
Abstract
Patients with lower educational attainment are underrepresented in inflammatory bowel disease (IBD) research. To increase our understanding of the health care perspectives of patients with less than a university degree, semi-structured interviews were conducted among 23 outpatients at the McGill University Health Centre IBD Centre (Montreal, Canada). Thematic analysis was used to analyze the qualitative data. Perspectives focused on communication with health care professionals, access to care, symptoms and treatment, and outside support. Access to an IBD specialist was the most important aspect of care. Good care, kind and receptive staff, and a lengthy delay to diagnosis were frequently reported experiences. IBD specialists, nurses, and family and friends were most helpful in managing disease. Physical and emotional symptoms, reduced social engagement, and medications were difficult aspects of living with IBD. An ideal IBD clinic would provide access to traditional and non-traditional services and assist with obtaining support to help patients engage in social activities, increase affordability of care, and maintain employment. Study findings may be helpful in designing equitable models of health care delivery.
Introduction
Inflammatory Bowel Disease (IBD) describes diseases of chronic inflammation affecting the gastrointestinal tract. Approximately 270,000 Canadians are living with IBD (1). Given the chronic nature of IBD, patients interact with the health care system and health care professionals (HCPs) to receive care and treatment. Effective communication is essential to ensure high-quality care (2). However, the quality of physician-patient interactions is determined, in part, by the patient‘s level of educational attainment (3). Lower educational attainment may hinder a patient‘s ability to participate in clinical decision-making, ask questions or speak about health problems during appointments, increasing the risk for poor health outcomes (4).
Educational attainment is commonly used as a proxy for socioeconomic status (SES); it influences the selection of occupation and is stable beyond early adulthood and less influenced by adult-onset disease compared to income or occupation (5). In IBD, two literature reviews show associations between lower SES and lower health-related quality of life, and higher rates of hospitalization and mortality (6,7) compared to higher SES. Moreover, newly diagnosed IBD patients of lower SES are less likely to get the herpes zoster vaccine (8) compared to those of higher SES, possibly because the vaccine cost is not covered by provincial health insurance.
Level of educational attainment may influence participation in research. Some IBD studies conducted in Canada (9,10), the US (11–13), and Israel (14) show that individuals with less education had lower participation rates compared to those with more education. Whether due to having less flexible work hours, working multiple jobs, or having insufficient resources to cover costs of transportation or paid caregivers given the higher unemployment rates in high school compared to university graduates (15), disparities in health care will likely persist unless underrepresented patient groups contribute their views to research. The present study was undertaken to increase our understanding of the health care concerns of patients with IBD with less than a university degree who may be at risk for poor health outcomes. This study is an add-on to a larger pan-Canadian study aimed at increasing our understanding of what patients want from their IBD health care providers (HCPs) to improve the delivery of equitable high-quality care (16).
Methods
Semi-structured interviews were conducted among outpatients treated at the McGill University Inflammatory Bowel Disease Clinic in Montreal, Canada (July-August 2018). Purposive sampling was employed to recruit information-rich individuals with less than a university degree who were open to discussing their experiences with the health care system since receiving their IBD diagnosis. Eligibility criteria were aged 18 years or older, able to speak English or French, have a gastroenterologist-confirmed diagnosis of either UC or CD for at least one year, and have less than a university degree. Ethics approval was obtained from the McGill University Health Centre Research Ethics Board (REB#2018-4324) prior to study commencement.
A research assistant not involved in patient care explained to patients that we were recruiting those with less than a university degree to understand their thoughts and concerns about the health care they receive for IBD. A semi-structured interview guide was created for the purposes of this study (Table 1); the research assistant wrote participant responses directly on the form. Interviews were held in a semi-private area of the clinic and were 10-15 min in duration. Written informed consent was obtained from study participants prior to conducting the interviews.
Semi-Structured Interview Guide.

The semi-structured interview guide contained open- and closed-ended items to provide qualitative and quantitative data, respectively. Items addressed three broad dimensions of IBD care: (1) characteristics of HCPs and the health care system; (2) what HCPs do in delivering care, and (3) desired outcomes and goals. A ‘most-least‘ exercise provided insight into how individuals were making their selections on these dimensions of care.
