
Abstract
Despite a wealth of research regarding COVID-19, little evidence exists about cancer patients’ specific needs and experiences at end-of-life. This study retrospectively describes the care of 34 hospitalised cancer patients dying with COVID-19. The palliative care needs of patients were described. The main domains of end-of-life care service provision were evaluated including treatment of pain and other symptoms, communication and decision making at end-of-life and level of involvement of the palliative care team. Physical symptoms were managed with relatively low doses of end-of-life medications. High levels of patient and family anxiety, however, highlight the complexity of death from a stigmatised disease. Prompt acknowledgement of the vulnerability of advanced cancer patients with COVID-19 can facilitate proactive symptom management, anticipatory communication and enhance family support.
Keywords
Introduction
Since the outbreak of the pandemic severe acute respiratory syndrome-coronavirus-2 (COVID-19), there has been much research on the features and outcomes of this disease. Large multicentre studies have examined the implications of a cancer diagnosis and systemic anti-cancer therapy (SACT) on COVID-19 mortality and found no increased mortality in patients who had received SACT within 4 weeks of COVID-19 infection (1,2). Advanced disease, poor performance status, and comorbidities have been associated with higher mortality, as well as male gender, increased age, smoking, and cardiovascular disease (3). The pandemic is expected to have a protracted effect on cancer service provision, with an estimated 45,000 late cancer diagnoses in the UK after the first year (4,5). Work reviewing the experience of bereaved family members during the pandemic identified worsened psychological wellbeing in the context of social isolation, communication challenges and hospital visiting restrictions (6–8). Small studies conducted in the UK described the end-of-life symptoms of patients with COVID-19 (9,10). However, <25% of the patients included in these studies had cancer and there is little published data about cancer patients’ specific needs and experiences at end-of-life during the pandemic. As the pandemic enters its second year, with additional COVID-19 variants emerging, and as countries face new waves of infection, preparation and planning for end-of-life care provision for cancer patients remain a priority.
Aim
The aim of this study was to describe the care of hospitalised cancer patients dying with COVID-19, to illustrate in part, these patients’ experiences at the end-of-life.
Methods
Study Design and Setting
A retrospective study of cancer patients who died at a tertiary referral cancer centre with COVID-19 during the peak periods of the pandemic.
This study was approved as a service evaluation by the local Committee for Clinical Research, approval number SE948.
Sampling
All non-ventilated inpatients aged over 18 years who died with either a confirmed reverse transcription polymerase chain reaction (PCR) diagnosis of COVID-19 or strong clinical suspicion of COVID-19 during the first two waves of the COVID-19 pandemic were included in the study. The study time period spanned from 25 March 2020 to 1 May 2020 (wave 1) and from 5 December 2020 to 1 March 2021 (wave 2), corresponding to the first COVID-19 positive death at the cancer centre during the surge periods of cases in the UK.
