
Abstract
Anemia in chronic kidney disease (CKD) is associated with reduced health-related quality of life and physical functioning. This study investigated knowledge and awareness of anemia in patients with CKD in the United States (US) through an online, quantitative survey administered to patients aged ≥18 years with self-reported CKD, with or without anemia. Of 446 patients included, 255 (57.2%) were diagnosed with anemia and 191 (42.8%) were in the non-anemia cohort. In patients with anemia, 71.0% were aware of the relationship between CKD and anemia versus 52.9% in the non-anemia cohort. In the anemia cohort, 46.3% of patients were aware of their hemoglobin level, versus 27.2% in the non-anemia cohort. Despite 67.4% of patients with anemia believing their condition was well/very well managed, only 50% reported being informed about different treatments without prompting healthcare providers. In the US, patients with anemia and CKD perceived that anemia had a negative impact on physical health and emotional wellbeing. Results emphasize a lack of disease awareness, suggesting patients would benefit from further education on anemia in CKD.
Introduction
The prevalence of chronic kidney disease (CKD) in the United States (US) is increasing (1). This increase may be attributed to increases in risk exposure, particularly type 2 diabetes (the leading factor associated with CKD in the US), hypertension, obesity, and an ageing population (1,2). Anemia is a common complication of CKD; of the approximate 37 million patients with CKD in the US (3), nearly 5 million have anemia (4). Anemia in CKD is associated with increased risk of hospitalizations, cardiovascular disease, cognitive impairment, and mortality (5). Appropriate anemia management can improve patient outcomes, as demonstrated in the Trial to Reduce Cardiovascular Events with Aranesp Therapy (TREAT) study; fatigue scores improved for patients receiving treatment targeted to higher hemoglobin (Hb) levels compared with the control group receiving treatment targeted to lower Hb levels (6). There is also a need for renal centers to standardize and individualize anemia management in patients with CKD (7).
While anemia is common in patients with CKD, patients may be unaware of the association between CKD and anemia (8). Symptoms specific to anemia may be difficult to discern from those of progressive CKD due to their similarities (9), contributing to confounding patient perceptions, clinician diagnosis, and treatment decisions, as well as communication between patients and healthcare providers (HCPs). Many patients with CKD and anemia experience reduced health-related quality of life (HRQoL) and physical functioning compared with those without anemia (10). However, the precise contribution of anemia in CKD to reduced HRQoL is difficult to ascertain; it is likely due to comorbidities, CKD progression, and anemia (6).
Although treatments exist for anemia in CKD, evidence suggests that the condition is underrecognized and undertreated (4,11) compared with guideline recommendations (12). Insight into patients’ perceptions of disease, experiences, and needs is important to improve condition recognition, optimize treatment plans, and provide the best possible support at all CKD stages.
Previous studies have identified a lack of awareness and knowledge of disease symptoms in patients with CKD (8,13). In a US study, only 19% of patients were aware of the relationship between proteinuria and poor kidney function, and only 22% understood that CKD may be asymptomatic (13). This lack of knowledge may be influenced by suboptimal communication between patients and HCPs; one-third of patients take a passive role in communicating with their physician, with 28% stating that they did not understand physicians’ explanations of topics related to CKD (8). Understanding patients’ experiences or impact of the illness and treatments on HRQoL is increasingly recognized as key in the US, with organizations such as the National Kidney Foundation and American Kidney Fund launching specific patient platforms for patient engagement and research (14,15). In addition, there is an increasing emphasis on patient-centered care and shared decision making, with researchers seeking patients’ voices through patient advisory boards, leading to improvements in study design, communication materials, and new patient-centered end points (16). This highlights the importance of involving patients in their care through education and support.
This study aimed to understand the experience of patients with self-reported CKD with or without anemia in the US, in terms of their knowledge of anemia, treatments received, and HRQoL. Sources of information used by patients to learn about their condition and their relationships with HCPs were also evaluated.
