
Abstract
Empathy is a cognitive attribute that forms the cornerstone for good doctor–patient encounters. The formative period for the development of empathy toward patients begins with clinical encounters within medical school. An individual medical student's empathy levels may in part be a product of their resilience and perfectionist attitudes. A cross-sectional study with 320 medical students across all years of study was conducted to determine the correlation of perfectionism and resilience with clinical empathy in medical students. The JSE-S, CD-RISC 10, and APS-R scales were used to assess levels of empathy, resilience, and perfectionism, respectively. The study found that a positive correlation exists between resilience (r = 0.174) and academic year with empathy, and a negative correlation exists between maladaptive perfectionism and empathy (r = −0.138). The resilience score declined progressively as the year of study progressed with a statistically significant. Mean empathy scores were lowest in fifth-year students (96.8 ± 12.5) and highest in third-year students (107.8 ± 13.2). Further longitudinal studies are necessary to better understand the impact of resilience and perfectionism on empathy.
Introduction
Clinical empathy has been defined as the ability to “a) to understand the patient's situation, perspective, and feelings (and their attached meanings); b) to communicate that understanding and check its accuracy; and, c) to act on that understanding with the patient in a helpful (therapeutic way)” (1). Low levels of clinical empathy have been shown to cause patients to harbor dissent and disappointment toward physicians and to decrease health-seeking rates and patient satisfaction (2). Ventures to increase empathy as expressed by physicians therefore have the potential to enhance the patient's experience in clinical encounters through better situational comprehension and meaningful communication resulting in impactful shared decision making and higher rates of patient compliance (3).
Recent studies have shown that several factors may have a modulating effect on an individual's empathic experience including apriori attitudes, stereotypes, group preferences, and group membership (4–6). Similarly, another study has shown how individuals raised within a lower socioeconomic background tended to show a greater frequency of empathic attitudes as compared to participants from the higher socioeconomic background (7). In medicine, factors such as age and gender have been shown to have a modulating effect on one's clinical empathic experience (8).
Moreover, recent advancements in the field of social neuroscience have shown that components of empathy depend on brain processes that mature later in the development process and can be altered by environmental factors and experiences (9). Hence, empathy is seen as a skill or ability, which could potentially be harnessed, trained, and modified if an understanding of these factors is developed. These brain processes are also impacted by the resilience and perfectionist tendencies in an individual, and this article focuses on the impact of these factors on clinical empathy (10,11).
Resilience is the capacity of oneself to withstand and to recover from significant hardships threatening stability, viability, or development (12,13). Physicians and medical students who exhibit such resolve have reduced burnout and dropout rates (14,15). This may be attributed to increased tolerance of stressful circumstances including prolonged, high-intensity health care exposure, drastic shifts in work–life balance, and the burden of exams as well as which are all responsible for the decline in empathy (16,17). Hence, it is expected that higher levels of resilience to such circumstances will help medical students preserve empathy. However, the relationship remains largely unexplored (18,19).
Perfectionism, the degree to which an individual achieves flawlessness, may also have a role to play in this framework surrounding empathy (20). Perfectionism largely exhibits itself in 2 forms: adaptive and maladaptive. Maladaptive perfectionism occurs when individuals remain highly self-critical when personal demands are not met and are highly prevalent in medical students, correlating with lower self-acceptance, as well as higher depression and burnout rates (21–23). High levels of maladaptive perfectionism may exacerbate the stressors. However, the correlation of perfectionism with empathy remains largely understudied.
Characterizing the modifiable factors that influence and modulate clinical empathy will advance its understanding and direct the focus of measures taken to enhance levels of empathy. Therefore, the aim of this study is to describe the association of resilience, perfectionism, and empathy with each other, and with the year of study in medical students.
Methodology
A cross-sectional survey was conducted during December 2019 among undergraduate medical students above the age of 18, enrolled in a medical undergraduate program at a private medical college located in Karachi, Pakistan. Of 500 students in the medical college, a total of 320 medical students were selected from all 5 batches, using stratified random sampling. If a student identified in stratified random sampling didn't give consent, another student was randomly selected from the same batch (strata). This survey achieved 80% power and 95% level of confidence, accounting for a 10% chance of incompletion.
