
Abstract
Whiteboards are ubiquitous fixtures in hospital rooms that may represent a ready-made patient engagement tool; yet, their use has only been minimally explored. This study examined the relationship between a standardized whiteboard communication process and patient activation by using the Patient Activation Measure (PAM®). Participants (N = 172) that were optimally involved in whiteboard communication had significantly higher PAM® scores compared to those who were suboptimally involved. PAM® scores also correlated with self-reported role, with those endorsing active participation scoring higher than passive listeners. Accordingly, this study establishes a positive association between the structured use of whiteboards and patient activation.
Introduction
Evidence from outpatient populations demonstrates that patient engagement, defined as active participation in the care process (1), is associated with improved patient satisfaction, higher adherence to healthy behaviors, formation of more trusting relationships with physicians, and better overall health outcomes (2–5). However, promoting engagement in the inpatient setting has been challenging (6).
Whiteboards have increased in prevalence in hospital rooms and could help address this issue, as they represent a cost-effective means to engage patients during their inpatient stay. Best practice guidelines have already been developed to both standardize and optimize their role in facilitating patient–provider communication (7). Indeed, previous studies using these recommendations have shown that whiteboards aid the patient in the identification of their providers, admission plan, and expected length of stay (8,9). Whiteboards also improve inpatient satisfaction (10), suggesting that their use has broad implications for person-centered care.
Yet, it is unknown whether patients play an active role in whiteboard communication. Indeed, this is the standard of care at most institutions; however, one of the barriers to whiteboard use is the time burden that it imposes on healthcare staff, especially physicians (10). As such, it is important to assess whether patients are being excluded from whiteboard communication in favor of efficiency. Additionally, the association between whiteboard use and patient activation, which is a result of engagement that includes patients’ knowledge, skill, and confidence in managing their health (11), has never been directly studied. Given the benefits of increased patient engagement at the individual level, it is necessary to explore this relationship to further justify to clinicians that integration of whiteboard communication is worthy of their limited time.
The goals of this study were to: 1) assess the role of the patient in the patient–provider whiteboard communication process, and 2) explore the relationship between whiteboard communication and patient activation by using the Patient Activation Measure (PAM®).
Method
Subjects
Two hundred thirty subjects were identified from the general medicine inpatient unit at our institution, a tertiary care academic medical center, between November 2020 and March 2021. All patients were at least 18 years of age and had a length of stay of at least two days. Exclusion criteria included: 1) non-English speaking, 2) vision impairment, 3) deafness, 4) illiteracy, 5) altered mental status, 6) pregnancy, and 7) imprisonment. All patients who met the inclusion and exclusion criteria were asked for verbal informed consent to participate. Of the 230 patients identified, 58 declined to participate (74.9% response rate).
Design
This was an observational cross-sectional study that used patient surveys as the primary method of data acquisition. A pre-study power analysis was conducted with an α = .05, power = .80. The projected minimum sample size was 172 participants. All consenting patients (N = 172) were asked a series of four yes/no questions regarding their role in whiteboard communication during their hospital stay: 1) whether someone explained the purpose of the whiteboard; 2) whether their questions were recorded on the whiteboard; 3) whether the whiteboard was used for education about diagnoses, test results, medications, daily plan, and/or discharge instructions; and 4) whether the patient felt that they were included in whiteboard communication overall. The number of “yes” responses to these questions were used to give each patient a whiteboard experience score ranging from 0 to 4.
These four questions reflect standard whiteboard practices at our institution and were used to dichotomize the sample. Thus, if the patient answered affirmatively to all four questions, we assigned them to the optimal whiteboard communication group (n = 101). Those that answered “no” to at least one question were said to be suboptimally involved (n = 71), as the standard of care had not been met from the perspective of the patient.
Whiteboards
The whiteboards at our institution have defined space to record the healthcare team, the daily care plan, discharge instructions, and questions. Routine practice involves collaboratively completing these whiteboard subsections during bedside rounds with the patient playing a participatory role. Direct healthcare providers were not made aware of this research to gauge the true usage of inpatient whiteboards compared to the existing standard.
Surveys
Patient surveys were administered by study investigators. Question domains included the following: 1) the patient's perceived role in the whiteboard communication process (four questions as described above, plus one additional question asking the patient to categorize their role as either active or passive); 2) demographics; and 3) PAM®, a validated 13-item measure used to quantify the level of patient activation (11). PAM® scores are based on a scale of 0 to 100, with higher scores representing stronger activation. The survey and study design were approved by the hospital's institutional review board.