Materials and Methods
Survey Design and Participants
A quantitative, custom-made, online survey was developed following insights gained from interviews with three clinicians regarding the treatment and management of patients with anemia in CKD. Insight from the clinicians ensured that the survey questions focused on areas of interest to patients and that the questions and possible responses were accurately worded for the intended audience. The survey was developed in collaboration with Portland Communications, London, UK, and was completed between August 29 and September 17, 2018 by 500 consenting patient volunteers from the US aged ≥18 years with self-reported CKD (any stage, on dialysis or not), with or without anemia (the latter acted as a neutral control group); patients with cancer were excluded. Assessment of knowledge and awareness of anemia in the CKD population as a whole, regardless of anemia status, was carried out. It was assumed that patients who had self-reported their CKD would provide accurate insights into their self-awareness of the condition.
A proprietary network, developed by the research firm Opinion Health Ltd, London, UK, was used to identify and recruit patients. Recruitment sources included an online community, patient associations, online support groups, and patient–patient referrals. Portland Communications worked with Opinion Health to carry out recruitment, fieldwork, and data processing. In brief, a random sample of potential patients from the proprietary network were invited to participate in the online survey and sign the consent form. Response rates were monitored and recruitment was not subject to quotas for CKD disease stages. Quality control checks were implemented to prevent duplication of participants. Further details on the survey, including codes of conduct and guidelines followed, as well as patient consent, can be found in the Supplemental Material. The research was carried out in accordance with the European Pharmaceutical Market Research Association Code of Conduct, the European Medicines Agency good pharmacovigilance practice guidelines, and General Data Protection Regulation guidance. All patients provided informed consent and were financially compensated for their time (incentive fee of $5 USD per participant, in accordance with AstraZeneca's guidelines on fair market value compensation). Ethics Committee approval was not sought as this survey was conducted as a market research study.
Data Collection
A survey was developed de novo in collaboration with Portland Communications, London, UK, and was made accessible to participants via an online platform through a weblink sent directly to the email address of each recruited participant. The final survey included 27 questions and aimed to gain insight into patient demographics; knowledge of anemia, its management, and its impact on symptoms and HRQoL; effects on the healthcare practitioner–patient relationship; and information sources for the condition. A full list of the questions is provided in the Supplemental Material.
All information on disease status, including CKD stage, anemia presence and treatments received was self-reported by patients. According to the EphMRA criteria, the market research survey was double blind. Data collected from the survey were aggregated and anonymized to protect patient confidentiality, so that no response could be attributed to any individual. Patient self-reported responses were not confirmed by medical records.
Details on data analysis can be found in the Supplemental Material.
Results
Study Cohort Selection
Of 500 volunteers with CKD who completed the survey, 54 patients reported having cancer or cancer-induced anemia and were excluded from the overall cohort.
Demographics
In the overall cohort (N = 446), 69% of respondents were female, mean age was 52.2 years, with 58% of patients aged ≥51 years (Table 1). The most common comorbidities in the overall cohort were hypertension (67.3%), type 2 diabetes mellitus (29.6%), and hyperkalemia (20.2%). In the overall cohort, the majority of patients had stage 3–5 CKD (67.7%); 22.6% had stage 5 CKD and were receiving dialysis (Table 1). Of the overall cohort, 57.2% (n = 255/446) reported being diagnosed with anemia by their doctor, 34.1% (n = 152/446) reported that they did not have anemia, and 8.7% (n = 39/446) could not remember or were unsure whether they had been diagnosed with anemia (Table 1).
Patient Baseline Characteristics.