Questionnaire
The following assessment tools were used in their original language (English) to assess levels of empathy, resilience, and perfectionism:
Jefferson Scale of Empathy S Version’ (JSE-S)
Empathy was assessed using “The Jefferson Scale of Empathy S Version” (JSE-S), a 20-item instrument that uses a 7-point Likert-type scale to measure empathy in healthcare professionals (24). The S version is designed for medical students. The scale has been validated in countries globally, including Pakistan (25,26). Previous literature has reported that this questionnaire has a validity of 0.7, test–retest reliability of 0.65, and alpha reliability coefficient of 0.9 (27). Permission to use the scale was obtained from Thomas Jefferson University.
Connor-Davidson Resilience Scale (CD-RISC 10)
Resilience was measured using the CD-RISC 10 tool, an instrument containing 10 questions to be answered on a 4-point Likert-type scale, with the output being in the form of a score between 0 and 40. This is an abbreviated version of the original CD-RISC scale, developed based on factor analysis at the University of California, San Diego (28). In literature, the validity of this scale has been reported as 0.83, test–retest reliability as 0.87, and alpha reliability coefficient as 0.89 (29).
Almost Perfect Scale-Revised Version (APS-R)
Perfectionism was measured using The Almost Perfect Scale-Revised (APS-R), assessing 3 variations of perfectionism: High Standards, Order, and Discrepancy. Participants responded to 23 scenarios in the instrument, which uses a 7-point Likert scale. Total scores for the entire scale range from 23 to 161 with individual scores for each category. The APS-R was used to classify perfectionists into 2 groups: adaptive and maladaptive. High scores in the Standards and Order subscales indicated perfectionism, whereas a high score in the Discrepancy subscale indicated Maladaptive perfectionism (30). The Cronbach's alphas of the subscale scores, according to previous studies, ranged from 0.82 to 0.92, and internal consistency coefficients (validity and reliability) for the APS-R ranged from 0.85 to 0.92 (30).
Data Analysis
Data were entered twice and cross-analyzed to avoid any discrepancies. Data analysis was conducted using IBM SPSS Statistics 21. Baseline characteristics are presented as mean score ± standard deviation for quantitative variables, and frequencies with percentages for qualitative variables.
Comparison of means in baseline characteristics was done using analysis of variance (independent t test) for continuous variables. The perfectionism scale was categorized into adaptive and maladaptive, and crosstabs were used to compare frequencies for each baseline characteristic.
The correlation between 2 continuous variables (empathy score and resilience score) was determined using bivariate Pearson's correlation and was displayed using a scatterplot with a line of best fit. Perfectionism and empathy scores were compared using linear regression. Perfectionism was categorized into adaptive and maladaptive, and adaptive perfectionism was used as a reference category when performing linear regression. The mean empathy score of each year of study (Years 1-5) was assessed using the interquartile range and presented as box-and-whiskers plot. Dummy variables were created for each year of study, using Year 1 as reference category. Comparison between the 2 variables was done using linear regression. A P value of less than .05 was considered to be statistically significant.
Results
Of the 320 students interviewed, 190 (59.4%) were male, and 209 (65.3%) were below the age of 22 years (Table 1). It was observed that females had a slightly higher, but statistically insignificant, mean empathy score as compared to males (104.2 ± 15.1 vs 101.1 ± 14.0). In terms of resilience, males had a slightly higher mean score (38.3 ± 5.4 vs 36.5 ± 6.0), and the mean difference of 2.0 was statistically significant. Moreover, 66.9% females were found to be maladaptive perfectionists, comparable to 66.3% of males (Supplemental Table 1). However, the difference was not statistically significant.
Baseline Characteristics of Participants in a Study on the Impact of Perfectionism and Resilience on Empathy.

Correlation of Empathy Scores With Resilience
Empathy scores in relation to resilience showed a weak positive correlation of 0.174, which was found to be statistically significant. Hence, increasing levels of resilience correspond with slightly higher levels of empathy.
