of dental procedures, especially aerosol-generating procedures, were deferred until later phases of ‘Safe Reopening’. In addition, COVID-19–positive dental patients could only be managed at the two national dental centres (National Dental Center Singapore and National University Hospital Center for Oral Health Singapore) that were equipped with additional facilities, such as negative pressure treatment rooms, which were necessitated by the pandemic.
These restrictions meant that dental treatment could not be provided on-site at these CCFs. Hence, the dental patients warded at the CCFs were triaged to determine whether they met the Ministry of Health’s eligibility criteria for referral to the national dental centres for emergency treatment, or not. The criteria were: (i) dental extractions for the management of dental abscess with potential obstruction of airway, and/or (ii) pain relief in cases of severe dental pain where the prescribed analgesics provided no or limited relief. Patients who did not meet these referral criteria were provided symptomatic relief for their dental conditions until such time that they were discharged from the CCFs and could seek definitive treatment when the (nationwide) restrictions were lifted.
This article is based on the author’s experiences with teledentistry when he was the sole dentist deployed as part of the Singapore Armed Forces (SAF) medical team over a 5-week period from June to July 2020 to the CCF at the Singapore Expo Convention and Exhibition Center (CCF@Expo for short) 4,5 where a total of 10 exhibition halls were converted to care for COVID-19 patients. This was the largest CCF by bed capacity, and the bed capacity was almost double that of the next largest CCF. The author had served as the dental consultant on-call to patients across a total of six halls (two halls operated by the SAF and another four halls operated by Woodlands Health Campus), with a total bed capacity of around 4,700 beds. The overall incidence of report sick encounters for dental conditions at the six halls was estimated at 2%. 6
Description of the Teledentistry Consultations
Using a general-purpose messaging application that allows users to send text messages and share media such as images or short video clips, the physicians (who were physically running the clinics) would contact the author with the patients’ complaints, take extra-oral and intra-oral clinical photographs with their smartphone and relay them to the author. This was followed by either a text or voice conversation where the author would provide a series of instructions to guide the physician in obtaining the clinical history, examine the patient and where necessary, request for more clinical photographs.
After the author had arrived at a provisional diagnosis for the case, he would then advise the physician as to whether the patient had met the referral criteria for emergency dental treatment or not. In situations where the patients required referral to the national dental centres for treatment, the author would also advise the physicians on what to include in the referral letter, as well as the clinical administrative processes for making the dental referral.
For the teleconsulted dental patients who did not meet the referral criteria, the author would advise the attending physicians on the medications to prescribe (such as analgesics, antibiotics and/or mouth rinse) to provide symptomatic relief and the subsequent management plan. The subsequent management plan included, for example, (i) whether a review was necessary during the remainder of the patient’s stay at the CCF, (ii) the frequency of the review, (iii) what the subsequent attending physician was to look out for at the review, and (iv) what to include in the memo for the patient to seek definitive treatment after he had recovered from COVID-19 and was discharged from the CCF@Expo.
The author was teleconsulted for a total 16 patients. Of these 16 patients, pulpitis (acute toothache due to dental decay) (n = 5) and periodontitis (gum infections resulting in bleeding gums or mobile teeth) (n = 5) were the most common presenting complaints, followed by pericoronitis (infection of gums associated with impacted wisdom tooth) (n = 3). Two of the 16 teleconsulted patients were eventually referred for emergency dental extractions. Of the 16 teledental patients, the author subsequently physically reviewed seven of them because: (i) In some of these cases, the referring physicians struggled to find the right description for the patient’s presenting dental complaints, signs, and symptoms thoroughly, presumably because doctors have no or minimal training in examining dental hard tissues during medical school (and even residency training) and are hardly exposed to, let alone pick up, the vocabulary needed to describe dental conditions. Prior experience, confidence, willingness, and/or risk appetite of the individual attending physicians, as perceived by the author, made up the rest of the considerations that signalled a need for physical review; and (ii) to follow-up and ensure that the dental patients were properly cared for during the remainder of their admission at the CCF. These patients included clinically complex cases (such as the case discussed below) where a physical examination could provide additional information, including tactile sensation, that could not be visually transmitted during the teleconsultation, and offered the opportunity to validate the provisional diagnosis reached during the teleconsultation.