Data Collection and Analysis
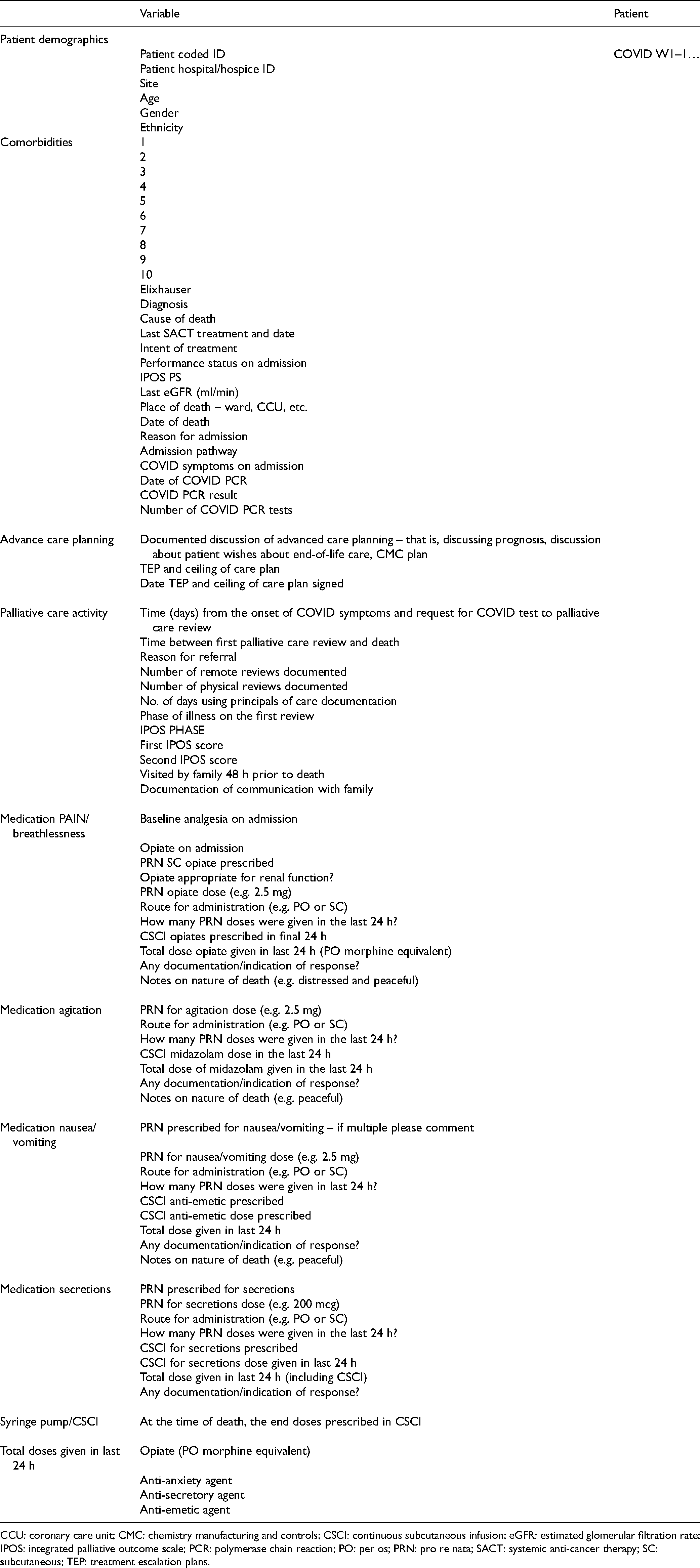
Data were extracted from medication charts and electronic patient records by clinicians (PM, YK, SW, and NW) using a standardised proforma (see Appendixes). This included patient demographics and risk factors for COVID-19 infection such as age, gender, ethnicity, cancer diagnosis, Elixhauser comorbidity index, performance status, SACT intent and last treatment date. Data were also collected to describe the main domains of palliative and end-of-life care service provision, that is:
Identification of individual patients’ needs: The symptoms and palliative care needs of patients were described using the validated integrated palliative outcome scale (IPOS), which is routinely used in clinical care locally and nationally (11). Each of the 17 IPOS items is scored 0–4 with higher scores representing increased severity of symptoms/concerns (12). IPOS scores were recorded on the patients first palliative care review (IPOS 1) and then again on subsequent assessment (IPOS 2). When patients did not have IPOS scores recorded in the electronic patient record, clinical documentation was reviewed by trained clinicians to retrospectively assess patients’ needs and extrapolate IPOS scores. The number of patients scoring 2, 3, and 4 on each IPOS item was calculated and presented as a proportion of the total study population at each time point. The palliative phase of illness at first review was also included (13). Management of pain and other symptoms: Prescriptions for medications across the four main end-of-life symptom domains of pain, anxiety, nausea and respiratory secretions were reviewed including total doses received in the final 24 h prior to death and clinical documentation of effectiveness. Communication and decision making: Documentation of advance care planning (ACP) discussions, including evidence of anticipatory care planning such as treatment escalation plans (TEP) and do not attempt cardio-pulmonary resuscitation (DNACPR) orders were described. Thematic analysis was carried out on documentation regarding communication with family members and any concerns recorded. Responsiveness of the palliative care team: Referrals and reason for palliative care referral, number of times the patients was reviewed by the palliative care team, time from onset of COVID-19 symptoms to initial palliative care review and time from first palliative care review to death were described.
Anonymised data were analysed with standard descriptive statistics using IBM SPSS V27.
Results
Overview
Thirty-four patients were included in this analysis. Twenty-nine non-ventilated COVID-19 PCR positive patients died during the defined time periods. A further five cases who died with a strong clinical suspicion of COVID-19 were also included.
Patient demographics and outcomes are summarised in Table 1. Half of all patients had an initial World Health Organisation (WHO) performance status of 3 (see Figure 1), reflecting their increased care needs.

