
Abstract
Keywords
Introduction
Waiting time is a significant indicator of healthcare use and it is commonly assessed between the patient's arrival at the clinic and the start of the specified services at various stations within the clinic (1). The overall visit time is the period beginning with the patient's entering the hospital to the end of the last clinic activity during the visit (2). While acceptable waiting times for specified services are not explicitly stated in many health systems, strategies to reduce waiting times and improve efficiency in patient flow management are critical goals in healthcare delivery. To achieve this, it is imperative to identify the variables that affect the length of time spent waiting and the satisfaction of patients with time spent in a quest to reduce waiting time and improve patients’ satisfaction (3).
Patients’ satisfaction with the quality of healthcare is an indication of the extent to which the patients accept that their needs are being met by the service. Satisfaction is commonly conceptualized using theoretical models such as the “value expectancy model,” “fulfillment model,” and the “discrepancy model” (4). As a latent construct, it indicates how clients’ experiences relate with their a priori expectations on the structure, process, or outcome of care. Satisfaction is enhanced when needs and desires on waiting times and various processes encountered while seeking medical treatment are met (5).
Patients’ satisfaction directly affects compliance with their treatment regimen and ultimately, their wellbeing. Satisfied patients are likely to maintain contact with their health care providers for follow-up or episodic care. As satisfaction is connected to consistency, adherence to treatment, and better healthcare results so is dissatisfaction associated with poor adherence to treatment guidelines and poor health outcomes (6,7).
Universal healthcare coverage (UHC) is premised on all individuals having access to a full range of promotive, preventative, curative, rehabilitative, and palliative healthcare services they need without facing a financial hardship (8). The attainment of UHC is viewed as one of all people's basic human rights regardless of their faith, color, social or economic status, and political convictions. Such attainment requires effective national healthcare frameworks and healthcare financing instruments that guarantee not only financial risk protection particularly for the poor (9), but could enhance patients’ experience of healthcare services.
Achieving UHC remains a herculean task in many developing countries, where large populations make out-of-pocket (OOP) payments at the point of access to needed health services. This bane of many local systems in developing countries like Nigeria is consequent on the limited coverage of pre-payment schemes or publicly financed access to healthcare. The preponderance of OOP has become a critical impediment to health care coverage and there is an emerging consensus that this practice should be eliminated as a means of achieving access, equity, and quality healthcare delivery in these systems (10).
Although satisfaction is understood differently by various stakeholders in healthcare, constructing satisfaction through the lenses of patients who are directly affected by the processes during the delivery of medical care is fundamental (11). Critical concerns with patients’ satisfaction and healthcare quality include long waiting time, the attitude of care providers towards patients, and unfulfilled consultation with the doctors (2,5)
Besides the reported impact of insurance status on access to healthcare, the value of time makes it imperative to measure and improve efficiency in patient flow management to guarantee continuing patronage of available services. One recommendation is that 90% of outpatients receive attention within half an hour of their appointment time (12). This goal is yet to be achieved in many developing countries where patients are reported to spend long waiting time in outpatient clinics (2,12). Insured patients may also experience long waiting time like their uninsured counterparts partly due to system constraints (13).
While previous studies captured patients’ satisfaction and/or waiting time as standalone interest and the possible relationship between patient satisfaction and waiting time (2,14–16), this study investigated how the insurance status of the patient affects waiting time and patients’ satisfaction with time spent at various service stations during visits to the general outpatient clinics in a tertiary hospital in Nigeria.
Methodology
Study Design
The study is a comparative longitudinal study that involves recruitment and follow-up of insured and uninsured patients through to consultation at the general outpatient clinic.
Study Setting
This study was carried out in the Family Medicine Department which hosts the General Outpatient Clinics (GOPC) of the University of Port Harcourt Teaching Hospital (UPTH). UPTH is one of 2 tertiary teaching hospitals in Rivers State, Southern part of Nigeria. The Family Medicine Department runs outpatient clinics at 2 separate locations for insured and uninsured patients. Insured patients are principals and 4 dependents covered under the National Health Insurance Scheme (NHIS). These clinics largely utilize paper-based patient records where first-time or repeat patients are required to first visit the medical records department to either open a new folder or recover their existing folders which are sent to the outpatient clinics by clerical officers. The general out-patients’ clinics for the uninsured sees an average of 120 patients daily, with 6 attending doctors, about 7 nurses, and 6 medical records personnel while the section for the insured (nicknamed ‘NHIS clinic’) sees an average of 70 patients daily, with 4 attending physicians, 3 nurses, and 4 medical records personnel.
