
Abstract
The aim of this study was to describe the impact of the COVID-19 pandemic on dementia care from a multiple stakeholder perspective. We used a multi-method design, with a cross-sectional survey followed by focus groups/interviews. Surveys were completed by people living with dementia (n = 27), family caregivers (n = 161), and health and social care professionals (n = 77). A sub-sample (n = 55) participated in an interview or one of 9 focus groups. Surveys were analyzed with descriptive statistics and focus group/interview data were analyzed using a thematic approach. Participants reported an impact of COVID-19 on dementia care, including less access to care and resources for care. Telehealth and tele-support/education were reported to be effective alternatives to support care. Themes from the qualitative data about dementia care were: (1) planning and providing care, (2) making choices around risk and safety, (3) experiences of loss, and (4) technology and dementia care. The results of this study present opportunities to improve the quality of care through addressing inequities and identifying improved and innovative approaches to address social isolation and virtual care for this vulnerable population.
Background
Older adults are especially vulnerable to the effects of the ongoing coronavirus 2019 (COVID-19) pandemic and among this group, people living with dementia (PLWD) warrant particular consideration. Dementia has been labeled a pandemic in our aging society and coupled with the COVID-19 pandemic, raises great concerns about the care for PLWD and their families (1). PLWD have been found to be at higher risk of contracting COVID-19, are more likely to require hospitalization, and are more likely to have severe or fatal infection compared with people without dementia (2). Furthermore, a growing number of studies are reporting the adverse impact of COVID-19 and the public health interventions to mitigate the spread of COVID-19 on the well-being of both PLWD and family caregivers (3–7).
Accessing health and social services is key to supporting the well-being of PLWD and their family caregivers. Health and social support in the community including adult day programs, home assistance, and support groups reduced services or transitioned to a virtual environment (6,8–10). A telephone survey in the United Kingdom, with 61 PLWD and 285 caregivers, reported an overall decrease in service hours since the beginning of the pandemic, with higher variability in-service hours associated with increased anxiety for PLWD and lower levels of mental well-being among caregivers (11). While these reports and others describe the reduction in services or subsequent adaptations and make recommendations for dementia care, there is limited empirical evidence that focuses specifically on the experiences and perceptions around dementia care during COVID-19 from both those giving and receiving care. The purpose of this study is to describe the impact of the COVID-19 pandemic on dementia care from the perspectives of PLWD, family caregivers, and health and social care professionals (HCPs).
Methods
A multi-method approach was used, with cross-sectional surveys completed by PLWD, family caregivers, and HCPs, followed by focus groups/individual interviews with a sub-sample of participants. This study was conducted using a community-engaged research approach, partnering with community members who participated in a Stakeholder Advisory Council (SAC). The SAC was comprised of people who were personally and professionally impacted by dementia (12). The Council initiated the study question, helped design the survey instruments, and participated in the collection and interpretation of the data.
This study was approved by the UT Health San Antonio Institutional Review Board (IRB) (HSC20200790E). Given the virtual nature of the study, the IRB waived written consent for both the surveys and the focus groups. Participants were presented with an information sheet to review prior to proceeding with the survey, with consent implied if they continued with the survey. Participants in interviews and focus groups were provided information about the study and their verbal consent was obtained before proceeding with the study.
Study Sample
Participants were eligible to participate if they were > 18 years of age, identified as a PLWD and community-dwelling, family caregiver, or HCP with experience in dementia care, and spoke English. We did not use a scale to measure capacity for PLWD but instead relied on a process consent method (13). This method includes different approaches to presenting the study information, assessing their understanding, and revisiting the purpose throughout the study. We discussed the study prior to beginning the focus groups/interviews to assess participants’ ability to participate and revisited the purpose throughout the focus group/interview. Convenience sampling was used for both the quantitative and qualitative aspects of the study. SAC members reached out to their networks and shared information about the study, and we shared a link to the study with our community and clinical partners and through a national listserv. SAC members also collected some surveys by telephone with PLWD and caregivers who did not have access to computer technology. Upon completion of the survey, participants were invited to participate in a focus group/interview. Participants in the qualitative part of the study included those individuals we were able to contact and schedule for an interview.