Correlation of Variable With Medical Year of Study
As observed from our results, the mean score of empathy peaked in the third year of medical education (107.8 ± 13.2) and it was lowest in final year medical students (97.8 ± 17.0) (Figure 1 and Supplemental Table 1). This difference in mean empathy score regarding year of study was found to be statistically significant from the reference first year empathy levels for third-year medical students only (Table 2).
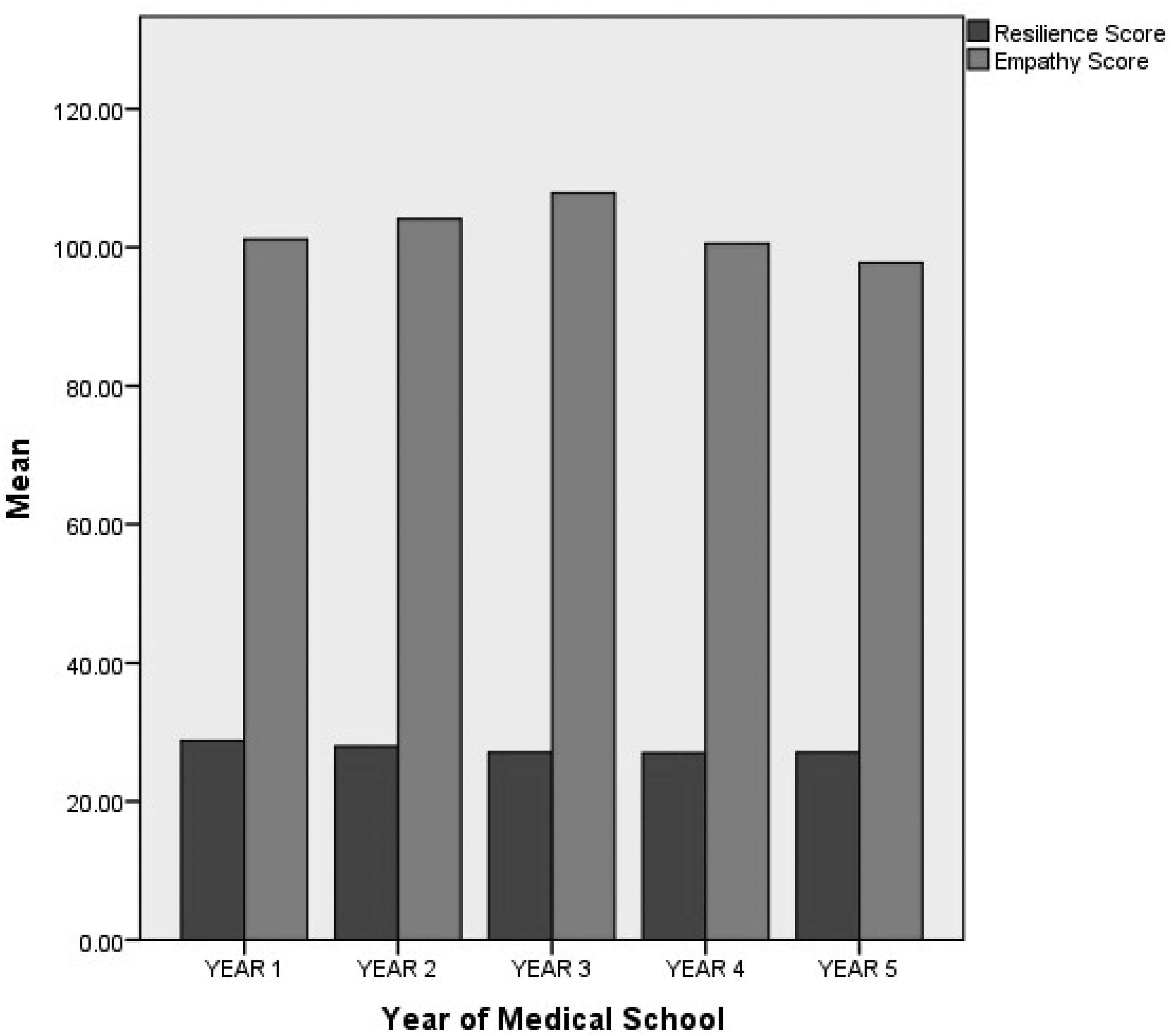
Variation in resilience and empathy score across each year of study among medical students.