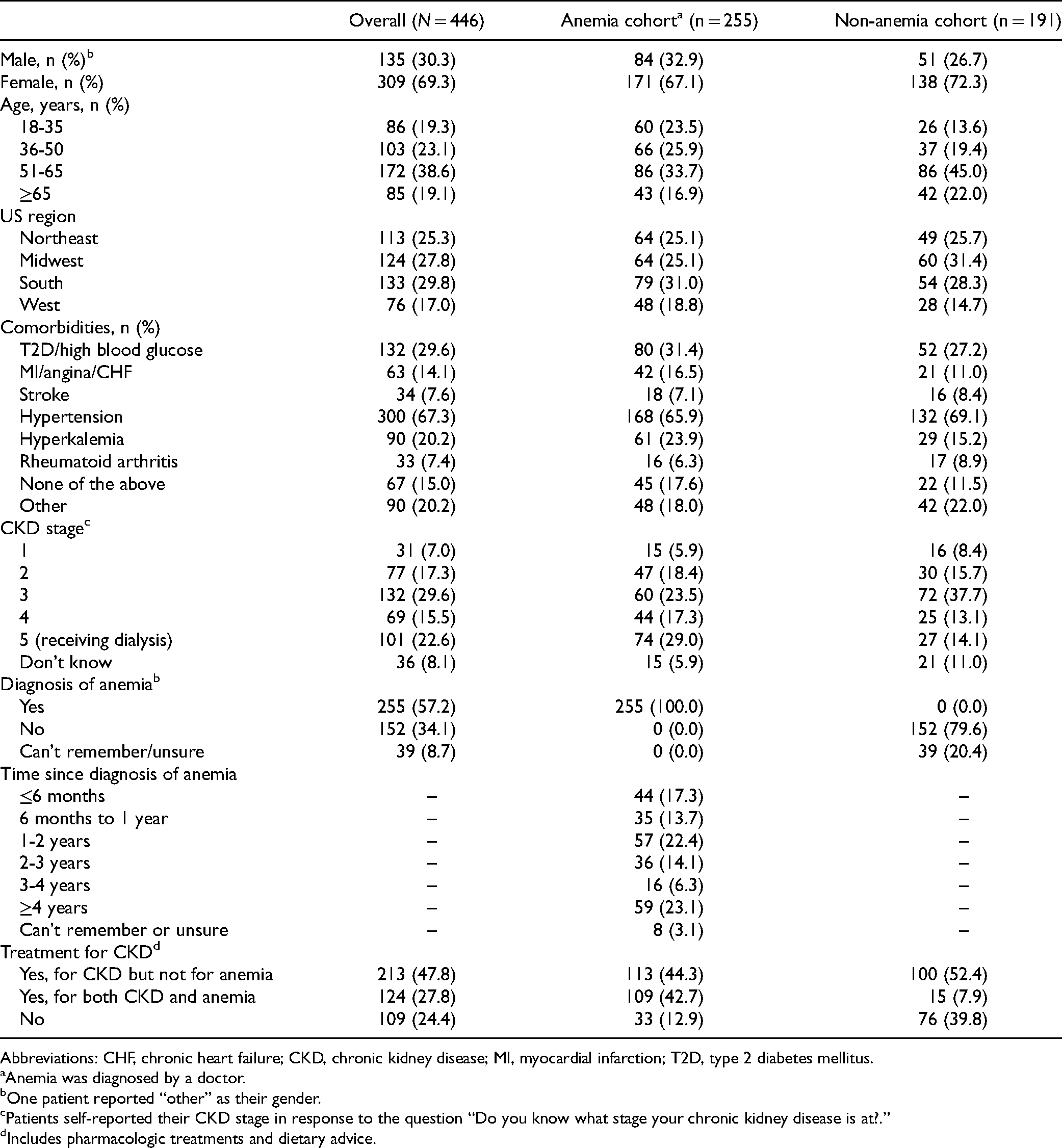
Abbreviations: CHF, chronic heart failure; CKD, chronic kidney disease; MI, myocardial infarction; T2D, type 2 diabetes mellitus.
Anemia was diagnosed by a doctor.
One patient reported “other” as their gender.
Patients self-reported their CKD stage in response to the question “Do you know what stage your chronic kidney disease is at?.”
Includes pharmacologic treatments and dietary advice.
Anemia Disease Knowledge
In the overall cohort, 63.2% of patients were aware of the association between CKD and the risk of anemia; a greater proportion of patients in the anemia cohort (71.0%) were aware of this risk compared with the non-anemia cohort (52.9%). A small proportion of patients in both cohorts had misconceptions about the causes of anemia, such as low blood sugar and irregular heart rhythm (Figure 1A).