Case Report of a Teledental Consultation
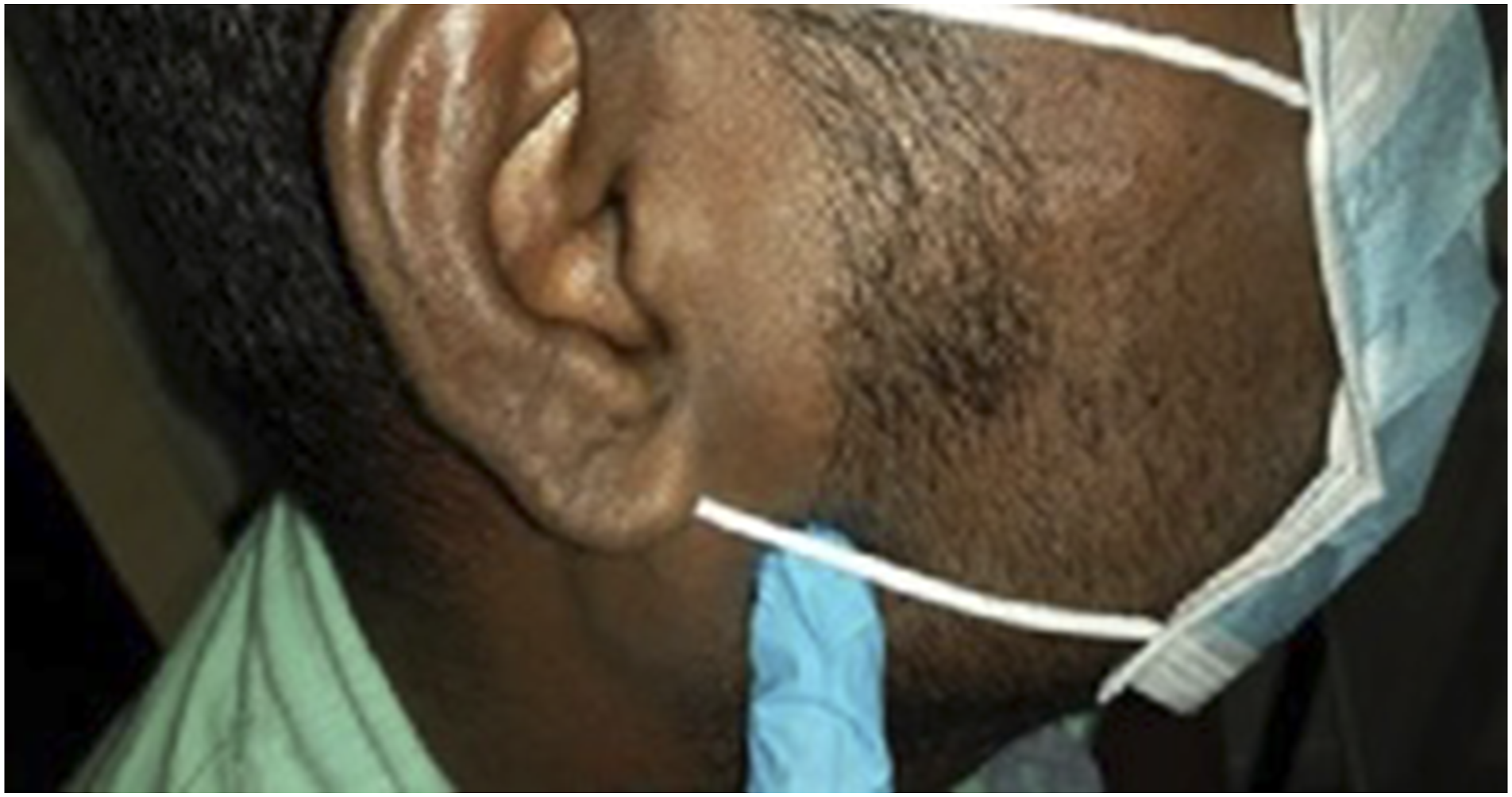
A 39-year-old Indian male patient was referred for ‘right jaw pain x 2/7. Electricity shooting pain localised to angle of the jaw. Wakes patient up from his sleep. Pain worse on chewing and moving his jaw. No blurring of vision. Nil obvious dental caries, gums not inflamed. No pain along salivary gland. Impression: query pulpitis vs TMJ pain.’ What follows is an almost verbatim reproduction of the text dialogue between the author and referring physician as the author guided the physician in conducting a detailed physical examination. Do note that the photographs in this article are unedited and reproduced as they were sent from the referring physicians to the author. Approval has been granted by (i) Woodlands Health Cluster (National Healthcare Group) to publish the patient data contained herein, and (ii) the Singapore Armed Forces to publish this article. Referring physician: “No pain elicited when I press around the gums, and the teeth on all surfaces.” Author: “Intra-oral photos look ok (referring to Figures 1 and 2 Intra-oral photograph showing the maxillary (upper) teeth of a patient referred for right jaw pain. Intra-oral photograph showing the mandibular (lower) teeth of a patient referred for right jaw pain. Physician: “Point tenderness at this point (see Figure 3 Point tenderness upon palpation at this exact extra-oral location. Author: “Are you able to take an intra-oral photo that roughly corresponds to the same spot? I know it can be difficult, try to retract the cheek as much as you can when you take the photo.” Physician: “It’s at the tip of my finger, the area just beyond my finger.” See Figure 4 Intra-oral location of pain that corresponds to Figure 3. Author: “Can you also examine his temporo-mandibular joint (TMJ) and external auditory meatus? For TMJ, palpate around the joint and ask him to open wide and close. See if any action elicits the same pain.” Physician: “External auditory meatus normal. When he opens his mouth, there is pain at that exact area shown earlier outside (referring to Figure 3).” Author: “Can you palpate the ascending ramus intra-orally?” Physician: “Ascending ramus is tender. Pain exactly here on palpation at the ascending ramus.” Referring to Figure 4 again. Author: “Can you palpate around the