Data Analysis
Survey data, including PAM® scores, were compared between the two cohorts using either χ2 analyses or two-sample t tests for mean difference. All statistical analyses were conducted in IBM SPSS.
Results
Role in Whiteboard Communication
Among the 172 patients who participated, 84.3% agreed that someone explained the purpose of the whiteboard, 70.9% reported that their whiteboard was used to record their questions, 69.8% confirmed that the whiteboard was used for inpatient education, and 77.9% felt included in whiteboard communication overall. The majority (58.7%) answered affirmatively to all four questions. The remainder of the sample responded as follows: 8.1% answered entirely in the negative, 9.9% had one affirmative response, and 11.6% responded positively to each of two or three questions.
Of those that responded positively to at least one question (n = 157), 37.6% reported an active role in whiteboard communication, while 62.4% endorsed passive participation. Active participation was significantly higher in the optimal communication group (51.5%) compared to the suboptimal group (12.5%), χ2 (1, N = 157) = 23.34, P ≤ .001.
Demographics
Demographics for the two communication groups are compared in Table 1. In both cohorts, most patients were female (52.48% vs 60.56%), Caucasian (81.19% vs 92.96%), and non-Hispanic (96.04% vs 97.18%). The mean age was 58.32 years (SD = 17.20) in the optimal group and 57.86 (SD = 19.31) in the suboptimal group. There were no significant differences between the groups in terms of gender, age, ethnicity, employment status, or education level; however, the number of Caucasian and non-Caucasian participants differed significantly between groups, χ2 (1, N = 172) = 4.81, P = .028.
Comparison of Demographics Between Whiteboard Communication Groups.

Caucasian versus all other races.
≥High school education versus <high school education.
PAM® Scores
Mean PAM® scores were significantly higher in the optimal whiteboard communication group (x̄ = 69.66, SD = 15.58) compared to the suboptimal group (x̄ = 61.40, SD = 13.08); t(170) = 3.65, P < .001) (Figure 1). Additionally, active participation (x̄ = 71.51, SD = 14.70) in whiteboard communication was also associated with higher PAM® scores compared to passive involvement (x̄ = 64.79, SD = 14.56); t(155) = 2.82, P = .005). No other explanatory demographic variable correlated with PAM® scores.
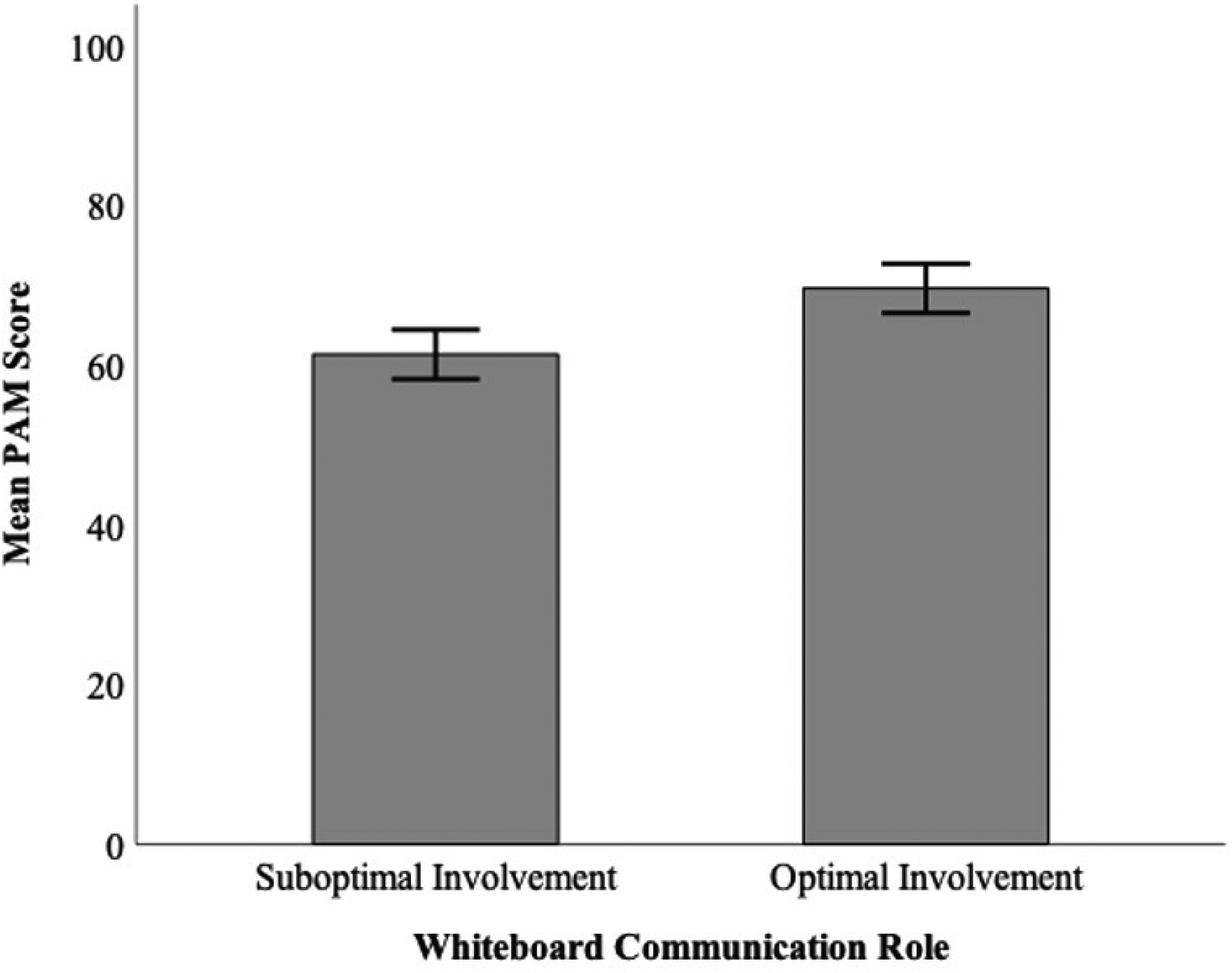
Mean PAM® scores were significantly different between optimal (x̄ = 69.66, SD = 15.58) and suboptimal (x̄ = 61.40, SD = 13.08) whiteboard communication groups t(170) = 3.65, P < .01. Error bars represent 95% confidence intervals.
Discussion