Correlation Between Year of Medical Education and Perfectionism With Empathy Score in a Study on the Impact of Perfectionism and Resilience on Empathy.

Correlation between empathy and year of education was significantly different for each year, with a maximum coefficient of 0.185 for third years, taking first years as reference. Hence, as first-year students’ progress to third year their empathy would increase by a factor of 0.185. A weak positive correlation was found between the year of study and empathy score in the first 2 years of medical education (Table 2).
The mean resilience score in first-year students was 38.7 ± 5.2, which declined progressively as the year of study progressed (Figure 1). This linearity was found to be statistically significant. Maladaptive perfectionism was found to have the highest proportion amongst third-year medical students (50 (76.9%); Figure 2).
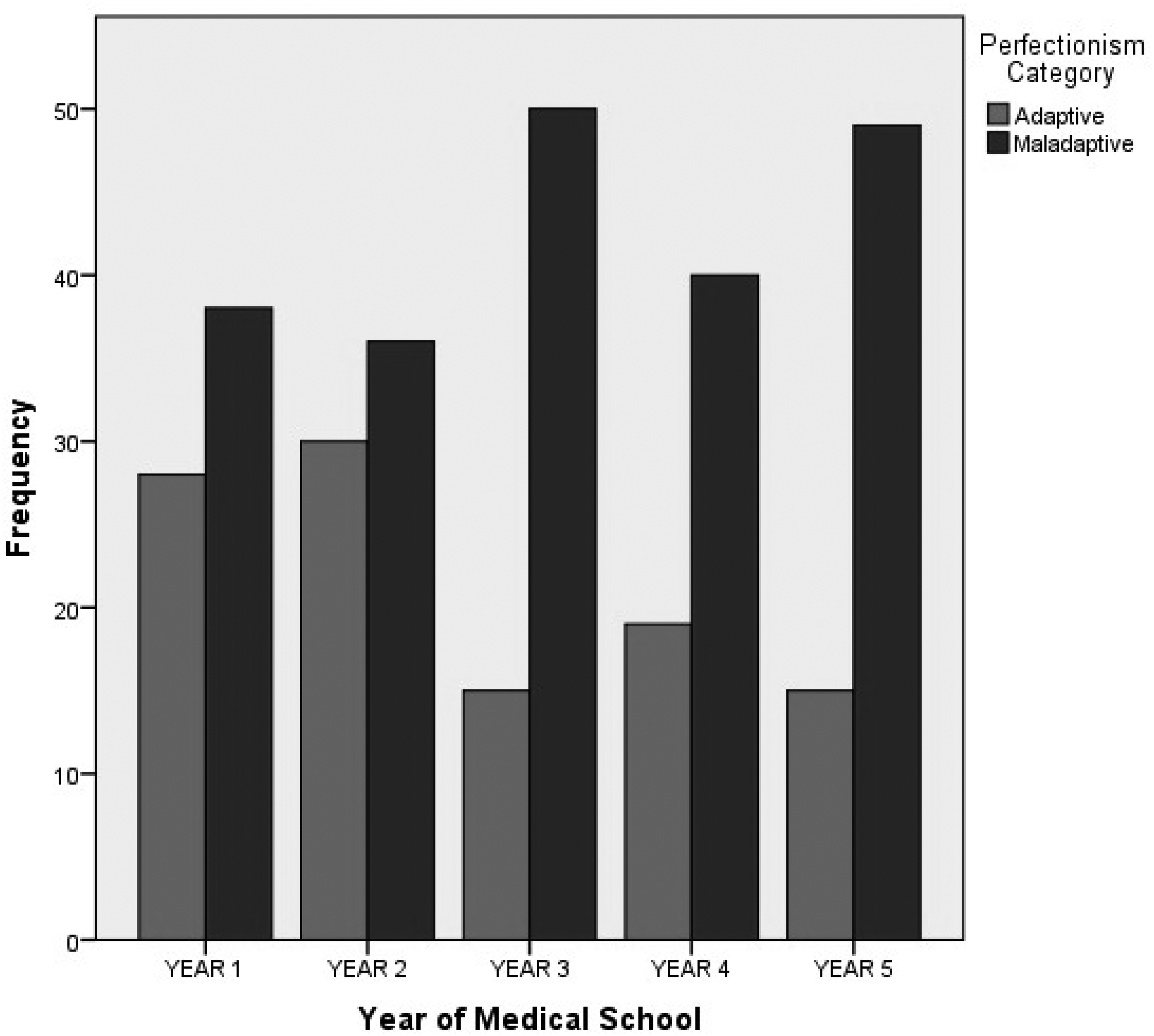
Variation in the proportion of students with adaptive and maladaptive perfectionism across each year of study among medical students.