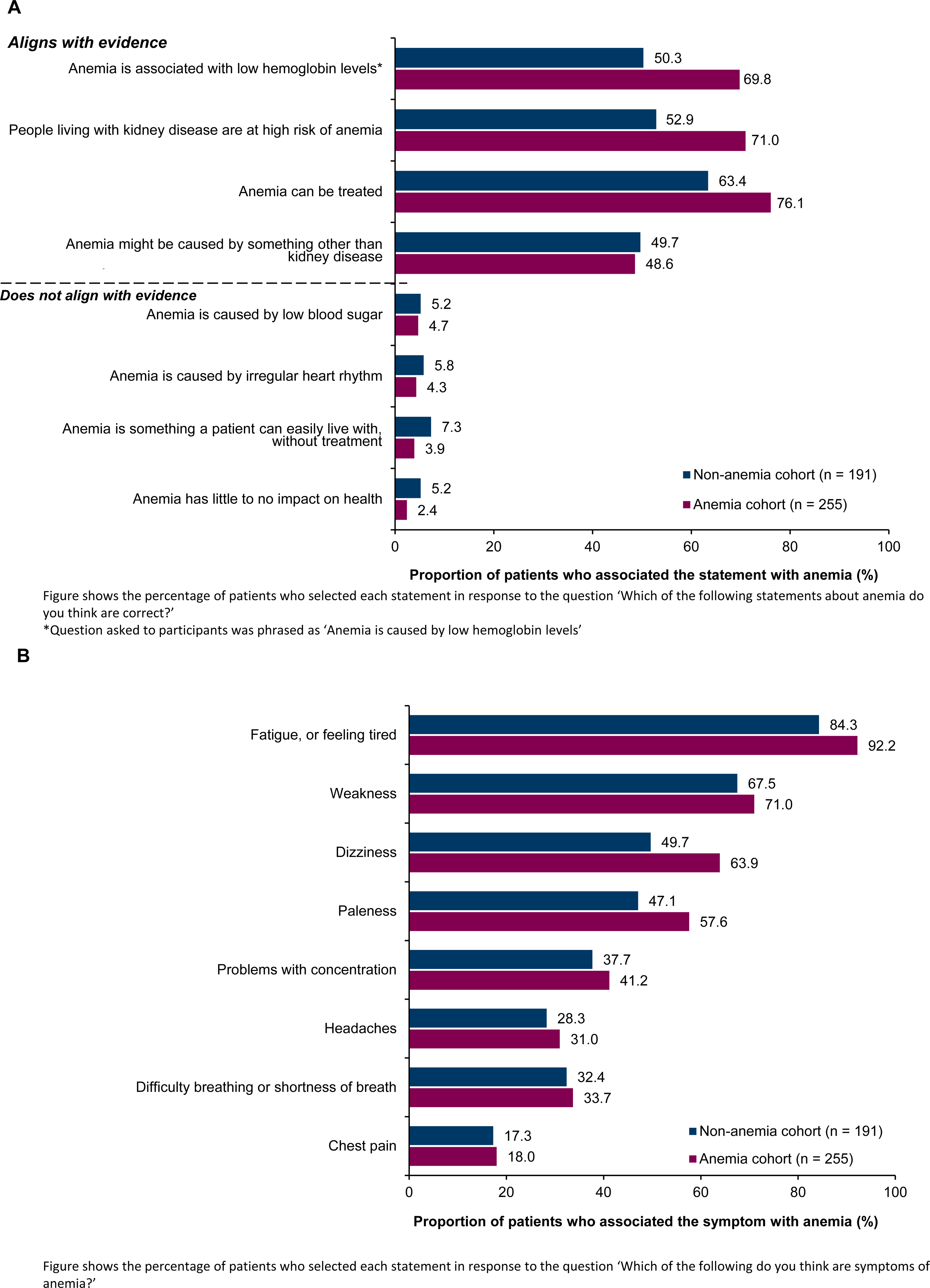
Beliefs about (A) causes of anemia, and (B) symptoms associated with anemia.
Fatigue or feeling tired, weakness, and dizziness, were identified by most patients in the overall cohort as anemia-associated symptoms, with a slightly higher proportion of patients in the anemia cohort identifying these symptoms (Figure 1B).