Procedures
Survey instruments were developed in collaboration with the SAC. We examined the current literature around dementia and COVID-19 as well as a database of scales for assessing COVID-19 domains for clinical or population research (14). We were unable to identify a scale fit for purpose to assess the impact of COVID-19 on dementia care but were able to use some items from identified surveys to include in the surveys for this study. Although there were some common questions across the 3 surveys, a specific survey for each group was created, with the surveys managed on the Research Electronic Data Capture (REDCap) (15). Survey data collected included basic demographic information, the impact of COVID-19 on aspects of quality of life for PLWD and caregivers, and questions about COVID-19 and healthcare for all participants. Surveys were completed between November 2020 and January 2021.
The focus group guide was developed in collaboration with the SAC and included questions about their experiences during COVID-19 and strategies that were helpful in care provision (Supplemental Table S1 for full guide). Nine focus groups (5 with caregivers, 2 with HCPs, and 2 with PLWD), as well as 3 interviews with PLWD who felt more comfortable to participate in an individual interview, were held between January and March 2021.
Data Analysis
Data from the surveys were analyzed with frequencies (percentages) and means (SDs) for categorical and quantitative descriptive statistics, respectively, using Stata 16.1. Focus groups and interviews were audio-recorded, transcribed, and analyzed using an inductive thematic analytical approach. Three doctoral students, one researcher, and one SAC member (family caregiver) participated in the qualitative analysis. A first transcript was reviewed by all team members to develop the initial codes. Following that, each transcript was independently reviewed by 2 team members and then brought to the team for discussion. Codes were merged to develop the overarching themes upon achieving thematic saturation (16). Credibility of the analysis and interpretation is demonstrated through the expertise of the team. The multiple quotations with voices of the participants as well as a review of the same transcripts by multiple study members support confirmability (17).
Results
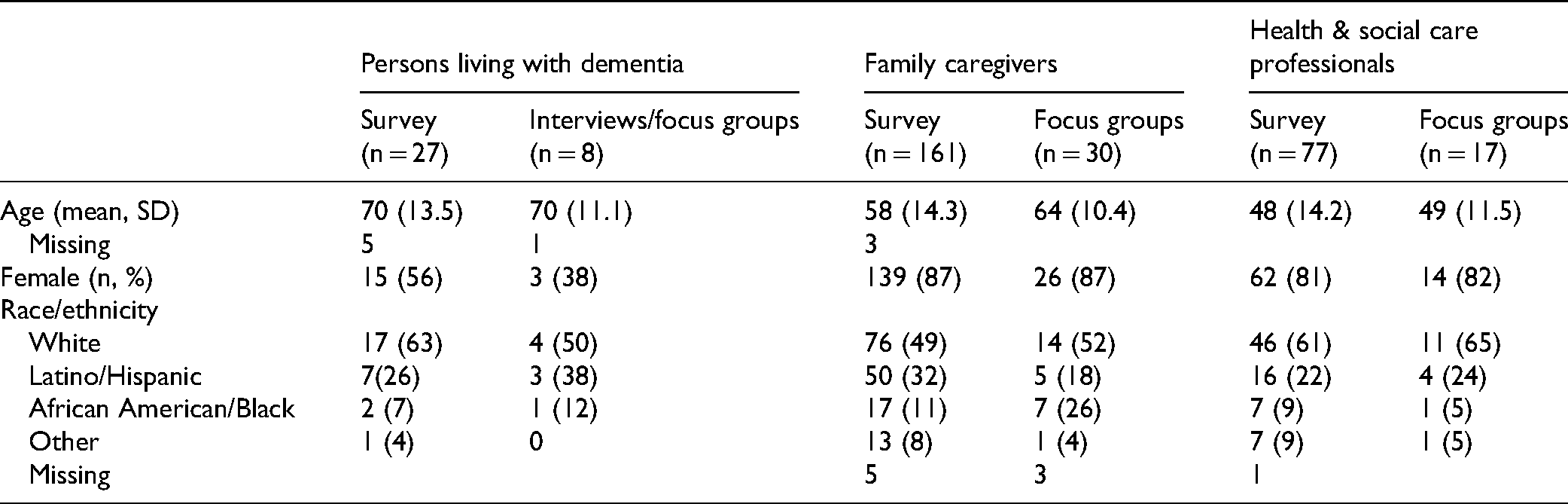
There was a combined total of 265 PLWD, family caregivers, and HCPs who completed surveys, the majority residing in Texas (90%), and of these, 74 people said they were interested in participating in a focus group or individual interview. From this group of 74, we were able to contact and schedule 55 people to participate in an interview or focus group, with group sizes ranging from 2 to 8 (Table 1). Most caregivers were providing care for a parent (survey 56%, focus group 77%) or their spouse (survey 31%, focus group 47%). HCPs who participated in the study included social workers, chaplains, nurses, occupational therapists, physicians, as well as personnel from memory care facilities, adult day programs, and other community programs such as the Alzheimer's Association (data not shown).