Data Analysis
Thematic analysis, a flexible method to identify, analyze and report patterns in the data that is not tied to a specific theoretical perspective (17), was used to analyze the qualitative data. The qualitative analysis was data driven; reviewers identified themes and extracted supporting exemplars. Descriptive statistics were used to describe the study population and to quantify the number of participants endorsing different aspects of health care. This paper adheres to the Consolidated criteria for reporting qualitative research (COREQ) guidelines for reporting qualitative research (18).
Results
Twenty-five of 54 patients approached for study participation met eligibility criteria, of whom 23 (92.0%) consented to participate. Participants had a median age of 41 years and 12 (52.1%) were female (Table 2). Thirteen (56.5%) participants had CD, 6 (26.1%) had UC, and 4 (17.4%) had both. Participants had been diagnosed with IBD for a median of 9.0 years. Educational attainment level showed that 21 (91.3%) participants did not attend university and 2 (8.7%) attended without completion for reasons related to their IBD.
Characteristics of Patients with Inflammatory Bowel Disease with Less than a University Degree (N = 23).

Table 3 presents the qualitative data on participants’ responses to experiences since receiving the IBD diagnosis. Participants were instructed to focus on events that had occurred within the health care system and with HCPs; what were the most difficult aspects of living with IBD; and what would help them better manage their IBD. In general, participants considered high-quality care as good care, getting appropriate referrals and easy accessibility, and low-quality care as lengthy delays until diagnosis, encountering non-receptive staff, having to access the private health care system to obtain care, poor accessibility, and getting inappropriate referrals. Four themes emerged from these data including communication with HCPs, access to care, symptoms and treatment, and outside support.
Responses to Open-Ended Questionnaire Items on Patient Experiences Since Receiving the Diagnosis of Inflammatory Bowel Disease (IBD) (N = 23).

Responses exceed the number of participants (n = 23) as they were permitted to discuss more than one subject per question.
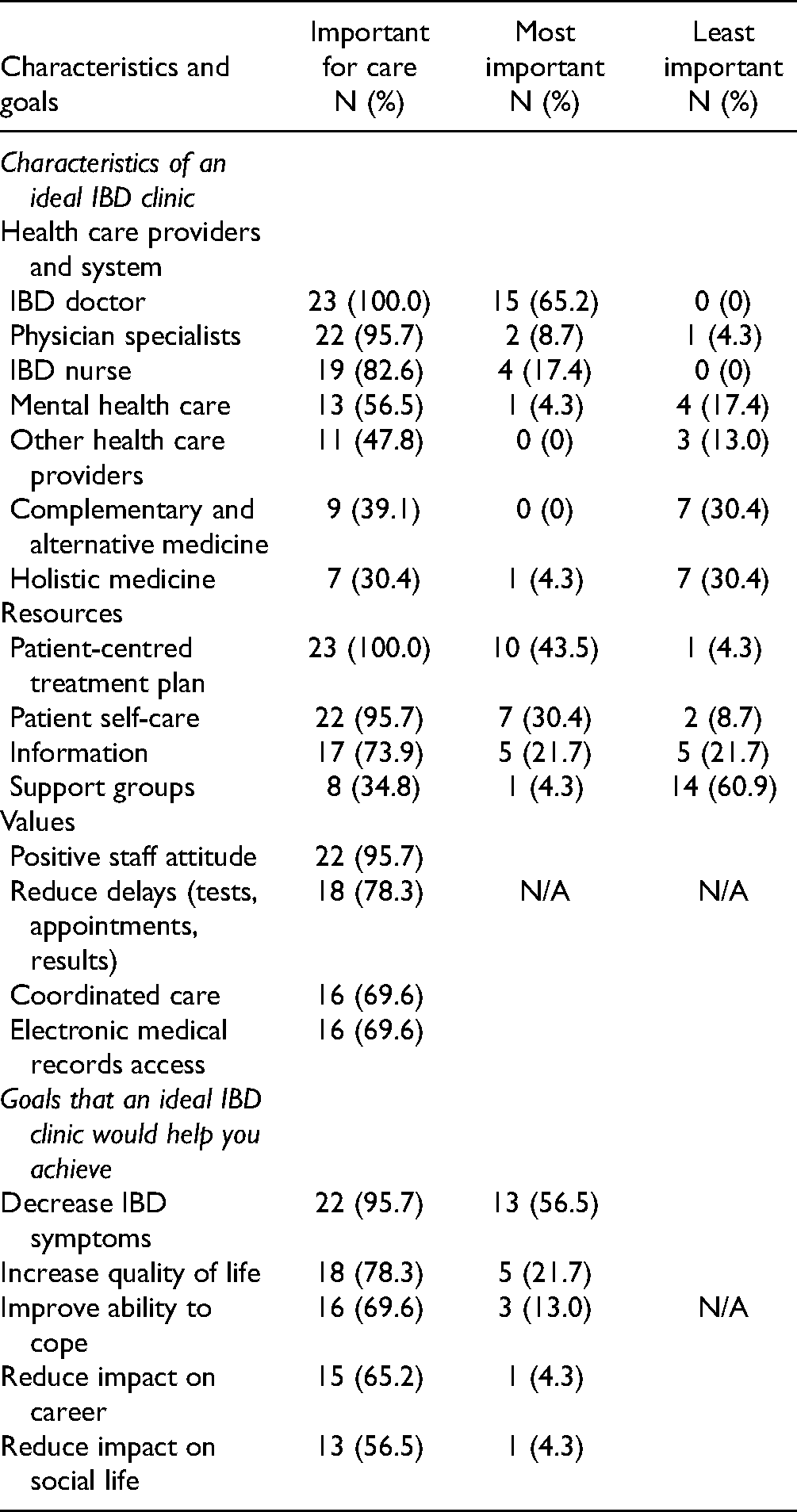
Table 4 presents responses to the quantitative questionnaire items on the characteristics of an ideal IBD clinic and the goals such a clinic would help patients achieve. Both Tables 3 and 4 will be discussed according to the four identified themes.
Characteristics and Goals of an Ideal Inflammatory Bowel Disease (IBD) Clinic (N = 23).
Communication with HCPs
Interactions with physicians and nurses were strong factors of satisfaction and dissatisfaction with care. Participants considered their IBD doctor and IBD nurses as most helpful to managing IBD (Table 3), particularly those who were knowledgeable, kind and receptive. “The IBD specialist I have now is really kind, responsive and present.”