Of the overall cohort, only 38.1% of patients knew their Hb level, compared with 46.3% of patients in the anemia cohort and 27.2% of patients in the non-anemia cohort. Some patients in both cohorts reported not having had a blood test in the last year (Table 2). The proportions of patients without a blood test in the past year decreased with increasing CKD stage, with all patients with CKD stage 5 having had a blood test (Supplemental Table S1). The proportions of patients who were unaware of their Hb level generally increased with increasing CKD stage (Supplemental Table S1).
Knowledge of Hemoglobin Levels.

Disease Impact on HRQoL
Patients with anemia in CKD indicated that the condition worsened their physical wellbeing (Figure 2A), affecting symptoms broadly divided into the following: fatigue, general malaise and feelings (including feeling ill, pain, and being bothered by side effects), and daily activities. Lack of energy was most frequently identified as being aggravated by anemia in CKD (82.4%; Figure 2B). The impact of anemia by CKD stage on physical wellbeing is shown in Supplemental Figure S1A to E. Anemia and higher CKD stage was generally associated with greater proportions of patients reporting reduced energy levels, time spent in bed, and difficulty meeting the needs of the family (Supplemental Figure S1F).
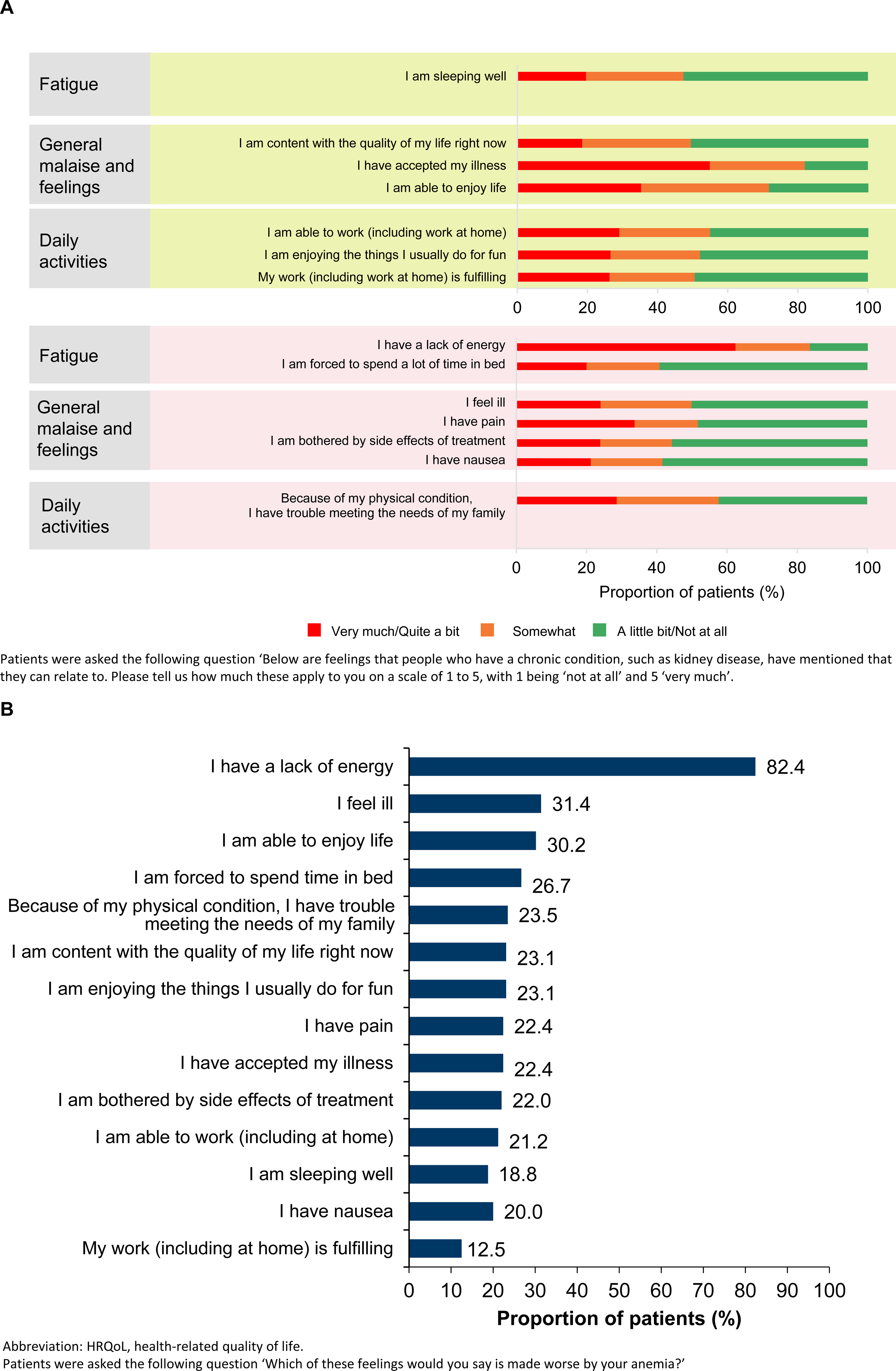
(A) Perception of chronic disease impact on HRQoL (anemia cohort, n = 255); (B) worsening of physical symptoms attributed to anemia by these patients.