After dealing with the medical record officers, patients are allotted serial numbers by the nurses in the order they arrive at the clinic and attended to on a first-come, first-serve basis. Nurses at the GOPC receptions deliver group health talks and checked the vital signs of the patients who maintain their queue while waiting for consultations with the doctors. Subsequent activities after consulting the doctor are dictated by the recommendations of the consulting doctor (Figure 1).

Pathway for insured and uninsured ambulatory general outpatients.
Subject Selection
All ambulatory adult patients seeking health care at the general outpatient clinic and those at the NHIS clinic were eligible if they gave consent, were not critically ill, and were not staff of the hospital. A systematic sampling approach was used to select 332 patients from the population of the insured and uninsured who were present at the medical record by 8 am on each day of data collection groups.
Sample Size
The minimum sample size of 332 was calculated using the formula below which is suitable for a comparative design showing the difference in proportion (17).

Data Collection
Data was collected over a period of 3 weeks, starting from November 16, 2020, to December 5, 2020. Each study participant was given a structured record sheet to enter the time they arrived and leave each of the service stations and provide feedback on their level of satisfaction with the time spent at each service station. Tracking was limited to the outpatient consultation aspect of the visit and did not extend to other critical stations, for example, pharmacy, referral for laboratory investigations, or specialist attention that followed recommendations after consultations with the doctors. The outcome variables were time spent and the level of satisfaction of insured and uninsured patients with the duration of time spent at each station. Both the idle (waste) time and the period of engagement with the caregivers (effective time) at these stations were measured and reported. A structured questionnaire and record sheets had 3 sections—Section A was designed to obtain the socio-demographic data of the respondents. Section B captured the clock in and clock out time at each station the participants received care, while Section C was designed to assess their satisfaction with the time spent at each service section. Time spent moving from one station to another (motion waste) or spent in other discretionary activities during their visit were not captured by the participants. The waiting times were operationalized as follows:
Waiting (idle) time at each station—from the point of arrival at the service station to the time of initiation of the intended service at that station. Effective time at each station—time spent receiving attention from health workers at each station. Total time spent—the time of arrival at the hospital to the conclusion of patients’ activities at the hospital. Total effective time—duration of time spent meaningfully engaging with the health workers at the various service stations. Total idle time—cumulative duration of time spent waiting for attention to be provided by the health workers at all service stations. Percentage wasted time—the percentage of overall time spent outside actual engagement with the health workers. Time efficiency for index visit—the percentage of total time spent engaging with health providers. It is calculated as:
The feedback on patient satisfaction with the various time spent was rated on a 5-point response scale (1 = highly dissatisfied, 2 = dissatisfied, 3 = indifferent, 4 = satisfied, and 5 = very satisfied).
Data Analysis
The data were analyzed using IBM's Statistical Package for the Social Sciences Version 20.0 (19). Chi-square test was used to determine if differences exist in the background characteristics of study participants; independent t-test and un-standardized estimates of mean differences in time spent. Spearman's ranked correlation was used to assess the relationship between time spent and patients’ satisfaction with time spent at each service point. Both point and interval estimates were computed and P-values of ≤.05 were regarded as significant.
Ethical Consideration
Participation in this study was voluntary and informed consent was obtained from the participants after assurances of confidentially. Participants were also informed that they could leave the study at any point without jeopardizing their care in the hospital.
Ethical clearance was also obtained from the Ethics Committee of the University of Port-Harcourt and the University of Port Harcourt Teaching Hospital's ethics review committees. Authorization was also obtained from the head of the Family Medicine Department of UPTH.
Results
The response rate was 100% and Cronbach's alpha for insured satisfaction with time spent was 0.63 while that for uninsured patients was 0.23. Table 1 presents comparative data on the socio-demographic characteristics of respondents. Most respondents in both groups were aged between 30 and 60 years. While a higher proportion of the insured respondents were males (54.8%), the uninsured group had more females (53.0%). A significantly higher proportion of the insured had attained a post-secondary level of schooling (P < .001), employed (P < .001), and repeat visitors (P = .003).
Socio-Demographic Characteristics of Respondent.

*Statistically significant (P < .05).