This is the first study to determine the role of the patient during whiteboard communication and to explore the relationship between patient activation and whiteboard use. Notably, most patients endorsed optimal whiteboard communication as measured against the standard of care at our institution. Patients in the optimal cohort were more likely to be active participants in whiteboard communication. On balance, PAM® scores were significantly higher in the optimal communication group, and for those who reported active participation in whiteboard use, irrespective of their communication group. These are significant findings, as increased patient activation has been shown to lower readmission rates (12) and reduce overall costs for healthcare systems (13), suggesting a relationship between structured whiteboard use and meaningful health outcomes.
These results seem intuitive, as physical completion of a whiteboard forces providers to temper the speed of their explanations, incorporate visual cues, and create opportunities for patient input (9). We know that patients and their families find these benefits helpful and frequently interact with the board after providers have left the room (14,15). Thus, the process of completing a standardized whiteboard serves two purposes: it creates a non-threatening space between provider and patient where discussion is fostered; and later serves as a living document, complete with questions, diagrams, and daily plans.
Overall, our findings suggest that most patients are meaningfully involved in whiteboard communication and that these individuals tend to have higher PAM® scores when compared with those who report suboptimal whiteboard communication experiences. This relationship requires further investigation to determine causation; however, whiteboard usage that encourages active patient participation in the four domains we studied may represent a subtle, yet effective way to improve health outcomes for hospitalized patients.
Limitations
Our study has several limitations. The cross-sectional design prevents us from establishing a causative relationship between whiteboard communication and increased patient activation, and it is equally likely that patients with higher baseline levels of activation were more likely to engage in meaningful whiteboard communication. There is also the issue of the racial differences between the two cohorts; however, race itself was not associated with higher PAM® scores. We also excluded non-English speakers from this study, as the whiteboard subheadings at our institution are permanently written in English. Future studies ought to assess whiteboard communication among vulnerable groups, as the benefits may be even more pronounced.
Footnotes
Authors’ Note
This study was approved by the institutional review board at the Milton S. Hershey Medical Center and Pennsylvania State University College of Medicine (Approval Number: STUDY00014160). All procedures in this study were conducted in accordance with the institutional review board at the Milton S. Hershey Medical Center and Pennsylvania State University College of Medicine (Approval Number: STUDY00014160). Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.