cheek by placing your index finger intra-orally, and thumb positioned extra-orally?” Physician: “No pain elicited this way.” Author: “Did he eat/bite/chew on anything hard in the past 2 days? Ask if he is aware whether he has any bruxism/nocturnal jaw clenching? When he wakes up, does he get any aches or pains around the jaw, particularly in the same area that you’ve palpated?” Physician: “No to all the above questions”


As a result of the thorough physical examination conducted by the referring physician, in response to the author’s guidance given via teledental consultation, the author was able to arrive at a provisional diagnosis of temporo-mandibular disorder (TMD). The author then directed the physician to prescribe a 5-day dosage of ibuprofen (which was the strongest analgesic available at the CCF@Expo’s pharmacy), as well as to arrange a physical review by the author 3 days later. At the physical review, the author noted that the patient’s pain experience had improved after taking analgesics. At the review, having repeated the examination, the case was definitively diagnosed as TMD associated with the right angle of mandible (masseteric muscle). The patient was then prescribed another week of ibuprofen and directed to return if his symptoms worsen. The patient did not return to report sick for the same condition and was eventually discharged from the CCF@Expo after recovering from COVID-19.
Discussion
Access to Teledentistry During the COVID-19 Pandemic
During the COVID-19 pandemic, teledentistry has been advocated by some healthcare organisations, such as the US Centers for Disease Control and Prevention, 7 as a means to triage dental patients and determine whether the patient needs to be physically seen at a dental clinic or not. The intention of these policy statements is aimed at reducing the overall burden on the healthcare system during the pandemic, as well as to minimise the COVID-19 transmission risks to both healthcare workers and patients. 8 Unfortunately, even before the COVID-19 pandemic, the reported uptake of telehealth by the dental profession lagged behind the medical profession,9,10 where telehealth has been increasingly used in routine care but not so in dentistry. As such, a sudden pivot to teledentistry meant that the gaps in equipment and catch-up in know-how was a significant challenge.