Patients with anemia in CKD also reported an emotional impact (Supplemental Figure S2A). Approximately half of the patients in this group indicated that anemia increased their concern that their condition will worsen (Supplemental Figure S2B). The impact of anemia by CKD stage on emotional wellbeing is shown in Supplemental Figure S3A to E. Anemia and higher CKD stage was generally associated with greater proportions of patients feeling sad and/or depressed and that they are losing hope in the fight against the illness (Supplemental Figure S3F). Furthermore, anemia and higher CKD stage was generally associated with lower proportions of patients receiving emotional support from their family and feeling close to partners and friends (Supplemental Figure S3F).
Disease Awareness and Management
Overall, 27.8% of patients reported receiving treatment for both anemia and CKD. In the anemia cohort, 42.7% of patients reported receiving treatment for both anemia and CKD. While 52.4% of patients in the non-anemia cohort reported receiving treatment for CKD only, 7.9% reported also receiving treatment for anemia (Table 1).
Approximately two-thirds of patients with CKD reported always having their Hb levels assessed during regular check-ups (Supplemental Table S2). Of those with anemia, almost half reported always being asked about symptoms during regular check-ups, and approximately two-thirds were made aware of the relationship between anemia and CKD by the doctor who diagnosed them (Supplemental Table S2).
Patients in the anemia cohort reported discussing immediate symptoms and risks of anemia (e.g. weakness, headaches, or feeling tired [66.7%], and impact of anemia on daily life or activities [45.9%]) with their HCPs. Serious long-term risks, such as needing to go into hospital (25.5%) and heart disease risk (22.4%), were discussed less frequently.
Half the patients in the anemia cohort were informed by their HCP about treatment options for anemia versus 14% in the non-anemia cohort. In the anemia and non-anemia cohorts, 21% and 36% of patients, respectively, wanted to learn about treatment options for anemia (Supplemental Figure S4A). The majority (58.8%) of patients with anemia in CKD felt confident that they understood the side effects associated with anemia treatment, compared with 29.3% of patients in the non-anemia cohort.
Patients with anemia in CKD most commonly reported receiving treatment with iron supplements (54.5%) and dietary advice on managing their anemia (33.3%) (Supplemental Figure S4B).
Patient Perceptions on Anemia in CKD Care
Most patients with anemia in CKD felt that their anemia was either “well managed” (24.7%) or “very well managed” (42.7%; Supplemental Figure S5A). Patients with CKD stage 5 were least likely to perceive their anemia as “badly managed” (2.7%) or “very badly managed” (1.4%) and most likely to perceive their anemia as “well managed” (27.0%) or “very well managed” (56.8%; Supplemental Figure S5B). In addition, 48.2% of patients with anemia felt that conversations with doctors made them feel more knowledgeable about anemia (Supplemental Figure S5C).
Disease Information Sources
Common sources to look for information about anemia were HCPs, online sources, and social media (Supplemental Figure S6A). Approximately half of patients in the anemia and non-anemia cohorts looked to online sources to learn about anemia. HCPs, particularly specialists, were the most trusted source of information on anemia by both cohorts (Supplemental Figure S6B). However, 9.9% of patients with anemia in CKD indicated that the information received from HCPs and patient support groups was conflicting (Supplemental Table S3).