Patients’ World Health Organisation (WHO) performance status on admission.
Patient Demographics and Findings.

COPD: chronic obstructive pulmonary disease; WHO: World Health Organisation; GI: gastrointestinal; CSCI: continuous subcutaneous infusion.
More patients were referred to palliative care during wave 1 (89% (17/19) compared to 73% (11/15) in wave 2). All patients had a DNACPR order and treatment escalation plan in place at the time of death. The median total opioid (oral morphine equivalent) and benzodiazepine doses administered in the last 24 h before death was 30 mg (range: 5–180 mg) and 10 mg (range: 0–30 mg), respectively. In total, 85% of patients had anticipatory medications prescribed for the four main end-of-life symptoms of pain, nausea, secretions and anxiety. In total, 79% of patients (n = 27) required a continuous subcutaneous infusion (CSCI) of medication in the last 24 h of life.
In total, 82% (n = 28) of patients had documentation that they were settled and comfortable at the time of death. Twelve percent (n = 4) had persistent agitation. Family discussions were held for all patients prior to death. In total, 76.5% (n = 26) of patients had a family member who visited the hospital in their final hours. Fifty percent of the total family concerns identified (n = 20) were regarding the unexpected, rapid deterioration from COVID-19. Concerns about challenges with communication and how families were coping with social distancing measures were also documented.
IPOS scores on initial assessment (IPOS 1) and 24 to 48 h before death (IPOS 2) were completed and recorded in the electronic patient record for 26 patients (76.5%) and 13 patients (38.2%), respectively. Eight patients (23.5%) had IPOS 1 scores extrapolated from clinical records and 21 patients (61.8%) had IPOS 2 scores extrapolated. Figure 2 shows the proportions of patients who had moderate, severe, overwhelming symptoms or concerns in each of the domains. Patient and family anxiety were the most prevalent issues. The most frequently reported physical symptoms were weakness, poor mobility, poor appetite and shortness of breath.

Identification of patient's individual needs using integrated palliative outcome scale (IPOS) on initial (IPOS 1) and subsequent assessment (IPOS 2), n = 34. Number (%) of patients scoring 2, 3 or 4 on IPOS items is presented to represent the number (%) of patients with moderate/severe/overwhelming symptoms or concerns in each IPOS domain. Physical symptoms: 2 = moderately, 3 = severely, 4 = overwhelmingly. Emotional symptoms (anxiety, family anxiety and depression): 2 = sometimes, 3 = most of the time, 4 = always. Feeling at peace, being able to share feelings, having enough information: 2 = sometimes, 3 = occasionally, 4 = not at all. Practical matters: 2 = problems partly addressed, 3 = problems hardly addressed, 4 = problems not addressed.
Discussion
Key quality indicators of good end-of-life care include open communication, personalised care plans, involvement of those caring for the patient and effective assessment and management of distressing symptoms and concerns (14). A prospective study about the care and end-of-life experiences of hospitalised cancer patients dying with COVID-19 was not feasible at the height of the pandemic. In this study, the use of objective measures including IPOS, phase of illness and medication prescriptions, along with a review of documentation in the medical notes has enabled us to describe the end-of-life care provided for hospitalised cancer patients with COVID-19. These data provide a unique, albeit partial, insight into the end-of-life experience of these patients.
Although limited by the small numbers and the retrospective nature of the study, the data reflect all eligible deaths in this tertiary referral cancer centre during two major periods of the COVID-19 pandemic. Ventilated and sedated patients were excluded from the study given their different management and treatment goals. Although we do not have direct information about how the patients and families perceived the end-of-life experience, our data mostly demonstrated a reduction in patients’ symptom burden and concerns following palliative care intervention. The modest doses of medications used suggest that the management of symptoms at end-of-life was uncomplicated. These data mirror other data from non-cancer/mixed populations (15) and are in line with UK guidelines (16). Our results suggest that provided dying is recognised, the end-of-life symptoms of cancer patients dying with COVID-19 could be managed by generalist physicians, supported with comprehensive guidelines and education, and with specialist palliative care input were indicated for more complex cases.