“The IBD nurses are great intermediates between the patients and the doctors.”
Several participants valued all aspects of the care they had received and did not consider any least helpful. However, not all HCPs understood patient information needs or were sufficiently informed about IBD themselves. Experiences with non-receptive physicians and nurses were considered least helpful, and among the most difficult aspects of living with IBD. “I want more physicians to understand IBD and listen to their patients. I was quarantined for three days during a flare because the ER staff thought I had a contagious virus despite informing them I had Crohn‘s Disease.”
Poor communication had occurred with gastroenterologists, family physicians and other specialists. Participants reported experiencing delays with testing, appointments and diagnosis, as well as poor coordination of care and being misdiagnosed. “The most challenging experience was having to wait eight years to be referred to the IBD clinic. (My) gastroenterologist would wait a year and a half to see if each medication would work despite me telling him they were not working.”
“I was sent home three times, at three separate hospitals being diagnosed with gastro.”
Table 4 shows that nearly all participants valued the clinic staff‘s positive attitudes as an important aspect of their care. Eighteen (78.3%) participants felt that reducing delays for appointments, tests and test results was important for their care. Sixteen (69.6%) participants valued each of coordinated care and having access to electronic medical records.
Access to Care
Access to care was a concern to patients with lower educational attainment. Poor access to physician specialists and nurses was considered least helpful, while distance to the clinic was considered the most difficult aspect of living with IBD (Table 3). “It‘s difficult having to travel every three to four months … for appointments and tests. I wish it could be treated more locally.”
Some participants wanted access to mental health care and holistic therapies to help them better manage their IBD. “I wish the doctors were more receptive about giving holistic medicine and lifestyle interventions, such as diet, a chance rather than constantly pushing drugs chronically. I wish Western medicine, nutrition and holistic medicine could be integrated and provided by the treating physician. This would provide safety when trying lifestyle modifications to help manage my IBD.”
Providing access to telehealth care was another way to help participants better manage disease especially during flares when teleconsultation could provide immediate care. “I could better manage my IBD if I was able to call the IBD clinic directly and have my questions answered immediately.”