Of the patients with anemia, 44.7% relied on their doctor to monitor their anemia (Supplemental Figure S7). Patients with anemia felt that the worsening of their symptoms and daily life being affected would encourage them to seek more information or support about anemia (Supplemental Figure S8).
Overall, 38.1% of all patients with CKD and 43.9% of those who had anemia in CKD confirmed that they would like to receive more information and support about managing conditions like anemia.
Discussion
This study evaluated the experience and awareness of patients with anemia and self-reported CKD in the US, examining how they perceive the consequences and treatment of anemia.
The study findings highlight the challenges faced by patients with CKD and anemia in terms of disease awareness and impact on HRQoL. Many patients were unaware of the association between CKD and anemia, the diverse symptoms of anemia, and the different treatment options available. This lack of awareness may be attributable to the variability in anemia management amongst HCPs and support groups. This emphasizes a need for improved patient education through a patient-centered approach and consistent messaging across HCPs and other trusted sources, to ensure that patients have all the necessary knowledge required to successfully manage their condition.
Despite the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines recommending that all patients with anemia in CKD should have their Hb levels assessed regularly (12,17), only 50.3% of patients in this study indicated that their Hb levels were always assessed during regular check-ups. However, some patients may have been unaware of what is being assessed when blood samples are taken or that the frequency of Hb monitoring, regardless of CKD stage, is influenced by Hb level (ie, more frequent monitoring may be appropriate in patients with more severe anemia) and rate of decline in Hb level (17). This may also suggest that Hb assessments are not routinely performed, such as in CKD patients not on dialysis, for whom it is recommended that Hb levels are measured at least every 3 months (17). These findings highlight an opportunity for enhanced physician–patient communication regarding anemia management, given that patient knowledge of their Hb levels may be associated with HRQoL (18). In addition, studies have found associations between higher Hb levels and improved HRQoL in non-dialysis-dependent CKD patients (19).
Patients with CKD and anemia perceived that anemia had a negative effect on their physical symptoms and emotional wellbeing, and this effect increased for some components with higher CKD stage. Physical symptoms of CKD become more apparent as the condition progresses, including fatigue, sleep disturbance, feeling a lack of control, and depressive symptoms, similar to symptoms associated with anemia (9,20). Thus, patients with anemia could have been conflating CKD and anemia symptoms when surveyed. However, some patients reported aspects of their physical and emotional wellbeing as being made worse by their anaemia, including lack of energy and depression, suggesting an additional impact of anaemia on HRQoL and the patients’ awareness of this.
Previous studies have shown a detrimental impact of anemia in CKD on HRQoL (6,10). A review noted the adverse impact of anemia on energy/vitality and physical functioning in patients with CKD (21), supporting the findings from the present study. Evidence also suggests that increasing Hb levels can improve energy-related HRQoL scores (6); therefore, more routine measurement of Hb levels than is currently reported in this study and that are recommended by KDIGO guidelines (17) are essential in order to improve HRQoL. These improvements include increased physical activity, lower CKD progression, and greater survival rates (19).
Treatment options were discussed by HCPs for half of patients with CKD and anemia, and approximately 20% of patients were seeking more information, indicating an opportunity for further patient education to ensure all patients receive information about treatment options. Online information and HCPs were the most popular sources for information. However, regardless of anemia status, patients with CKD trusted their HCPs to a greater extent that all other information sources. The use of online sources may be reflective of the younger patient demographic for this survey (mean age 52.2 years), compared with the US CKD population as a whole (38% are aged 65 years or older) (3,22).