Our study has identified high levels of patient and family anxiety, which persisted after palliative care intervention, and has been previously documented in patients receiving palliative care in a non-COVID setting (11). Thematic analysis of documentation of family communications identified three key areas of concern: rapidity of deterioration with COVID-19, social distancing/isolation, and communication. Our results suggest that death from a transmissible, pandemic disease, associated with social restrictions and uncertainty, adds additional complexity to the dying period (17). An initial rapid patient and public involvement review during COVID-19 (18) described patients’ anxieties about the continued delivery of holistic patient-centred care and the provision of extended bereavement support in the context of a rationed, overburdened health care system. The negative impact of social distancing and barriers to face-to-face communication on bereavement is well recognised (19). Research during the pandemic has highlighted the importance of effective communication and family support (20) and the emergence of novel technologies to overcome social distancing barriers (21). Despite reduced visiting access, a high proportion of patients in this study saw their families in their final hours. Family and carers play a key supportive role as patient advocates throughout the patient's cancer journey (22). The emergence and application of virtual platforms to support communication has been more effective and more normalised since the start of the pandemic (23,24). Further research is needed to enable in-depth exploration of patients and families’ understanding of the diagnosis and impact of COVID-19 on their anti-cancer regimen and expected prognosis.
All the patients in this study were seen at a tertiary referral cancer centre and were receiving ongoing SACT. All patients had appropriate personalised TEPs and DNACPR recommendations in place. Discussions with patients and families about preferences and wishes at end-of-life including resuscitation status and TEP form part of the process of ACP (25). Timely recognition of the vulnerability of cancer patients with COVID-19 and prompt, open communication regarding ACP can facilitate high-quality end-of-life care (26). Recognising dying patients, however, is a skill that requires experience. When facing another wave of the pandemic, training and support on recognising deteriorating patients must be prioritised.
The need for palliative care to be embedded within contingency planning for further and future pandemics has been recognised (27). Our data support a parallel focus of embedding palliative care early within the cancer treatment pathway to proactively ensure the best quality of life and end-of-life care for cancer patients.
Conclusions
We provide a unique insight into the end-of-life experience of cancer patients dying with COVID-19 at a tertiary referral cancer centre. The medical management of cancer patients dying from COVID-19 is relatively uncomplicated. As a transmissible disease, associated with social restrictions and anxiety, death from cancer and COVID-19 is complex. Our data demonstrate that prompt identification of palliative care symptoms and concerns can facilitate proactive symptom management, anticipatory communication about patients’ priorities and enhance family support. We recommend that palliative care service provision and training in the management of symptoms at end-of-life should be embedded within preparations for further pandemic case surges and during the COVID-19 recovery phase.
Footnotes
Ethical Approval
Ethical approval is not applicable to this article.
Patient Consent
There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Study Proforma
| Variable | Patient | |
|---|---|---|
| Patient demographics | ||
| Patient coded ID | COVID W1–1… | |
| Patient hospital/hospice ID | ||
| Site | ||
| Age | ||
| Gender | ||
| Ethnicity | ||
| Comorbidities | 1 | |
| 2 | ||
| 3 | ||
| 4 | ||
| 5 | ||
| 6 | ||
| 7 | ||
| 8 | ||
| 9 | ||
| 10 | ||
| Elixhauser | ||
| Diagnosis | ||
| Cause of death | ||
| Last SACT treatment and date | ||
| Intent of treatment | ||
| Performance status on admission | ||
| IPOS PS | ||
| Last eGFR (ml/min) | ||
| Place of death – ward, CCU, etc. | ||
| Date of death | ||
| Reason for admission | ||
| Admission pathway | ||
| COVID symptoms on admission | ||
| Date of COVID PCR | ||
| COVID PCR result | ||
| Number of COVID PCR tests | ||
| Advance care planning | Documented discussion of advanced care planning – that is, discussing prognosis, discussion about patient wishes about end-of-life care, CMC plan | |
