
Abstract
A descriptive review was conducted to evaluate the evidence of cognitive patient-reported outcome measures (PROMs) following cardiac surgery. The search of electronic databases resulted in 400 unique manuscripts. Nine studies met the criteria to be part of the final review. Results of the review suggest that there are few validated PROMs that assess cognitive function in the cardiac surgical population. Furthermore, PROMs have not been used to assess overall cognitive function following cardiac surgery within the past decade. However, one domain of cognitive function—memory—was described, with up to half of patients reporting a decline postoperatively. Perceived changes in cognitive function may impact health-related quality of life and a patient’s overall view of the success of their surgery. Early identification of cognitive changes measured with PROMs may encourage earlier intervention and improve patient-centered care. In clinical practice, nurses may be in the best position to administer PROMs preoperatively and postoperatively.
Introduction
Much of the research on clinical outcomes in cardiothoracic surgery focuses on objective end points such as perioperative morbidity and short- and long-term survival (1). Although these measures have their place in influencing treatment decisions, they may be less meaningful to patients by not capturing the entirety of their personal experience. It has been suggested that objective markers may be an insufficient measure of the patient’s postoperative recovery (1,2). This has resulted in a movement toward patient-centered care, with a shift in measuring outcomes from the patient’s perspective (1).
Patient-reported outcome measures (PROMs) are validated tools that measure physical, mental, and emotional well-being obtained by patient self-report (1,3). These measures can provide information on a range of health status outcomes in a consistent manner across patients and providers that are nonetheless still sensitive to changes in the patient’s condition (3). Patient-reported outcome measures in cardiovascular care are classified as either generic, such as the Short-Form 36, or disease-specific, such as the Minnesota Living with Heart Failure Questionnaire (4). When utilized serially over time, PROMs may provide a more accurate representation of changes in patient status allowing for earlier intervention (1). PROMs are critical in reducing the rift between medicine and humanistic disciplines while also making the care process more patient centered (5). For the purposes of this review, a PROM is any validated or researcher created tool used to measure patient self-reported cognitive well-being.
Postoperative cognitive dysfunction (POCD) is a subtle disorder of thought processes, which may influence isolated domains of cognition such as memory, attention, executive functioning, or concentration (6). However, defining and detecting POCD is problematic as evidenced by the wide variety of definitions in the literature (7,8). For the purposes of this review, POCD is broadly defined as any self-report of decreased cognitive function after cardiac surgery. Furthermore, POCD must be distinguished from postoperative delirium, for POCD has no fluctuations in consciousness, has a prolonged duration, and is evident after the immediate postoperative period (6,7). Nonetheless, postoperative delirium has been shown to be an independent risk factor for POCD in cardiac surgery patients (9). A recent meta-analysis found that 43% of coronary artery bypass grafting (CABG) patients experienced objective cognitive impairment in the acute phase after surgery (10). There is a general consensus that POCD improves over time, with 19% to 30% continuing to experience cognitive decline at the 6-month postsurgical mark (10,11).
Postoperative cognitive dysfunction is most commonly assessed and diagnosed using an assortment of objective neuropsychological tests administered pre- and postsurgery (12). However, due to the varying definitions and the combinations of neuropsychological tests used to assess POCD, the incidence reported in the literature varies from 40% to 60% within 4 weeks of surgery (11). While some reports describe POCD as one of the most common complication of cardiac surgery, others describe the incidence as vastly overestimated due to poor study designs and the ongoing definitional issues (11,12). Interestingly, most definitions of POCD do not account for patient-reported perceptions of cognitive decline.
Purpose
The purpose of this descriptive review was to evaluate the evidence of the measurement and results of patient-reported cognitive outcomes following cardiac surgery.
Methods
An academic reference librarian assisted in the development of a Boolean search protocol, implemented on July 15, 2019. For the purposes of this review, the cognitive domains identified and utilized for search terms included those found in The Montreal Cognitive Assessment (MoCA) scale, which is composed of visuospatial/executive function, naming, attention, memory, language, abstraction, delayed recall, and orientation (13). The MoCA was selected to develop search terms based on its widespread use and familiarity to the interdisciplinary team. Furthermore, the MoCA is sensitive and specific in detecting impairment when compared to traditional cognitive tests of executive functioning and performance in the MoCA subsections predicts impairment in their respective cognitive domains (14). The detailed search strategy can be found in Supplementary materials.