Participants considered access to a broad range of HCPs important to their care in an ideal IBD clinic (Table 4). Access to an IBD doctor was important to all participants, with 15 (65.2%) selecting it as the most important aspect of care. Twenty-two (95.7%) felt access to other physician specialists was important, 2 (8.7%) of whom selected it as the most important aspect of care. Access to an IBD nurse was important to 19 (82.6%) participants, with 5 (21.2%) selecting it as the most important option. Eight (34.8%) and 9 (39.1%) participants considered holistic, and complementary and alternative medicine important services, respectively, although these were considered least important to 7 (30.4%) and 7 (30.4%), respectively.
Symptoms and Treatment
Participants had concerns about symptoms and treatment. Physical and emotional symptoms as well as medications including side effects and injectable administration were among the most difficult aspects of living with IBD (Table 3). Treatment that reduces symptoms was most helpful in managing IBD, and better treatments and technologies would help patients better manage their IBD. “Better treatment. Nothing else would help unless symptoms are controlled.”
Table 4 shows that all participants endorsed having a patient-centred treatment plan important to the care delivered in an ideal IBD clinic, 10 (43.5%) selecting it as the most important aspect of care delivery. Patient self-care was important to 22 (95.7%) participants, with 7 (30.4%) selecting it as most important. Eight (34.8%) participants felt that support groups for themselves and their families were important, but 14 (60.9%) selected this item as least important. Nearly all (95.7%) participants considered reducing symptoms an important care goal, with 13 (56.5%) selecting it as most important.
Outside Support
Outside support was discussed for its contributions and challenges. Participants indicated that support from family and friends and other patients was most helpful to managing their IBD (Table 3). “My mom helped me at the beginning when I was in severe pain and didn‘t know what was going on. She brought me home and took care of me.”
“Meeting with others who suffer from the same disease is helpful. It helps to discuss and engage about the diseases.”
In contrast, the lack of government recognition and financial assistance was least helpful in managing IBD. Participants acknowledged the difficulty of accessing public washrooms and wanted government-issued Crohn‘s and Colitis Canada washroom access cards that would be legally binding and enforceable. They also wanted the government to cover the full cost of medications to improve the affordability of treatment.
“The government does not recognize IBD as a disability. This could help with transport and access to washrooms. They should create a card that would be issued by the doctor and government that would allow IBD patients to access handicap and private washrooms such as in subways and private businesses.”
“Medications are extremely expensive and not fully covered by the RAMQ. It can cost thousands of dollars.”
The impact of IBD on careers was among the most difficult aspects of living with the disease. Better informed employers might facilitate the implementation of workplace accommodations to allow individuals with IBD maintain employment. “Employers don‘t know about the disease and therefore think you‘re slacking off. I wish they understood the disease better.”
Reducing the cost of hospital parking was another way that outside support would help patients better manage their disease. Not only might the high cost of parking deter patients from seeking health care, but patients might be hardest hit by parking costs during flares when they are also absent from work.
“Make parking free or cheaper. You have to be rich to afford it”
Further endorsement for outside support is presented under goals of care (Table 4). For the majority of participants, an ideal clinic would help them reduce the impact of IBD on both their careers and social lives. Achieving these goals would allow them to maintain employment and engagement in social activities.
Discussion
This study sought to improve our understanding of the experiences with, concerns for, and goals for health care of IBD patients with less than a university degree who may be at risk for poor health outcomes. Participants were most concerned about communication with HCPs, access to care, symptoms and treatment, and outside support. The age diversity of participants represents various experiences and perspectives that allowed identification of common patterns as well as differences. Patients and physicians clearly differ in their perspectives of what constitutes high-quality care (19).
Comparison to Other Studies
Participants considered kind and receptive HCPs essential to high-quality care that includes family and ED physicians who are often the first HCPs to interact with newly ill patients, as well as IBD specialists. Encountering nonreceptive HCPs mirrors the findings of others that showed more than half of patients are unable to tell their physicians important details about their IBD and believe their gastroenterologist should ask probing questions to better understand the impact of IBD on their quality of life (20). Study participants wanted all HCPs to have a thorough understanding of the clinical presentations of IBD to facilitate delivery of appropriate and timely care to prevent lengthy delays to diagnosis, which can lead to poor outcomes including increased risk of intestinal surgery (21). However, an in-depth understanding of IBD by primary care and ED physicians may not be practical as these physicians infrequently encounter IBD patients in clinical practice. Moreover, diagnosis in these settings is challenging, as patients tend to initially present with non-specific symptoms (i.e. gastrointestinal bleeding, abdominal pain, changes in bowel patterns), which explains, in part, the median time to diagnosis for UC and CD of 4 and 9 months, respectively (22).
