
Abstract
Although there are studies on the use of social media and palliative and end-of-life care (PEOLC), there are no studies specifically investigating the content of online public feedback about PEOLC services. This study sought to understand experiences of end-of-life care provided in hospitals in the West of Scotland by exploring the main themes within the content of stories posted on a nationally endorsed nonprofit feedback online platform, Care Opinion, within a 2-year period. We used “Appreciative Inquiry” as a theoretical framework for this study to determine what works well in end-of-life care, while also identifying areas for further improvement. Of the 1428 stories published on “Care Opinion” from March 2019 to 2021 regarding hospitals in the West of Scotland, 48 (3.36%) were related to end-of-life care, of which all were included in data analysis. Using the software package NVivo and thematic analysis, we identified 4 key themes. We found that people overwhelmingly posted positive feedback about their experiences with end-of-life care. People reported positively about staff professionalism in providing compassionate and person-centered care to meet their loved ones needs at end of life. Other experiences of care related to challenges facing healthcare services, particularly during the COVID-19 pandemic. Quality appraisal of staff responses highlighted areas for improving feedback. This study can add to the aim of improving staff response to people’s concerns about end-of-life care. This study has provided a novel perspective of patients’ experiences of end-of-life care in hospitals in the West of Scotland. Novel insights were the appreciation of quality of care, staff professionalism, effective communication, and meeting patient’s needs at end-of-life particularly by nursing staff.
Keywords
Introduction
With the rapid growth of digital innovations over the last decade, new ways of gathering online feedback have been promoted alongside the traditional use of paper survey questionnaires. 1 According to a report on online consumer behavior in the United Kingdom (UK), 2 three-in-four users of the Internet read comments prior to buying a product or service and two-in-five post online reviews.
There is an increasing focus in Scotland on patient experience as an aspect of patient safety and quality improvement. Care Opinion is a nationally endorsed nonprofit public feedback platform for health and social care services that was set up in the UK in 2005. 3
There is little analysis of why people post on Care Opinion, how staff respond, and how people feel about the responses they receive. A survey conducted as part of a major UK review of online feedback, Improving National Health Service (NHS) Quality Using Internet Ratings and Experience (INQUIRE), found that online feedback is seen by those posting online reviews or comments as more positive than expected. 4 Providing information for other service users (39%), expressing admiration for a service (36%), and contributing to the quality of care within the NHS (15%) were the top reasons for providing feedback. Complaining about a service, treatment, or professional was less common compared to providing praise.
In palliative and end-of-life care (PEOLC) feedback can identify areas where changes can be made, or services improved. There is little published research on the content of “Care Opinion” posts in the context of PEOLC. The collation and analysis of people stories is a useful exercise, facilitating understanding of the wide-ranging experiences of service users when receiving end-of-life care in acute hospitals within NHS Greater Glasgow and Clyde (NHSGGC).
Aim
This study was part of the first phase of a larger multi-method participatory action research in which we aimed to identify the main themes within the content of online feedback/stories on the “Care Opinion” platform provided by people regarding their experiences of end-of-life care in hospitals within NHSGGC. The focus of this study was on the “Discovery” phase of the 4D cycle to map best practices and gain insights particularly—though not exclusively—of what service users appreciate in their stories on “Care Opinion” about end of life care at hospitals within the NHSGGC.
Methods
To approach this study, we sought a framework that allows generating a sense of optimism, creativity, and motivation for change through using available resources and current strengths in place. Therefore, an “Appreciative Inquiry” (AI) lens was chosen to guide this study to gain an understanding of care that went well, while identifying and learning from negative aspects of care. 5
AI is a strength-based approach focusing on the assets of an organization and its stakeholders’ values that includes building effective partnerships and collaborations between researchers, practitioners, and service users through encouraging less hierarchical structures and more equalized power to identify and build upon positive mechanisms and outcomes across the system. 6 AI comprises 4 iterative phases (discovery, dream, design, and destiny) known as the 4D cycle that are flexible and can be adapted to different settings and populations.
The AI approach was used to develop a framework based on service users’ vision of change to service from a “bottom–up” perspective. As AI values wholeness and humanity, it complements values of holistic care and compassion thereby supporting the specific context of end-of-life care.
We conducted a thematic analysis of public feedback stories about end-of-life care posted on Care Opinion Scotland during a 2-year period as well as quality appraisal of stories’ associated with professional responses.