Table 2 presents the analysis of time spent by insured and uninsured patients using the mean difference. Idle time before seeing a nurse was significantly higher for the uninsured category (md: 74.5 min; 95% CI: 69.8–79.3 min). Significantly higher idle time before consultation with the doctor was also observed among the uninsured group (P < .001). While the effective time spent receiving nursing attention was significantly higher among the insured group (P < .001), there was no significant difference in the time spent in consultations with the doctors (P = .107). Total time spent on the visit was lower for the insured (106.6, 95% CI: 102.6, 110.6) compared to the uninsured (204.8, 95% CI: 197.8, 211.8), and this difference was statistically significant (P < .001). Over three-quarter of the time spent by uninsured patients were spent outside one-on-one engagement with providers at each of the relevant service stations and there was an observed 17.4% (95% CI: 15.6, 19.2%) higher percentage of time wasted among the uninsured which was statistically significant (P< .001).
Comparing Time Spent by Insured and Uninsured Patients.

*Statistically significant (P < .05).
Table 3 shows the relationship between time spent and the insured/uninsured patients’ satisfaction with time spent at the various service points. There were mostly consistent and inverse relationships between these variables. These relationships were statistically significant in both categories for time spent at the registration point, for an idle time before nursing attention, and idle time before consultation with the doctors (P < .001). A weak significantly inverse relationship was observed for consultations with the doctors among insured patients (r = −0.16; 95% CI: −0.32, 0.01; P = .036), the converse was observed for the uninsured category (r = 0.15; 95% CI: −0.01, 0.35; P = .049).
Relationship Between Time Spent and Patient Satisfaction With Timing at Service Stations.
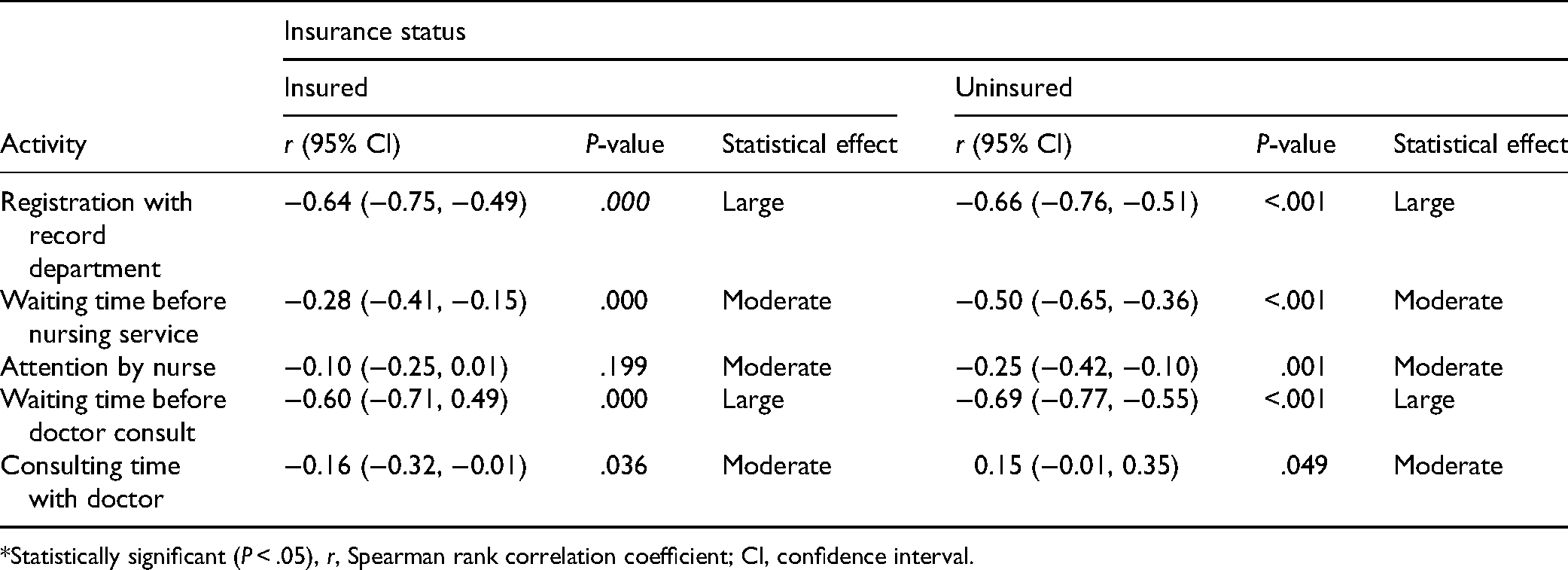
*Statistically significant (P < .05), r, Spearman rank correlation coefficient; CI, confidence interval.