Demographics of Participants.
The supplement (Supplemental Tables S2 to S4) provides the complete surveys for PLWD, caregivers, and HCPs along with their responses. Here we present the data specifically as it relates to the impact of COVID-19 on dementia care.
Participants across groups reported an impact of COVID-19 on dementia care (Tables 2 to 4). HCPs reported reduced access to care (somewhat to extremely, 77.2%) and over half of caregivers (64.8%) and PLWD (51.9%) reported that they had delayed or canceled an appointment. Both caregivers and PLWD worried about attending appointments related to COVID-19 (somewhat to extremely, 70.8% and 46.1%, respectively). Telehealth and tele-support/education were reported to be somewhat to extremely effective alternatives by over 75% of HCPs, with 75% of caregivers accessing telehealth and 50.8% accessing tele-support/education. Most caregivers were somewhat to extremely satisfied (83.4%) with telehealth for their care recipient's needs. Both HCPs (95.7%) and caregivers (83.9%) felt confident in access to information to guide care, including information to weigh risks and necessary precautions around COVID-19. Caregivers (87.9%) and PLWD (61.5%) felt somewhat to extremely concerned about the impact of COVID-19 on their healthcare, although both caregivers (82.3%) and HCPs (90.3%) were confident in the care they were providing to PLWD. Across respondent groups, all reported a decline in the health and quality of life of both PLWD and caregivers. Caregivers expressed somewhat to extreme worry about contracting COVID-19 themselves (65.4%) and even more so for the PLWD (81.5%).
Perspectives of Health/Social Care Professionals on Dementia Care During Pandemic.

Abbreviations: PLWD, Person living with dementia; CG, caregiver.
Sample size varies across questions related to missing data.
Perspectives of Family Caregivers on Dementia Care During Pandemic.

Abbreviations: PLWD, person living with dementia; CG, caregiver.
Sample size varies across questions related to missing data.
Perspectives of PLWD on Dementia Care During Pandemic.

Abbreviations: PLWD, person living with dementia; CG, caregiver.
Sample size varies across questions related to missing data.
Qualitative Findings
The following themes related to dementia care were identified from the focus groups and individual interviews: (1) Planning and Providing Care, (2) Making Choices around Risk and Safety, (3) Experiences of Loss, and (4) Technology and Dementia Care.