Correlation of Empathy Scores With Perfectionism
Empathy scores in relation to maladaptive perfectionism showed a weak negative correlation (r = −0.138), which was statistically significant. Hence, higher levels of maladaptive perfectionism correspond with lower levels of empathy (Table 2).
Discussion
The study found a statistically significant negative correlation between perfectionism and empathy (r = −0.138), and conversely, a significant positive correlation between resilience and empathy (r = 0.208) across all years of study. Empathy is a cornerstone of physician–patient interactions. Higher scores on instruments designed to quantify healthcare provider empathy have shown to have a positive impact on patient experience in a myriad of scenarios, including continued control of laboratory parameters in diabetic and dyslipidemic patients, in management of anxiety during clinical encounters, and in primary care consultations in areas of socioeconomic disparity (31–33). An understanding of the factors modulating empathy becomes increasingly relevant with the surfacing of research that shows that the experience of clinical empathy involves affective and cognitive neural processes (34,35). This study was an initial attempt at characterizing the psychological, modifiable variables that modulate clinical empathy.
The significant correlation of resilience and perfectionism with empathy suggests that they may have an impact on the cognitive responses that modulate clinical empathy. Previous studies conducted on finding a relationship between resilience and clinical empathy yielded a positive correlation of 0.36 and 0.375 in France and South Korea, respectively (18,36). The relationship between perfectionism and clinical empathy has not been previously explored, to the best of the author's knowledge.
However, the magnitude of both correlations is weak which suggests that perhaps, while perfectionism and resilience are components of the cognitive process that modulate empathy, it is a multifactorial response, and further understanding of other factors that modulate empathy is needed. It can be further understood by breaking down the empathetic response into 3 phases. Phase 1 is the inner process of empathetic listening to another who is personally expressive in some way, reasoning, and understanding; phase 2 is the attempt to convey an empathetic understanding of the other person's experience, and phase 3 is the client's actual reception or awareness of this communication (37). Highly resilient individuals who can recognize their own hardships and develop appropriate measures to endure may similarly be able to work through the 3 stages of the empathetic response, as their resiliency is an easily translatable skill from the “self” to the “other.” If, however, they are limited to recognition of the self and are unable to generate an appropriate awareness for others, they may be perceived to lack empathy. A similar paradigm can be proposed for individuals with low resilience. Less resilient individuals who may display adequate empathy may be able to perceive distress for both self and others but are only able to generate an appropriate action for others, as some distance from the issue may help gain perspective. On the other hand, if a person is nonresilient because of a lack of perceptivity and not a lack of action, they may also seem unempathetic as they are similarly imperceptive toward the affliction of others.