A subscription was granted by Care Opinion for full access to the platform for ease of data extraction and additional functions (eg, data access, report generation, and visualization). The two analyzing authors attended training sessions on the platform and its features.
Data Collection
We gathered and analyzed public feedback stories, and their associated staff responses, posted on Care Opinion Scotland over a 24-month period (March 2019-2021) relevant to end-of-life care provided in acute hospitals across NHSGGC. As pressures on health services have been greatest since the onset of the COVID-19 pandemic, we included 2019 to review more heterogeneous comment/feedback pool.
Search filters were designed in conjunction with our patient and public involvement (PPI) group, the patient experience team at NHSGGC, and the director of Care Opinion Scotland to maximize sensitivity and specificity (Table 1).
Search Strategy.

Abbreviation: NHS, National Health Service.
Two authors ran the search and screened stories for inclusion independently using an inclusion criteria form (see Appendix 1). Ambiguous results were resolved by discussion within the research team.
Inclusion/ Exclusion Criteria
Feedback was included in the study if they discussed the treatment or diagnosis of a life-limiting condition, end-of-life care experience, or service in hospital settings within NHSGGC. Stories that related to primary care, nonhospital services were excluded. Any disagreement was resolved by discussion with the research team.
Data Analysis
To understand the content of people stories/ feedback, Braun and Clarke's six-phase reflexive thematic analysis 7 was used in conjunction with using NVivo by QSR International 8 to organize the qualitative data.
The extracted data was read by two members of the research team (SK, SR) to gain familiarity with feedback content and achieve data immersion for the development of codes. A provisional coding framework for the analysis was then refined through multiple iterations to produce a final coding framework. The final codes were categorized into themes/subthemes and reviewed by two clinical experts in palliative care to discuss differences in opinion and reach a consensus. Stories were read and classified as positive, negative, or mixed in relation to the end-of-life care content and tone.
Existing staff responses were quality-appraised using the Plymouth Listen, Learn and Respond Framework (PLLRF). Baines et al. 9 co-designed and tested the PLLRF framework as a best-practice response for evaluating the quality of staff responses to Care Opinion posts by identifying different factors considered influential in effective organizational responses from a patient perspective. The framework has been also successfully applied to staff responses to Care Opinion in various fields, beyond its original use in mental health services.1,6 Where there was more than one staff response to a story, the most detailed response was chosen for the quality appraisal.
Results
Of the 1428 stories published on “Care Opinion” from March 2019 to 2021 regarding NHSGGC, 48 (3.36%) related to end-of-life care in acute hospitals. Four core themes were identified from qualitative analysis:
Feelings about the experience of end-of-life care. Meeting needs at end of life. Information and communication. Healthcare challenges.
The majority of stories were coded more than once and grouped into 2-or-more themes or subthemes. Based on the research team’s interpretations of stories content and tone, three quarters were classified as positive (n = 36/75%), less than one-fifth of stories were negative (9/48, 18.8%); the remaining were mixed (n = 3/6.3%). “Feelings about the experience of end-of-life care” was the prevalent theme with the most expressing their appreciation toward staff (39/48, 81.25%). Table 2 provides a summary of themes/subthemes contained in people stories with a selection of representative quotes illustrating each theme.
Summary of Themes and Subthemes and Representative Quotes.