A total of 788 articles were retrieved searching the electronic databases MEDLINE (1946 to present by OVID), EMBASE, Cochrane Library, CINAHL Plus with Full-Text, Scopus, and Web of Science Core Collection (Figure 1). Once duplicates were removed, 400 articles remained and title and abstract reviews were completed to identify manuscripts related to the research question. Studies were selected for full-text review if the abstract described a cardiac surgical focus that included CABG or valve surgery an adult surgical patient population a reference to a cognitive focus the use of a PROM

PRISMA diagram.
This resulted in 24 manuscripts selected for a full-text review. Of these manuscripts, 9 were selected for this descriptive review (Tables 1 and 2).
Full-Text Studies Excluded With Reasons (n = 15).

Abbreviation: PROM, patient-reported outcome measure.
Summary of Studies Selected for Review (n = 9).
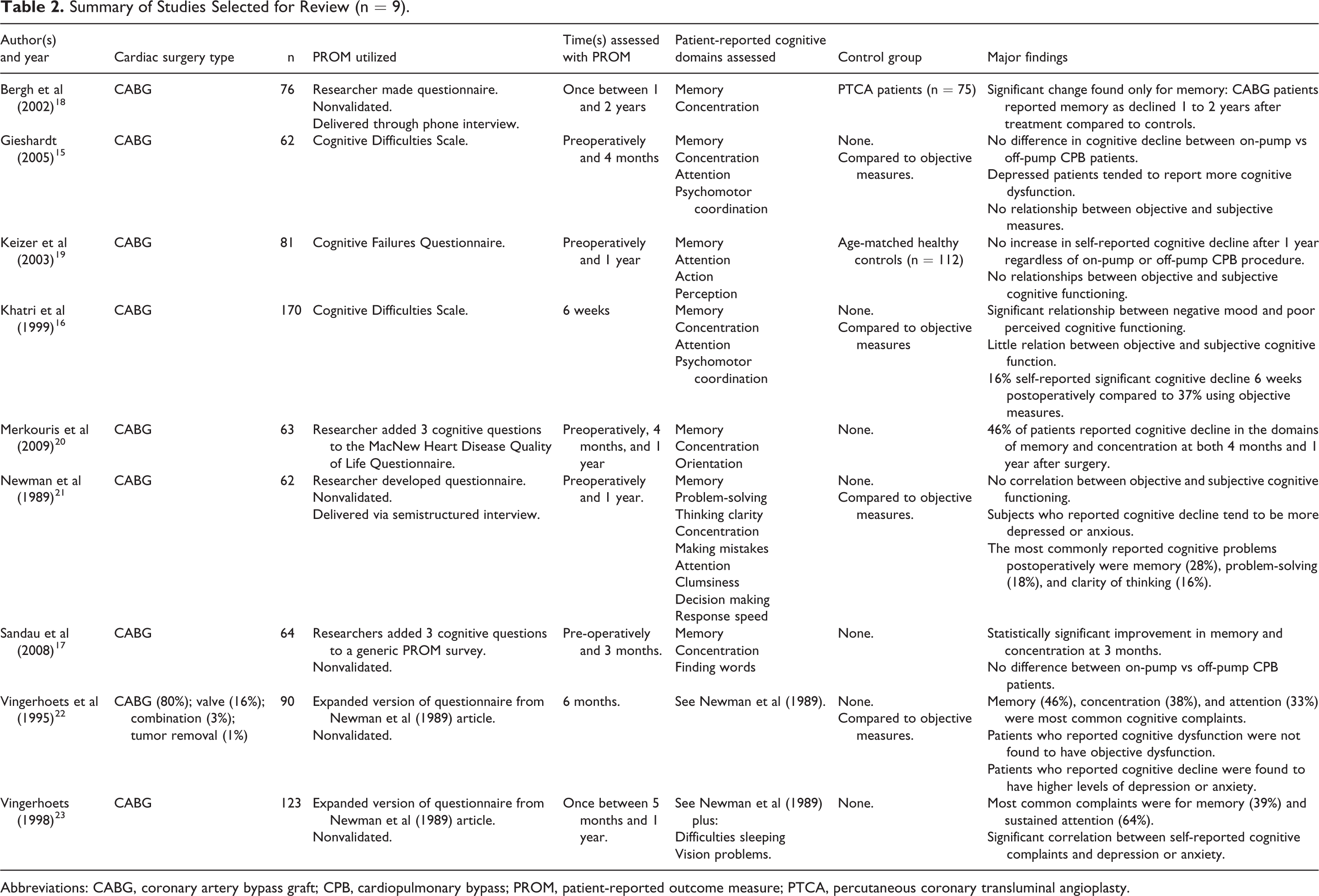
Abbreviations: CABG, coronary artery bypass graft; CPB, cardiopulmonary bypass; PROM, patient-reported outcome measure; PTCA, percutaneous coronary transluminal angioplasty.