These findings suggest that there is an opportunity for increased dialogue between patients and HCPs, regarding the association between CKD and anaemia, its symptoms, treatment options and treatment effects. Such dialogue may enable patients to have better control over the management of their condition, allowing them to seek monitoring and guidance on treatment or alternative treatment options. Patients may also benefit from having a better understanding of the value of assessing their Hb levels, and take proactive measures in managing their condition. This approach is important in CKD management since slowing its progression, and hence improving HRQoL, must include patient involvement. In addition, our findings suggest that there is a need for more trustworthy and consistent online information to support patients in addition to discussions with HCPs, as some patients received conflicting information from HCPs and patient support groups. A recent systematic review reported that self-management support interventions (resulting in increased patient knowledge) were most frequently associated with statistically significant improvements in chronic disease management (23). Therefore, improved patient knowledge through more reliable information sources (such as awareness campaigns, patient advocacy groups, or patient-focused handouts, infographics or videos at General Practices) has the potential to improve HRQoL. However, the challenge will be how to provide this improved education to patients in a meaningful, engaging, and coherent manner.
The study had several limitations. According to the survey methodology and market research design, all patient information collected was anonymized and self-reported by patients, and therefore not confirmed by medical records. Thus, patients who reported that they had not discussed anemia symptoms or treatment options may have failed to recollect such discussions. Some patients with CKD in the non-anemia cohort reported receiving anemia treatment. This indicates an opportunity for HCPs to provide patients with more information and clarification regarding treatments. Furthermore, patients who responded to the online survey may be more engaged with, and knowledgeable about, their care than the general patient population, in addition to being better informed than those unfamiliar with technology and the internet. In addition, the demographics of the study are skewed towards advanced CKD. Therefore, this cohort may not be entirely representative of the CKD and anemia population as a whole, and may not provide a comprehensive picture of anemia treatment in the US. Finally, this was a cross-sectional study that used an unvalidated de-novo questionnaire in a limited sample size and did not include a longitudinal follow-up. While validated instruments to assess quality of life exist, they are not specific for assessing patient perspectives and experiences of the impact of anemia in CKD and, therefore, the objective of the present market research warranted development of a de-novo questionnaire.
Conclusion
These study findings emphasize gaps in the knowledge of disease awareness in patients with CKD and anemia, adding to the scarcity of patient-specific knowledge and experiences. It also reiterates the challenges faced by these patients, highlighting an opportunity for further patient education from HCPs and other trusted sources in the management of anemia, the importance of anemia monitoring, the symptoms of anemia, and available treatment options. This may aid the transition to a more patient-centered approach to treatment with potential to improve clinical care and patient-specific outcomes.
Supplemental Material
sj-doc-1-jpx-10.1177_23743735221092629 - Supplemental material for Understanding Patient Perspectives of the Impact of Anemia in Chronic Kidney Disease: A United States Patient Survey
Supplemental material, sj-doc-1-jpx-10.1177_23743735221092629 for Understanding Patient Perspectives of the Impact of Anemia in Chronic Kidney Disease: A United States Patient Survey by Susan Grandy, Eirini Palaka, Nicolas Guzman, Alicia Dunn, Eric T. Wittbrodt and Fredric O. Finkelstein in Journal of Patient Experience
Footnotes
Acknowledgments
We would like to thank the patients who participated in this study. Medical writing support was provided by Mahalia Gilmartin, PhD, and India Wright, MSc, and editorial support was provided by Rachael Cazaly, BSc, all of Core Medica, London, UK, supported by AstraZeneca according to Good Publication Practice guidelines (link). The sponsor was involved in the study design and collection, analysis, and interpretation of data, as well as data checking of information provided in the manuscript. However, ultimate responsibility for opinions, conclusions, and data interpretation lies with the authors. Development of this manuscript was supported by AstraZeneca.
Author Contributions
A. Dunn, S. Grandy, E. Palaka, and E.T. Wittbrodt contributed to the study design and data collection. E.T. Wittbrodt, E. Palaka, F.O. Finkelstein, N. Guzman, and S. Grandy performed the data analysis and interpretation. All authors critically reviewed the manuscript, approved the final version, and accept accountability for the overall work.
Data Sharing Statement
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E. Palaka, N. Guzman, A. Dunn, E.T. Wittbrodt, and S. Grandy are employees and stockholders of AstraZeneca. F.O. Finkelstein has received consultation fees from AstraZeneca, GlaxoSmithKline, and Akebia.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by AstraZeneca.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.