| TEP and ceiling of care plan | ||
| Date TEP and ceiling of care plan signed | ||
| Palliative care activity | Time (days) from the onset of COVID symptoms and request for COVID test to palliative care review | |
| Time between first palliative care review and death | ||
| Reason for referral | ||
| Number of remote reviews documented | ||
| Number of physical reviews documented | ||
| No. of days using principals of care documentation | ||
| Phase of illness on the first review | ||
| IPOS PHASE | ||
| First IPOS score | ||
| Second IPOS score | ||
| Visited by family 48 h prior to death | ||
| Documentation of communication with family | ||
| Medication PAIN/breathlessness | Baseline analgesia on admission | |
| Opiate on admission | ||
| PRN SC opiate prescribed | ||
| Opiate appropriate for renal function? | ||
| PRN opiate dose (e.g. 2.5 mg) | ||
| Route for administration (e.g. PO or SC) | ||
| How many PRN doses were given in the last 24 h? | ||
| CSCI opiates prescribed in final 24 h | ||
| Total dose opiate given in last 24 h (PO morphine equivalent) | ||
| Any documentation/indication of response? | ||
| Notes on nature of death (e.g. distressed and peaceful) | ||
| Medication agitation | PRN for agitation dose (e.g. 2.5 mg) | |
| Route for administration (e.g. PO or SC) | ||
| How many PRN doses were given in the last 24 h? | ||
| CSCI midazolam dose in the last 24 h | ||
| Total dose of midazolam given in the last 24 h | ||
| Any documentation/indication of response? | ||
| Notes on nature of death (e.g. peaceful) | ||
| Medication nausea/vomiting | PRN prescribed for nausea/vomiting – if multiple please comment | |
| PRN for nausea/vomiting dose (e.g. 2.5 mg) | ||
| Route for administration (e.g. PO or SC) | ||
| How many PRN doses were given in last 24 h? | ||
| CSCI anti-emetic prescribed | ||
| CSCI anti-emetic dose prescribed | ||
| Total dose given in last 24 h | ||
| Any documentation/indication of response? | ||
| Notes on nature of death (e.g. peaceful) | ||
| Medication secretions | PRN prescribed for secretions | |
| PRN for secretions dose (e.g. 200 mcg) | ||
| Route for administration (e.g. PO or SC) | ||
| How many PRN doses were given in the last 24 h? | ||
| CSCI for secretions prescribed | ||
| CSCI for secretions dose given in last 24 h | ||
| Total dose given in last 24 h (including CSCI) | ||
| Any documentation/indication of response? | ||
| Syringe pump/CSCI | At the time of death, the end doses prescribed in CSCI | |
| Total doses given in last 24 h | Opiate (PO morphine equivalent) | |
| Anti-anxiety agent | ||
| Anti-secretory agent | ||
| Anti-emetic agent |
CCU: coronary care unit; CMC: chemistry manufacturing and controls; CSCI: continuous subcutaneous infusion; eGFR: estimated glomerular filtration rate; IPOS: integrated palliative outcome scale; PCR: polymerase chain reaction; PO: per os; PRN: pro re nata; SACT: systemic anti-cancer therapy; SC: subcutaneous; TEP: treatment escalation plans.
Proforma Tool for Reviewing Medication Charts

|
|
|
|
|
|
| Baseline opioids prescribed on admission – please check Med Rec on the back page | |
| PRN opiate prescribed with dose, route and frequency (e.g. 2.5 mg morphine SC 4 hourly). | |
| How many PRN doses were given in the last 24 h? | |
| CSCI opiates prescribed in final 24 h (with dose) | |
| Total dose opiate given in last 24 h (PO morphine equivalent) | |
|
|
|
| PRN prescribed for terminal agitation | |
| - If multiple prescribed please comment which ones and fill out information for all prescribed | |
| PRN for agitation dose and route (e.g. 2.5 mg SC) | |
| How many PRN doses were given in the last 24 h? | |
| CSCI anti-anxiety prescribed in last 24 h (with dose) | |
| Total dose given in last 24 h | |
|
|
|
| PRN prescribed for nausea/vomiting | |
| - If multiple prescribed please comment which ones and fill out information for all prescribed | |
| PRN for nausea/vomiting dose and route (e.g. 8 mg SC) | |
| How many PRN doses were given in the last 24 h? | |
| CSCI anti-emetic in last 24 h (with dose) | |
| Total dose given in last 24 h | |
|
|
|
| PRN prescribed for secretions | |
| - If multiple prescribed please comment which ones and fill out information for all prescribed | |
| PRN for secretions dose and route (e.g. 200 mcg SC) | |
| How many PRN doses were given in the last 24 h? | |
| CSCI for secretions prescribed given in last 24 h (with dose) | |
| Total dose given in last 24 h | |
|
|
|
| Was CSCI via a syringe pump prescribed? | |
| At the time of death, the end doses prescribed in CSCI: |
CSCI: continuous subcutaneous infusion; PO: per os; PRN: pro re nata; PS: performance status; SC: subcutaneous.