This article shows that teledentistry need not necessarily involve sophisticated technology nor telehealth-dedicated equipment per se and that it is feasible to undertake teledental consultations using clinical photos taken by smartphones which are then transmitted via a general-purpose messaging application. The practical implication is that there is a reduced barrier for patients, non-dental and even dental healthcare professionals, to access teledentistry and that this will hopefully translate into the continued provision of some form of dental care to patients during the COVID-19 pandemic, especially in areas with movement restrictions and/or have policy restrictions on the provision of certain types of dental treatment. In this situation, the proposition is that some care is better than no care at all, even if it is just to provide temporary symptomatic relief. The adoption of teledentistry may also translate into an avenue for affected dental professionals to continue making a living during the pandemic.
Potential Applications of Teledentistry
This article also shows that there is another utility of teledentistry beyond serving as a means to screen whether dental patients need to be seen physically at a dental clinic or not. The author’s experience has shown that dentists can also use teledentistry to remotely guide physicians on how to manage patients who have any dental complaints.
This additional utility of teledentistry can be beneficial in situations where the patient is unable to access a dentist immediately and the physician or nurse is the next best person available to address the patient’s dental conditions. Such situations include, for example, the neighbourhood medical general practitioner setting to more austere environments such as in expedition and wilderness medicine, offshore medicine on-board ships and oil rigs, or even during military deployments.
A potential use case for teledental consultations could be where expedition medics and doctors need (i) to determine whether the patient needs to be evacuated to a dental clinic urgently, and (ii) guidance from a teleconsulted dentist to perform simple emergency dental ‘stop-gap’ treatment (such as placing temporary fillings on decayed teeth), 11 even if they have already had some training but are not so familiar and experienced with performing these procedures. The purpose is to address the patient’s dental complaint to the extent that the patient can continue with the expedition or mission and then obtain definitive dental treatment later. In this situation, teledentistry also serves as a means for the dentist to perform the initial stages of history taking before the patient is referred for definitive management.
Current Limitations of Teledentistry
Teledentistry can be beneficial, pandemic or no pandemic, but more work needs to be done to address certain issues before it can be more widely adopted by the dental profession. Without addressing these issues, the approach of teledentisty will likely be limited as a screening tool in situations where there are barriers to accessing a brick-and-mortar dental clinic. The discussion will focus on three limitations that were specific to the author’s experiences because it is beyond the scope of this article to cover all the limitations of teledentistry.
Data Security
Measures that were taken to minimise the potential data security risks surrounding the mode of teledentistry described in the article included, but were not limited to: (i) only capturing and transmitting images that were necessary for clinical purposes, (ii) the avoidance of capturing images where the identity of the patients could be discernible or at least altering the images to minimise this risk, and (iii) deleting the images and messages once their intended clinical purposes had been achieved. If the appropriate measures were followed to minimise the data security risks surrounding this mode of teledentistry, then in the author’s opinion, the data security risks do not appear to be inevitably higher than any other telehealth operation. This is because data security risks will arise whenever there is some form of digitalisation of patient records including electronic healthcare records of brick-and-mortar clinics who do in-person consultations. As such, the development of appropriate security features and user security protocols would be the way forward, rather than to shun teledentistry altogether.
Further, in the context of the current pandemic where the only available options maybe some care versus no care, data security risks are only one of and, not a trump factor, in decision making. Teledentistry overcomes some of the barriers to accessing dental care and so benefits individuals (e.g. patients with special needs and geriatric patients) and communities (e.g. the less socioeconomically well-off). Indeed, teledentistry has been reported to contribute to the reduction of inequalities in the availability of dental services in rural and/or underserved areas.10,12
Standard of Care
In a teleconsultation, the dentist is wholly dependent on the description of the patient’s condition and clinical photographs provided to arrive at an accurate diagnosis because an incomplete clinical picture will skew the telediagnostic impression and potentially result in under- or over-diagnosis. To illustrate this point, another COVID-19–positive patient at the CCF@Expo was referred for ‘right cheek pain and right premolar pain since yesterday. No fever. Some bleeding when brushing. I think it is probably gingivitis with early signs of turning into a gum abscess…’ See Figures 5 and 6. Extra-oral photo of a patient referred for ‘gingivitis with early signs of turning into gum abscess’. Intra-oral photo of a patient referred for ‘gingivitis with early signs of turning into gum abscess’.