Results
The 9 studies selected for inclusion (Table 2) were published between the years 1989 and 2009. There were no studies identified in the search protocol that evaluated cognitive PROMs in the cardiac surgery population within the past decade (2010-2019). Three of studies occurred in Canada (15) and the United States (16,17), and 6 studies were completed in Europe (18 -23). The most common surgery type across all studies was CABG, with only 1 study including patients who underwent valve replacement, combination of valve replacement with CABG, and/or tumor removal surgeries in their cohort (22). The number of participants in these studies ranged from 62 to 170 patients.
Of the 9 studies, 7 used prospective study designs (15 -17,19 -22). Three studies used validated PROMs to measure cognitive dysfunction, including the Cognitive Difficulties Scale (CDS) and the Cognitive Failures Questionnaire (CFQ) (15,16,19). All other cognitive outcomes were measured using nonvalidated researcher developed questions. Two studies (22,23) used a base questionnaire developed by Newman and colleagues (21) and expanded the questionnaire by adding additional questions. Most of these PROMs were administered on paper, although 2 used verbal interviews (18,21). The most common cognitive domains assessed across all studies were memory, concentration, and attention. General cognitive function was not assessed by the manuscripts included in the review.
Only 2 studies included formalized control groups for comparison (18,19). The participants of 4 studies acted as their own control by comparing subjective PROM findings to objective neuropsychological measures, such as the Rey Auditory Verbal Learning Test, the Trail Making Test, or the Purdue Pegboard Test, among others (15,16,21,22). The final 3 studies had no control group (17,20,23). Five studies used PROMs as part of their baseline assessment, while the others only used PROMs as part of their follow-up sessions (15,17,19 -21). The time for these follow-up sessions ranged from 6 weeks to 2 years postoperatively, with only 1 study assessing their patients at multiple time points after surgery (20).
While few studies measured all cognitive domains, a number of studies measured 1 or more common domains. Memory was the most frequently assessed and reported domain, with 28% to 46% of patients experiencing decline in memory following surgery. Of the studies that evaluated on-pump versus off-pump cardiopulmonary bypass (CPB), all reported no difference in cognitive outcomes between patients in either group (15,17,19). Five studies reported that the presence of depression and/or anxiety was correlated with cognitive decline (15,16,21 -23). Interestingly, it was found that reports of subjective cognitive complaints did not correlate with objective cognitive test results (15,21,22). Only 1 study found an improvement in cognitive function postoperatively (17).
Discussion
The results of this review suggest that although self-reported cognitive decline following CABG surgery is a common issue, few studies use validated PROMs to assess changes in cognitive function following cardiac surgery. In addition, when cognitive PROMs were used following cardiac surgery, they were not confirmed using traditional objective measures. Methodologically speaking, there are a variety of issues with the studies found in this review, necessitating a refreshed look at this important area of research.
Several studies in this review categorized patients between on-pump versus off-pump CPB groups and compared their cognitive function postoperatively (15,17,19). Prior to these studies, there was a debate as to whether or not the use of a CPB pump was a factor in the development of cognitive decline. The results of these studies suggest that CPB does not have an impact on subjective cognitive decline in the cardiac surgery population and this assertion is supported by more recent reviews (11,12). Current research is now moving toward investigating anesthetic, inflammatory, or preexisting neurovascular causes (12). However, the development of cognitive decline is likely to be multifactorial, consisting of both surgical and patient factors (12).
Similar to the definitional issues surrounding objectively measured POCD, there appears to be debate regarding which domains sensitively measure cognitive decline. Although cognitive domains such as memory, concentration, and attention were commonly assessed, there were studies that measured less well-validated domains of cognitive functioning. For example, Vingerhoets (23) assessed vision problems and difficulties sleeping. In addition, there appear to be overlapping concepts across studies. For example, separate studies assessed the domains of psychomotor coordination, action, and clumsiness (15,16,19,21). Likely these concepts overlap, but a standard definition of which domains are included in the assessment of cognitive function would provide clarity. For the purpose of this review, the cognitive function domains used as search terms were those identified in the MoCA (13). Given that this tool was only published in 2005 and the fact that this review only identified studies published between 1989 and 2009, the domains used as search terms may not have included domains reported in this review.