Participants wanted access to efficient, high-quality multidisciplinary care that included mental health care and non-traditional therapies. However, management of IBD can be fragmented across health care systems and HCPs (23). IBD patients have higher rates of anxiety and depression compared to the general population (2), and which are higher in those of lower compared to higher SES backgrounds (24,25). Providing access to preferred therapies should be a treatment option since anxiety and stress contribute to disease exacerbation (26).
Managing symptoms was considered the most difficult aspect of living with IBD, while better and more effective treatments were considered most helpful. Medication in IBD is life-long and problematic owing to severe side effects or difficulties with injectable administration (9). Nevertheless, patients prioritize symptom relief over both the frequency and route of medication administration (27), which explains the finding that almost half of IBD patients experience medication side effects despite concerns about long-term effects (20). Some participants believed that non-traditional therapies were important to their care and wanted their physicians to know more about diet and lifestyle interventions that could potentially act as first line therapies for managing IBD. Non-traditional therapies recommended or provided by the treating physician would increase patient confidence in their safety.
Outside support from government and employers was thought to help patients overcome financial, social and occupational challenges. Lower income patients may lack private health insurance or the ability to afford medical costs on their own, and full government coverage for medication would relieve them from having to pay the difference. Reducing the out-of-pocket cost of parking to attend medical or treatment visits, which might be compounded by unpaid absence from work (28,29), would also improve the affordability of care. Government-issued public washroom access cards would reassure patients that their basic hygiene needs are met when they leave home and increase their participation in social activities. Workplace accommodations to permit frequent bathroom access might occur if employers were sufficiently knowledgeable about IBD, which, in turn, would enhance patients’ ability to remain at work (2).
Similarities and differences were noted in comparing findings of the present study to those of our larger study (16). Similar findings included the barriers to receiving adequate care such as delayed diagnosis, long wait times for appointments, geographical and physical accessibility barriers, and physicians having insufficient knowledge of IBD, as well as inclusion of services provided by an ideal IBD clinic such as mental health support and non-traditional therapies. Differences in findings showed that participants in the larger study wanted better care coordination including gate keepers and care coordinators, a patient portal or app with direct access to medical records, specialized care, and improved communication between providers, patients and family members. In comparison, participants in the present study wanted support from outside sources to lessen the social, occupational and financial impacts of IBD. Whereas participants in both studies expressed the need for greater access to multidisciplinary services, those with lower educational attainment also wanted system changes that increased their abilities to remain at work and engage in social activities, and that reduced out-of-pocket expenditures.
Limitations
Participants did not represent all patients of lower educational attainment, a limitation common to all qualitative research. Findings may not reflect the perspectives of patients with a university degree or higher, those who do not speak English or French, or those seen in non-specialized IBD clinics. Assessment of place of residence and income/occupation would have enhanced our understanding of whether participants lived far from the clinic and were of low SES, respectively.
Conclusion
Health care perspectives of IBD specialty clinic patients with less than a university degree focused on communication with HCPs, access to care, symptoms and treatments, and outside support. Highly valued were receptive, kind and knowledgeable HCPs; access to multidisciplinary HCPs and services; effective treatments; and outside support to help individuals maintain employment and social engagement and improve the affordability of health care. Findings underscore the importance of understanding the health care perspectives of IBD patients with lower educational attainment when designing models of health care delivery.
Footnotes
Acknowledgments
The authors thank the McGill University Health Centre IBD Clinic patients who participated in this study. DAM is supported by the Arthur J.E. Child Chair in Rheumatology and a Canada Research Chair in Health Systems and Services Research (2008-2018).
Authors’ Contributions
Study concept and design: EH, MJS. Acquisition of data: EH. Biostatistical programming: EH and MJS. Analysis and interpretation of data: all authors. Drafting of the manuscript: EH, MEB, MJS. Critical revision of the manuscript for important intellectual content: all authors. Obtained funding: EH and MJS.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ferring, (grant number Ferring Scholarship Grant Award [2018] ).