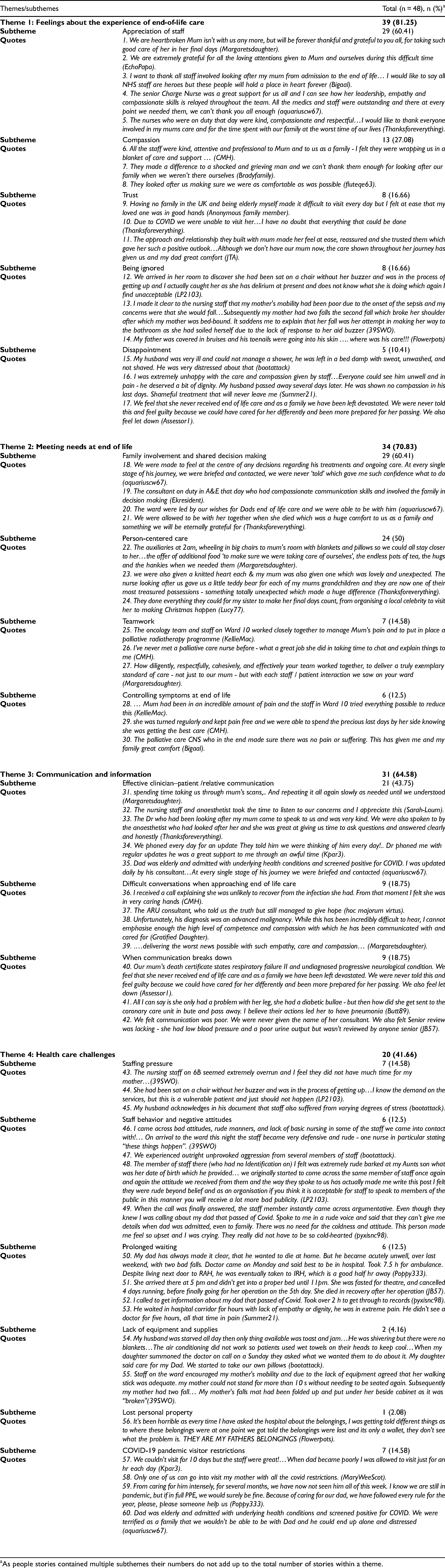
As people stories contained multiple subthemes their numbers do not add up to the total number of stories within a theme.
Feelings About the Experience of end-of-Life Care
Feedback relating to feelings about end-of-life care experiences was mixed. The majority of stories praised staff and conveyed gratitude. “Compassionate”, “supportive”, “kind”, “respectful”, “professional”, and “competent” were common terms used to describe staff (Table 2, quotes 1-5). “Compassion” was mentioned in several stories and was fundamental to positive relatives’ experiences during end-of-life care (Table 2, quotes 6-8). ‘Trust’ was very important when family members were not able to visit their loved ones in hospital (Table 2, quotes 9, 10). Effective patient-clinician relationships were perceived as a key element in building trust and reassurance - comforting both patients and relatives during end-of-life care (Table 2, quote 11).
Some responders included negative care experiences in their posts. Staff disregarding family concerns about their loved one's condition (Table 2, quotes 12, 13), unsafe environments/surrounding for vulnerable patients (Table 2, quotes 12), inadequate care, lack of dignity, and compassion (Table 2, quotes 14, 16), particularly in the absence of family members (Table 2, quotes 13) were evident in people stories. These were associated with strong feelings of being ignored and disappointment toward staff and quality of end-of-life care. When family members were uncertain about the reasoning for their family members sudden deterioration before death, experiences of end-of-life care could become unpleasant and disappointing (Table 2, quote 17).
Meeting Needs at end of Life
People commonly described positive experiences of how staff were supportive of meeting their loved ones needs at the end of life.
Family involvement and shared decision making during end-of-life care were reflected in several of the posts and appeared to be highly important to meeting needs at the end of life. The perception of “being at the center of any decisions regarding treatment and care” was often detailed through the use of effective phrasing. For example, as evidenced in one of the stories, they were never “told” but rather shared the decision making. This highlights the importance of two-way patient-provider relationship and the transition of patients and family members from passive recipients of care and treatment to active participants (Table 2, quotes 18, 19). Facilitating family presence at the time of death was a key concern in feedback with end-of-life care which was consistent with their wishes (Table 2, quote 20). This also helped them accept the situation, feel comfort, and give meaning to the trajectory of life-limiting illness and death as well as to their own experience (Table 2, quote 21).
The provision of person-centered care was regularly highlighted and indicative of high-quality care from the relatives’ perspective. Providing welcoming spaces and comfortable amenities to allow overnight visiting were highlighted as an important resource for relatives (Table 2, quotes 22, 23). While the experience of a family member’s death could have significant impacts on bereaved relatives, they reported that receiving “something totally unexpected” such as a knitted heart or teddy bear from nursing staff is important in memory-making in their bereavement (Table 2, quote 24). They noted the efforts of staff in “making final days of their loved one count” through organizing family gatherings (Table 2, quote 25). Stories noted this made a “huge difference”.
Multidisciplinary teamwork was repeatedly described as “positive” and “core” to good end-of-life care (Table 2, quotes 25-27). Praise for the wide range of health professionals involved in end-of-life care was evident (Table 2, quote 27).