Discussion
This study compared the waiting time and satisfaction with waiting time among insured and uninsured patients seeking general outpatient care in the University of Port-Harcourt Teaching hospital.
Although many patients arrive early to the hospital, departures occur at a rather stable rate from the commencement of consultation leaving those who arrived early spending longer time in the hospital. This observation, which is consistent with previous studies (2,20), typifies one of the untoward effects of late commencement of clinical activities in public hospitals and its attendant consequences on patient flow management, economic losses, and patient experiences (21). Even where the medical record officers arrive early, the flow of patients to specialist clinics are affected where gatekeepers in the general outpatient clinics are not available to discharge their clinical duties.
The finding of more male patients in the insured category corroborates findings from an earlier study and might depict the selective enrolment into the social health insurance scheme of those who are economically advantaged, working in the formal sector or have the means to pay the premium—a situation that favors the male population in this setting (18,22,23). Similar higher proportion of enrolled patients in the age range of 30 to 60 years connotes the economically productive segment of the population and reinforces the skewed health coverage in this setting. The majority of these enrollees are federal public servants who are mandatorily enrolled into the scheme with premium deducted from the source (24,25).
An uninsured patient spends on average, 92.2 (95% CI: 90.2, 106.2) minutes more time from the point of arrival in the records department to the end of the consultation with the doctors. The uninsured patients are required to make an out-of-pocket payment at the various revenue collection points after each request by the health workers. The longer duration of time spent by the uninsured patients corroborates finding from previous research (2) and suggests an advantage for insured patients. Aside from the insurance status of the patients, the differential caseload and bureaucracies in patient flow management in the 2 clinics may also be contributory to the longer duration of time spent at the section for the uninsured (18). With equity still an important driver of healthcare reforms, it will be desirable to estimate the direct and indirect costs of this dismal disparity in time spent by patients seeking outpatient services. Findings from such assessment can provide evidence-based for strengthening strategies for scaling up enrolment into the social insurance scheme.
A further elaboration on the above scenario is the finding of over three-quarters of time spent by insured patients and about two-thirds of the time spent by insured patients as wasted. While a longer duration of time was spent waiting for consultation with the doctors among the insured patients, more time was spent waiting for attention by nurses among the uninsured categories. The time wastages give an indication of the value that focused interventions for improving patient flow management will yield for insured and uninsured patients.
Improving efficiency in patient flow management for insured and uninsured patients will require a system approach that scrutinizes the inputs and processes in health care delivery. For an outpatient clinic, this will require creating a healthy work culture and adherence to operating times. The punctuality of health workers needs to be addressed as the different categories of health workers are known to commence their daily duties at different times in contravention of the public service requirements (22). Feasible technical options of improving efficiency in patient flow management and reducing time wasted include the introduction of the patient appointment system and physician scheduling, active monitoring of demand and supply of outpatient services, improving personnel management in public health institutions, patient empowerment, task shifting, strengthening extant regulations, and exploring legislative approaches to managing waiting time in public health institutions (2,26).
It is not surprising that insured patients showed significantly higher levels of satisfaction with the nursing and doctor's idle times. This study also demonstrated a consistent inverse relationship between the duration of time spent and the patients’ satisfaction with the time spent. The corroboration of a higher level of satisfaction with time spent among insured patients (24,27,28), may have been the result of staff humanness, deployment of technology in managing patient information, and the absence of frustration experienced by uninsured at various payment portals in the hospital.
Results showed a statistically significant association between waiting times patients’ satisfaction with time spent at each service station. Significantly higher levels of satisfaction with time spent at the stations were reported among the insured patients. Plausible reasons adduced for this were better workflow, fewer workloads, and stricter third-party supervision in the NHIS clinic. The obverse report of uninsured patients being more satisfied with the quality of care (28) and time spent was adduced to the cash-backed nature of the dealings with providers who are incentivized by tokens from patients who are in turn, readily given prompt and better attention by health workers (29,30).