Planning and Providing Care
Consistent across groups, participants described challenges around planning and providing care related to COVID-19. This included planning for future care as well as concerns about the resources available to support current care. Plans for care were disrupted and some were put on hold. “I've had care partners who, you know, if it weren't COVID happening, they would be moving toward finding a place for their loved one to live, moving them toward a residential setting. But here we are a year later, and their person is needing a lot more care. So I'm seeing that kind of, frankly, dangerous situation” (HCP). In the face of challenges in planning care, there was also a sense of urgency brought about by COVID-19 to ensure that care plans were in place, not only for the PLWD but also plans for care should the caregiver contract COVID-19 or something else happen to them. “So COVID, if nothing else, brought this to everybody's attention that you need to think about your loved one and planning for care. But you also need the plan B, thinking about yourself. If something happens to you, what's going to happen to the person you are caring for?” (CG)
There was uncertainty related to the availability of resources across settings for care provision. “The struggles of keeping their parents or loved ones that have different forms of dementia engaged and entertained, having social interactions, and things like that. With day programs closed, COVID really brought on a lot more of difficult times for our caregivers” (HCP). Across focus groups, caregivers expressed the challenges of providing care during the pandemic, aptly described by one caregiver as “caregiving on steroids.” The limited community resources left caregivers to take on the additional care. “So it was very hard and I needed a break but no one came because no one wanted to get sick and I was now picking up those other roles and responsibilities” (CG). For those caregivers with a family member in an institution, they noted the difficulties for facilities who often relied on the support of family members to assist with care. “They weren’t ready for it. I do recognize that was very hard on the facilities during COVID because they did not, they rely so much on us to assist. They, you know, we partner with that facility” (CG).
Making Choices Around Risk and Safety
Participants described the difficult choices to mitigate risk and ensure safety, while providing patient and family-centered care. “And that was a struggle that he had, you know, is he making the right choice of allowing her to continue on with, you know, three or four friends, because it brings her so much joy, and she's so much happier having that interaction versus the risk that you know, of her contracting COVID” (HCP). Family caregivers described difficulty balancing public health measures with seeing the effects of social isolation. “I think for me during that time of COVID, the hardest thing was that I saw him forget me quicker, because I couldn't be there. And then when I was there, I'm the stranger behind this mask. And what sense does that make?” (CG). A PLWD also described choices she was making around managing risk. “When you are isolated, you’re not challenging your brain. I am missing that social piece that works your brain … so these are my concerns about what I am losing to manage risk” (PLWD).
There were difficulties in explaining and managing safety precautions for the PLWD. “And so just reiterating, ‘What's going on?’ ‘And do I have to wear a mask in the house?’ and ‘how come we can't see the kids?’ Just did not, did not understand at all. And it’s so frustrating” (CG). Risks associated with COVID-19 and isolation were examined within discussions about the quality of life. HCPs described the social isolation they were seeing among older adults and the effects this was having on PLWD. “And so having that quality of life discussion of, you know, hate to put it this way, but quantity, quantity over quality, and, and what do you do” (HCP). HCPs and caregivers in particular discussed their roles in advocating for quality dementia care. “I try to do my best to learn and speak on my grandmother's behalf for her care because it is very important for me, you don’t ever want to stop being an advocate” (CG). HCPs advocated for ways to manage risk at institutional and community levels while providing quality care. “And so to have essential visitors be able to visit the same way the staff do with the appropriate protective wear and testing, we have been advocating really hard” (HCP).
Experiences of Loss
The theme of loss related to dementia care was identified consistently across focus groups/interviews. The loss came in many forms including losing a family member/friend to COVID-19, loss of different aspects of dementia care, perceived loss of cognitive function for PLWD, and loss of connections. HCPs described the many losses and the grief they were experiencing in providing care. The following quotes from participants illustrate these different losses. “And when COVID hit, the emotional and spiritual health workers were banned from the nursing home. We lost that aspect of care” (HCP). Although uncertain whether it could be directly related to COVID-19 or part of the disease progression, participants described loss of cognitive function for PLWD during the pandemic. “And right now my brain is like, I can feel that my Alzheimer's is progressing. And I don't know if it's progressing faster because of the isolation or if it's just part of the disease progression itself. My time is limited because of the Alzheimer's, losing the opportunity to make memories” (PLWD). Family members described the losses they were experiencing with the physical and social isolation. “We lost her and we tried to zoom and she couldn’t you know, she couldn’t follow that. And I couldn’t talk to her on the phone as she wouldn’t understand anyway” (CG). A PLWD described his sense of loss, “a lot of us are kind of isolated, and some may not even have access to, you know, phones and computers and things like that to stay engaged. So I just don’t want us to be forgotten” (PLWD).