Controlling symptoms was associated with good care at end of life, giving a sense of comfort in family experiences. Pain was the most frequent symptom highlighted in stories. People perceived that staff helped to reduce pain in dying patients (Table 2, quotes 28-30).
Communication and Information
Feedback reported positively the skills and professionalism of team members in communicating in an honest and empathic manner during end-of-life care. The competency of nurses and doctors was highlighted, as was making time to talk, actively listening to concerns, and ensured the information provided was sufficient and comprehensible (Table 2, quotes 31-33). Despite visitor restrictions due to the COVID-19 pandemic, communication by telephone/video call was perceived as optimal and families were kept appropriately informed (Table 2, quotes 34, 35).
One key feature of positive reviews was that clinicians were skilled and competent enough in breaking sad news with empathy (Table 2, quotes 36, 37). The acts of kindness and compassion shown when approaching end-of-life care had a positive impact on the relationship between the health care provider and family (Table 2, quotes 38, 39).
In other cases, relatives experienced a lack of proactive regular communication with the health care team. This was often associated with a breakdown in the trust between relatives-clinicians (Table 2, quote 40-42).
Health Care Challenges
Difficult working conditions, low staff numbers, high work volume, and lack of time spent caring have been noted by some relatives as a marker of poor care (Table 2, quotes 43-45).
Perceived lack of dignity and respect was a factor in reporting a negative care experience in some stories (Table 2, quotes 46, 47). This included both clinical and nonclinical staff (Table 2, quote 48). On reflection, relatives noted sensitivity to the quality of verbal communication. Families expected that the choice of word, tone, and pitch of voice be adapted to their emotions particularly during the difficult time of the COVID-19 pandemic (Table 2, quote 49).
Prolonged waits for ambulances, hospital beds, planned care, and treatment were highlighted as having the potential to adversely impact relatives’ experience. This was seen to be associated with lack of coordination/consistency across services (Table 2, quote 50-52). It was frustrating and worrying for family members when they witnessed their loved ones in pain for several hours, waiting in the hospital to be visited by a health care professional (Table 2, quote 53).
When basic essential equipment was in short supply there were negative experiences of end-of-life care (Table 2, quotes 54, 55).
The negative experience of missing cash or valuables belonging to the deceased loved ones was in the minority in the analyzed stories (Table 2, quote 56). However, it does highlight the importance of collecting and managing patients' personal property.
Total ban on visits and end of life only visiting policies during the COVID-19 pandemic were felt to be insufficient and had a negative impact on family members’ experiences (Table 2, quotes 57-60). Families felt that if visits had been permitted, they would be able to play their role in supporting and caring for their loved ones (Table 2, quote 59). Visitor restriction was associated with a very strong feeling of powerlessness and distress. Visits were perceived by relatives as essential for not letting the patient die alone (Table 2, quote 60).
Analysis of Staff Responses
All stories received a response within 7 days with only one “changes made” reported. There were 58 responses in total, from 28 staff members. The majority of responses came from the nursing team (n = 25/43.1%) or from the Patient Experience and Public Involvement Team (n = 13/22.41%). The response by job title is presented in Table 3.
Spread of Responders by job Title.

We used thematic analysis to summarize how responses performed against the “PLLRF” criteria. 6 As illustrated in Table 4, boxes marked in green show good practice while red boxes suggest areas for possible.
Staff Responses and Quality Appraisal of Existing Responses.

“Plymouth Listen, Learn and Respond framework” (PLLR).
“Traffic light” colour coding system (green ≥ 60% good practice; orange = 50% to 60% acceptable; and red ≤ 50% areas for possible improvement.
*Only applicable to positive or mixed stories.
**Only applicable to negative or mixed stories
In terms of response type, negative stories commonly received offline responses with responders keener and more comfortable in addressing these concerns in other forums. This may reflect either discomfort with addressing challenging issues in a public forum, or an effort to respond in a comprehensive and considered manner. Positive stories mainly received appreciative responses in which it was commonly highlighted that relevant staff members would be identified and feedback would be passed on. However, it was rarely clear if the appropriate team or individual had successfully received the feedback.