While finding from this study showed that a reduction in the overall waiting time was associated with a significant increase in the level of satisfaction for both the insured and uninsured patients, a previous study conducted at a teaching hospital in North-eastern Nigeria had reported no significant difference in satisfaction between insured and uninsured patients (28). Apart from the duration of time patients spend at the station, the level of constructive engagements while waiting may also predict the psychological impacts on patients. While idle times often appear longer and more frustrating than times spent while being engaged, waiting times in hospital is more complex than commonly conceptualized linear construct based on an assumption that patients become more distressed the longer they wait. Waiting can be irritating, frustrating and a source of great uncertainty (1). However, patients’ experiences while waiting for elective care are complex, subjective, and often constitute serious barriers to efficient patient flows in many health systems (13).
Distractions or meaningful engagement of patients while waiting can improve patients’ experiences of healthcare. Such engagement is achieved when hospitals provide newspapers, magazines, free Wi-Fi, and audio-visual entertainment. Evidence suggests that such constructive distractions can reduce the negative psychological impact related to stress, anxiety, frustrations, etc associated with waiting (21).
The time patients spent during outpatient visits help to shape their overall experience and has a powerful effect on their satisfaction. It also directly affects their economic and psychological well-being. Improving the comfort at the receptions where patients wait by ensuring conducive ambient temperature, provision of complimentary tea/coffee, etc could reduce these negative impacts of prolonged waiting times.
Transitioning to technologically driven healthcare processes including the introduction of electronic health records (EHR), mobile queue, telehealth patient appointment system, or providing a callback option for patients who speculate they may wait too long is evidenced-based cost-effective strategies that can be deployed in healthcare delivery in developing countries. Favorable situational factors for the deployment of technology include the high internet/mobile penetrations and the support of key stakeholders including patients and providers (23,31).
Similarly, task-shifting approaches can be redeployed to reduce the idle time before engagement with nurses and doctors especially in a setting with a skewed provider–patient ratio. This strategy should not, however, replace stricter administrative measures to ensure staff punctuality, discipline, a regular survey of bottlenecks, or enabling providers to have access to patients’ information before the scheduled appointments. In all, improving efficiency in patient flow management is recommended in public health facilities in Nigeria.
Strengths and Limitations of the Study
This study derived its strength from the rigorous methods deployed in the measurement of patient waiting time and patient satisfaction with the waiting time at the various service stations. The strength was also enhanced by the granularity of the data, the representativeness of the population included in the sample, and the high response rate with the support of the research assistants.
Notable limitations of the findings of this study include the limitation of tracking of the patients to consultation within the outpatient clinic. As such essential encounters with other services stations that would define total time spent on the visit were not achieved. The low internal consistency reliability of the instrument used to measure satisfaction with time spent was also of concern. Furthermore, the study did not capture the possible influence of staff, patients’ characteristics, and organizational processes on waiting for time and patients’ satisfaction. Nonetheless, the findings vividly demonstrated the flow of insured and uninsured outpatients in a tertiary health facility in a developing country.
Conclusion
Significant variations exist in the time spent and satisfaction with time spent by insured and uninsured ambulatory patients attending the outpatient clinics at the University of Port-Harcourt Teaching Hospital. As the waiting time is inversely related to level of patients’ satisfaction, innovation to reduce patient waiting time should be pursued to improve patient experiences as well as their economic and psychological wellbeing.
Footnotes
Acknowledgments
Our profound gratitude goes to Felix Anyim for your assistance during the data collection and interpretation. The efforts of the medical record staff in identifying insured and uninsured patients who visited the hospital for general outpatient care are highly appreciated. Finally, we appreciate all the patients who participated in this study for their calm responses and cooperation.
Authors’ Contributions
Ethical Consideration
Ethical clearance was obtained from the Ethics Committee of the University of Port-Harcourt (ref: UPH/CEREMAD/REC/MM72/064, dated January 28, 2021) and the University of Port Harcourt Teaching Hospital's ethics review committees (ref: UPTH/ADM/90/S.II/VOL II/1028, dated November 12, 2020). Authorization was also obtained from the head of the Family Medicine Department of UPTH.
Consent
The participation of patients in this study was voluntary and informed consent was obtained from the participants after assurance of confidentially and minimal disruption of receipt of care was given by the research team. Patients were also informed that they could leave the study at any point without jeopardizing their care in the hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
The participation of patients in this study was voluntary and informed consent was obtained from the participants after assurance of confidentially. Patients were also informed that they could leave the study at any point without jeopardizing their care in the hospital.