It was fortuitous that an extra-oral photograph (Figure 5) was taken and transmitted during the teleconsultation because there was an obvious facial swelling on the patient’s right side which was not visible on the intra-oral photograph (Figure 6). The telediagnostic impression would be incomplete had the referring physician only sent the intra-oral photograph and the author relied on the physician’s description of the patient’s condition, which did not mention the presence of the extra-oral facial swelling.
In order to enhance the standard of teledental care, the dental profession should consider developing a standard operating protocol to standardise the approach to teledentistry to minimise the risks of missing out signs and symptoms, and therefore bring the standard of care closer to an in-person physical examination. For instance, such a clinical protocol will require the patient or referring physician to provide as complete a clinical picture as possible by including extra-oral photographs (as required) and a thorough description of the patient’s complaint and condition. Since doctors have no or minimal training in examining dental hard tissues, it is worthwhile for physicians and dentists exploring partnerships in providing teledentistry to consider training in the common intra-oral signs for the referring physician to look out for and commonly used dental nomenclature.
Medical–Legal Liabilities
Finally, the teledental provider will need to consider medical–legal liabilities if something goes awry. At present, healthcare workers providing telehealth services in Singapore are expected to provide the same level of quality and standard of care as that of those who provide in-person care. 13 Therefore, in a two-way teledental encounter between the patient and the dentist, the duty of care and liability squarely falls on the dentist. 14 Moreover, the legal situation becomes complex if both parties are physically present in different jurisdictions. In this situation, should the laws of the patient’s jurisdiction and/or dentist’s jurisdiction apply? In fact, there are differing schools of thought with respect to what should be the correct answer to this question. 14
In telehealth encounters, where there are intermediaries between the patient and dentist (as described in this article), it has been stated that the liability should attach to both the dentist and the healthcare provider at the patient’s physical location. 14 This again highlights the need for some form of training in teledentistry if physicians and dentists were to partner in providing teledentistry. Who bears the liability in a situation where the referring physician does not follow the teleconsulted dentist’s advice and there is a negative outcome? How about in an austere setting involving an expedition medic or nurse as the intermediary between patient and dentist; will the principle of necessary intervention and/or the Good Samaritan constitute sufficient defence for the intermediary with respect to medical–legal liabilities?
The segment on medical–legal liabilities raises more questions than answers, and this is partly because the regulatory landscape and modalities to provide telehealth services are still rapidly evolving. For instance, at present, there is no overarching legislation that governs the provision of telehealth in Singapore (until the establishment of the new Healthcare Services Act 15 in early 2023), and the field is currently only regulated by guidelines (such as the National Telemedicine Guidelines) 13 and standards (such as the Position Statement on Teledentistry 16 by Dental Protection, a dental-legal insurer).
Conclusion
This article shows the feasibility of using clinical photos taken by smartphones which are synchronously transmitted via a general-purpose messaging application for teledentistry. This means there is greater accessibility to teledentistry for patients and healthcare professionals without having to resort to sophisticated equipment, which can then serve as an alternative means to continue providing some form of dental care to patients during this COVID-19 pandemic, as opposed to no care at all. This article also shows the potential applications of teledentistry as (i) a screening tool to triage patients who require referral for emergency dental care, and (ii) a means for dentists to guide physicians on how to provide symptomatic care for patients that present with dental conditions. The current limitations of teledentistry with respect to data security, clinical standard of care, and medical–legal liabilities are also discussed.
Footnotes
Acknowledgements
The author would like to thank Woodlands Health Campus (WHC) for having him on-board as a dental consultant to the four WHC CCF@Expo halls, as well as the contribution of dental patients cited in this article.
Author Contributions
The author was the sole person who prepared the article.
Declaration of Conflicting Interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The article did not involve any studies on human subjects, and hence, there was no need for a review by an institutional review board (IRB) or similar ethics committee.
Informed Consent
Approval has been granted by WHC that held the license to operate the six COVID-19 Community Care Facility halls mentioned in the article to publish the patient data contained herein. Approval has also been granted by the author’s employer (the Singapore Armed Forces) to publish this article.