Technology and Dementia Care
Utilizing virtual connections for healthcare appointments, caregiver support, and social interactions were seen as vital to supporting dementia care. “It has been crucial to have the lifeline that the technology has provided” (CG). Telemedicine provided a safe way to ensure that people continued to receive healthcare. “So luckily, again for the telemedicine with her neurologists, we were able to, you know, talk and get some solutions” (CG). Caregivers described opportunities to access support and social engagement. “Learning how to Zoom has opened up a lot of opportunities for me to engage in education and support sessions” (CG).
Participants commented on the nature of their interactions through technology. “But the interactions are not the same, that face to face and physical interaction is still something you can't substitute with technology” (HCP). “It's been very, very difficult because she [PLWD] doesn't like the Zoom calls when the doctor wants her to do Zoom calls” (CG). A PLWD described interactions on Zoom in the following way, “And you can still socialize on Zoom. But it's just, it's like, it's an animated socialization without substance. And after a while, I think the substance just, you know, you really miss it.” Despite the advantages of technology, participants described inequities in access and challenges with technology. “There is the disconnection with residents who can’t Zoom, can’t figure it out because of cognition. And then there are those who do not have access to technology” (HCP).
Discussion
We report on the impact of the pandemic on dementia care from multiple stakeholder perspectives, thus providing a more comprehensive understanding. A strength of this study is the participation of the SAC in all aspects of the study, including data analysis and interpretation. This is one of few studies that include the voices of PLWD in understanding the impact of COVID-19 on dementia care (7,11) and the only study of which we are aware that provides information on the pandemic and dementia care from multiple perspectives. This offers new insight into dementia care, highlighting similarities and differences across groups. We utilized the Institute of Medicine (IOM) framework for care to provide a framework within which to interpret our findings. The IOM framework has established 6 domains: safe, effective, patient-centered, timely, efficient, and equitable, which defines quality healthcare (18).
Safety was of utmost importance during the pandemic. Both our quantitative and qualitative findings underscored the choices that were being made to manage safety and risk and how it impacted on planning and providing care. A higher percentage of HCPs than family caregivers reported confidence in the information they received to manage risk, with participants consistently describing the associated challenges in the choices they were making. Most caregivers described missed visits and delays in care for both themselves and for PLWD, related to concerns about leaving their home because of the virus and also to canceled appointments or delays in care. In a cross-sectional study with 73 caregivers, 50% described reported having to delay seeking needed help for themselves, as well as the person they were caring for, described as “foregone care” (19). Caregivers described their central role in supporting the safety of the person they were caring for, but also described the challenges in reinforcing masks, social distancing, and maintaining proper hand hygiene for someone with cognitive impairment. These results are aligned with other studies which similarly reported on the stress for caregivers and their increased vigilance in supporting the safety of their family members living with dementia (5,20,21). HCPs in our study described the challenges in supporting timely and efficient care while ensuring safety. Similarly, many investigators have reported on the challenges around safety that impacted on the timeliness and efficiency of care (9,22,23).