Both positive/negative stories often received thanks/apologies. Thanks were commonly offered regarding specific elements of the feedback, particularly, the beneficial impact positive feedback could have on staff performance and their confidence. Respondents also offered thanks, regardless of the feedback content, for the time and effort people had spent describing their experiences of end-of-life care. Where people had reported negative experiences, apologies were made by responders, prompting the story author to continue the conversation via various methods from providing their contact details to sign posting to patient experience teams or other relevant services. However, it was unclear to what extent staff was able to learn from the story and improve the delivery of subsequent end-of-life care.
Discussion
Our findings of feedback sentiment support the notion that online feedback is generally positive, as sentiment leaned toward positive stories. There is also evidence that respondents to questionnaires/satisfaction scores tend to come from the extremes such as those very satisfied and those very unsatisfied. 2 Using AI's “Discovery” phase helped bring to light the service’s positive capacity in regard to end-of-life care, in order to discover and make explicit “what works “or “what is already going well”. Relatives commonly reported positively about staff professionalism, particularly in providing person-centered care and family support. Experiences of communication with healthcare providers also were described positively, highlighting the importance of building rapport, allocating adequate time to provide information and updates to patients and their families in every stage of end-of-life care. Despite this, when people felt one-or-more aspects of their loved ones care was missing, they were more likely to report negative experiences.
Although AI is a “strength-based” approach, we have highlighted negative care experiences to prevent data neglect associated with problems or concerns.
Disappointment was also expressed in relation to staffing pressure, prolonged waiting, lack of equipment, lost personal property, and visiting restrictions. These often resulted from multiple factors, for example, the COVID-19 pandemic. However, such problems should be fed back to hospitals in order to identify causes and prompt improvement.
A further finding was that despite research suggesting transparent, conversational responses are more desirable by service users,6,10 they were the least popular type of responses in our sample and were mostly from negative stories. In contrast, appreciative responses were commonly from families reporting positively about their experiences of end-of-life care. This suggests that positive stories are less likely to be utilized to improve experiences of healthcare, and that negative feedback is more likely to be used to impact the way that subsequent care is delivered.
Limitations
Similar to all research exploring the impact of technology on improving health care, users of such services are not necessarily representative of the overall population, with low-literacy, disabled and older adults, and those who have limited access to the Internet being less likely to provide online feedback.11,12
Furthermore, due to the anonymity of data on Care Opinion, sociodemographic characteristics of the story authors are not known.
There are a higher number of positive posts compared to negative ones on Care Opinion11,12 and this was evident in our study. Therefore, there is limited data on how service users perceive suboptimal care or articulate negative experiences.
This study offers a starting place for exploration of end-of-life care experienced by families but future research with dying patients and hospital staff would enable greater understanding and potential improvements to services or care.
Conclusion
This study has provided a novel perspective of patients’ experiences of end-of-life care in hospitals within NHSGGC. Novel insights were the appreciation of quality of care, staff professionalism, effective communication, and meeting patient's needs at end of life particularly by nursing staff.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221103029 - Supplemental material for Views of Care at End of Life: A Secondary Analysis of Online Feedback Using Care Opinion
Supplemental material, sj-docx-1-jpx-10.1177_23743735221103029 for Views of Care at End of Life: A Secondary Analysis of Online Feedback Using Care Opinion by Sahar Khonsari, Claire O Neill, Catriona R Mayland, Fraser Gilmour, Marc Aitken, Alistair Mckeown, Sian Russell, Angela Mcalees, Morag Gardner and Bridget Johnston in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735221103029 - Supplemental material for Views of Care at End of Life: A Secondary Analysis of Online Feedback Using Care Opinion
Supplemental material, sj-docx-2-jpx-10.1177_23743735221103029 for Views of Care at End of Life: A Secondary Analysis of Online Feedback Using Care Opinion by Sahar Khonsari, Claire O Neill, Catriona R Mayland, Fraser Gilmour, Marc Aitken, Alistair Mckeown, Sian Russell, Angela Mcalees, Morag Gardner and Bridget Johnston in Journal of Patient Experience
Footnotes
Acknowledgments
The authors would like to thank the patient experience team NHS GGC, Care Opinion Scotland, and all the anonymous family members and friends who posted on Care Opinion.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scottish Government.
Author’s Contribution
All authors provided substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data for the work, drafted the work or revised it critically for important intellectual content, provided final approval of the version to be published, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethical Approval
Ethical approval is not applicable for this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.