This study also allows us to analyze the impact of the current medical curriculum on levels of empathy, resilience, and perfectionism. For this purpose, it is imperative to describe the existing framework of progression of students through the medical undergraduate program. The first 2 academic years are spent studying basic sciences, while accompanied by clinically oriented workshops designed to hone examination skills. These years tend to have minimal patient interaction. This focus shifts once students graduate to the third year, where they are required to attend clinics, ward rounds, and operation theaters, until the end of their undergraduate education. Hence, the crux of issue lies in the transition from second to third year when the additional work burden, patient interaction, and reduced personal time should greatly affect the 3 focal parameters of the study. Of additional relevance is the time frame of the study. Between the 4th and 16th of December, most students are at the beginning of their academic year, having spent an average of 4 weeks in their first module (first and second years) or rotations (third year onward). This signifies an ongoing adjustment periods for those in third year entering their first rotations and those in fourth year who have just completed their first clinical year. A significant spike in empathy levels can be observed in third years. However, the fourth year presents a decrease in empathy, indicating a rebound burnout period for students after their first year of increased duties. Final year students surprisingly trend back toward baseline levels of empathy exhibited in preclinical years but do not reach initial levels of empathy. This observation hints at the interesting notion that though empathy is affected positively by acute clinical exposure, medical education may have detrimental effects on empathy in the long term. These results are comparable with the results from similar studies conducted in Boston, South Korea, and other teaching hospitals in Pakistan (38–40).
A consistently negative trend for resilience was present throughout the 5 years. The decline in resilience is problematic because low levels of resilience are associated with burnout (41,42). The sample of medical students also displayed greater levels of maladaptive perfectionism than effective adaptive perfectionism. It was, however, reassuring to see that mean resilience scores according to the year of study ranged 27.0 to 28.7 which is comparable with the average score measured in university students in other populations (29).
Implications
If correctly attended to, medical education can be tuned to equip future healthcare workers with tools to build clinical empathy, a cornerstone of physician–patient interaction, and curb rates of burnout. Our results provide a better understanding of factors that modulate empathy and may be targeted to improve empathy among medical students. They can also form the criteria by which candidates entering medical schools are assessed to determine the emotional fitness necessary for medical training. This study highlights a need for reassessment of medical education to root out the causes for declining trends in resilience and adaptive perfectionism in clinical years requiring patient interaction. These trends, in conjunction with the correlation of these 2 factors with clinical empathy scores, could portend suboptimal patient experiences and outcomes if unaddressed.
Limitations
This study is characterized by a few limitations. It is a single-center study which poses a challenge to generalize the conclusions to the larger population of medical students. It may also be beneficial in future studies to expand the subjects of the study to residency programs within the hospital to see the impact of a different learning environment on clinical empathy. Moreover, the study uses a self-assessment tool to measure levels of empathy since empathy in students belonging to preclinical years was also measured. A positive correlation between self-assessed levels of empathy and patient's perceptions of physician empathy has been reported. However, the strength and statistical significance of these associations vary greatly, where effectors such as gender, race, and ethnicity may confound data. Regardless, these associations point toward a reasonable self-assessment by physicians of their expression of cognitive/clinical empathy (43).
Conclusion
In conclusion, there exists a significant positive correlation between resilience and academic year with empathy and a significant negative correlation between maladaptive perfectionism and empathy. This study offers insight into the factors impacting clinical empathy and paves the way for further research. Identification of these factors is necessary for programs designed to improve clinical empathy for effective physician–patient interactions as they may cater to improving factors that contribute to higher levels of empathy. Further longitudinal studies are necessary to further understand the impact of resilience and perfectionism on empathy.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221106603 - Supplemental material for Impact of Perfectionism and Resilience on Empathy in Medical Students: A Cross-Sectional Study
Supplemental material, sj-docx-1-jpx-10.1177_23743735221106603 for Impact of Perfectionism and Resilience on Empathy in Medical Students: A Cross-Sectional Study by Wardah Rafaqat, Ashmal Sami, Muhammad Talal Ibrahim, Hamza Ibad, Sheharbano Awais, Ayesha Memon, Fatima Farrukh Shahbaz, Daniyaal Ahmed, Shahzaib Zindani, Abdul Lateef Leghari and Sarah Saleem in Journal of Patient Experience
Footnotes
Authors’ Note
Data can be accessed on reasonable request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.