Providing person and family-centered care that was safe and effective was central across participants in the choices and the decisions they made to plan and provide quality care. The alignment of perspectives is shown to be important to person-centered care specifically during the pandemic (24). Data from the surveys and focus groups/interviews highlighted the difficulties related to the pandemic and the consequences on the quality of life for families impacted by dementia. Within both the quantitative and qualitative data, HCPs and family caregivers, in particular, were concerned about the loss of cognitive function for PLWD. There were also important discussions related to the experiences of other losses across groups, including losses around certain aspects of care and social connectedness. These reflect broader discussions that have been taking place during the pandemic in supporting families impacted by dementia and the “acceptable” risk-taking as part of person-centered care (6,7,23,25–27).
Technology and its role in supporting quality care was recognized here as well as in other studies (22,28–31). While it took time to transition from the traditional models of care including office visits, in-person support groups, and other forms of education and social engagement activities for families impacted by dementia, those who engaged in virtual care and other forms of support were generally satisfied and HCPs were confident that they were able to provide quality care. The transition to technology, however, has served to deepen the digital divide and the inequities in care for those without access to technology and for those who find communication through technology difficult (32–34), in particular as reported by PLWD in this study.
Limitations
Convenience sampling methods were used for both the quantitative and qualitative parts of the study, which limits the generalizability of the findings. While we attempted to represent diverse stakeholders in this study, since we conducted the study electronically, the results are representative of those persons who are able to access and are comfortable using technology. We did collect some surveys by telephone for those without digital access, but this represents a small percentage of participants. Although we aimed for diversity in race/ethnicity, our samples were approximately 50% White. The survey utilized for the study was developed in partnership with the SAC which we believe supports face validity and they reviewed the items for readability. This survey instrument, however, was not tested for reliability or further validity which may limit the findings. This study took place during the end of the first year of the pandemic, was cross-sectional, and thus reflects perspectives at that time.
Conclusion
This in-depth examination of the impact of the pandemic on dementia care can inform future health and social care to ensure that we provide quality care as defined by the IOM.(18) Results from this study highlight opportunities to improve the quality of care through addressing inequities in care and supporting improved approaches to address social isolation and virtual care. The greater use of telehealth can have important advantages for families impacted by dementia including avoiding travel time and waiting time in crowded clinics. The current context affords opportunities to evaluate technologies that are effective in providing cognitive stimulation and reducing the harmful effects of social isolation for PLWD. The use of virtual technology including telehealth, however, was challenging for some PLWD and this underscores the need to consider other strategies to provide health and social care, such as home visits. The findings from our study reinforce the need for future care planning, not only for the PLWD, but considerations about care should the caregiver be unable to provide care, as was reported by families during the pandemic. These recommendations can inform dementia care during the ongoing pandemic and prepare us for other future situations where social distancing and virtual care may be required.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221112208 - Supplemental material for A Multiple Stakeholder Perspective on the Impact of COVID-19 on Dementia Care
Supplemental material, sj-docx-1-jpx-10.1177_23743735221112208 for A Multiple Stakeholder Perspective on the Impact of COVID-19 on Dementia Care by Carole L. White, Sara S. Masoud, Ashlie A. Glassner, Shanae Rhodes, Mayra Mendoza and Kylie Meyer in Journal of Patient Experience
Footnotes
Acknowledgments
We gratefully acknowledge the contributions of the members of the Stakeholder Advisory Council.
Authors’ Contributions
Conceptualization: [CW, SM, MM]; Methodology: [CW, SM, AG, MM]; Formal analysis and investigation: [CW, SM, AG, SR, MM]; Writing—original draft preparation: [CW]; Writing—review and editing: [CW, SM, AG, MM, KM]; Funding acquisition: [CW].
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article [and its supplementary information file].
Consent for Publication
All participants provided verbal consent.
Data Statement
The data has not been previously presented orally or by poster at scientific meetings
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
This project was approved by the Institutional Review Board at the University of Texas Health Science Center San Antonio (HSC20200790E).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Patient-Centered Outcomes Research Institute, (grant no. Eugene Washington Engagement Award (10725-UTHSC), National Institute of Aging P30AG066546 (South Texas Alzheimer’s Center).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.