It is of note that no studies were identified within the past decade that measured patient-reported cognitive function following cardiac surgery. Numerous studies have evaluated cognitive function postoperatively using data collected by the care provider. For example, there were 2 meta-analyses published in 2018 that evaluated cognitive outcomes following cardiac valve surgery and transcatheter aortic valve implantation (TAVI) (24,25). Both of these meta-analyses selected studies that used standardized neuropsychological test batteries to assess cognitive function, such as the MoCA or Mini-Mental Status Examination (24,25). Results from TAVI patients showed no significant cognitive changes from baseline measures 6 months after surgery (24). In contrast, cardiac valve surgery was associated with cognitive decline 6 months postoperatively, although the authors acknowledge that outcomes after 6 months are unclear (25). Comparison between these meta-analyses is difficult due to the differences in age between the patient cohorts and the level of invasiveness of these procedures (25).
Of the selected studies, only 3 utilized validated PROMs (15,16,19). The CFQ is a 25-item questionnaire developed in 1982 that is used to assess the frequency of lapses in 3 areas: perception, memory, and motor function (26). Sample questions include “Do you find you forget why you went from one part of the house to the other?” and “Do you have trouble making up your mind?”(26, p. 15) Patients rated themselves on a 5-point Likert scale of having experienced these lapses within the past 6 months (26). The higher the CFQ score, the higher the incidence of cognitive lapses (26). The CFQ has been validated as a measure of multiple dimensions of cognitive failure, although it has not been frequently used in a cardiac patient population (27). The other cognitive PROM used by Khatri and colleagues (16) was the CDS, a 39-item questionnaire developed by McNair and Kahn (28). Sample statements include, “When interrupted while reading, I have difficulty finding my place again” and “I have trouble thinking of the names of objects.”(28, pp. 142-143) Patients rated themselves on a Likert scale similar to the one found in the CFQ and in addition are asked about their cognitive experiences over the past several days. The major cognitive domains assessed with this tool were short- and long-term memory, psychomotor coordination, concentration, and attention (28). The CDS has been validated through correlations with neuropsychological test performance and has been used in several studies of patients with cardiovascular disease (29,30).
While 3 studies used the same base questionnaire, most were developed for each researcher’s specific purpose (21 -23). Accordingly, it was not possible to assess the validity and reliability of these tools. Furthermore, adding questions to existing validated tools, a methodology employed by 2 studies in the review, may also threaten the underlying reliability and validity of the original PROM (4,17,20).
It is interesting to note that in the studies selected for review, there is consistent reporting on the fact that clinical measures of objective dysfunction did not necessarily correlate with results from PROMs (15,19,21,22). There are a number of suggested possibilities for these differences. The first is sensitivity of the measures: Patients may be more sensitive to cognitive changes than clinical measures, or clinical measures may be more sensitive than the patient to cognitive changes (11,15). The second is the validity of the measures, whereby PROMs are not necessarily capturing cognitive data but instead capturing data related to changes in mood. One common finding was that patients who scored higher for depression and anxiety also reported more cognitive decline (15,16,21,22). Newman and colleagues (21) suggested that negative mood can contribute to perceptions of poor health. In other words, patients with depressed mood may focus more extensively on their cognitive failures, rating themselves as having decreased cognitive function (15). Khatri and colleagues (16) took the opposite approach by suggesting that perceived cognitive impairment may play a role in the development and maintenance of depressed moods. Presumably, depressed mood and perceived cognitive decline are interactive (15). Although these 2 concepts are representative of general issues related to the collection of PROMs, they reinforce the urgent need for new cognitive PROMs with appropriate validity and sensitivity to the cognitive changes in postsurgical cardiac patients.
Ideally, PROMs should be assessed longitudinally in order to assess changes in function and the extent of improvement or deterioration over time (1). However, only 1 study (20) evaluated patients at multiple time points postoperatively, while several studies did not assess their patient sample preoperatively (16,18,22,23). Without knowledge of the baseline cognitive function, it is difficult for health care providers to be able to interpret patient-reported changes. Assessing changes over time is further complicated by research that suggests 20% of candidates for CABG already have cognitive impairments before surgery, with age being the strongest predictor of cognitive function (31). In other words, it is possible that cognitive function could be impaired preoperatively due to long-standing cardiac or concomitant disease. As such the American Heart Association, which refers to PROMs as patient health status measures, recommends that all measures be administered at baseline and repeated at some subsequent time point (4).
The American Heart Association defines health-related quality of life (HRQoL) as the discrepancy between actual and desired functional status and overall impact of health on well-being (4). Cognitive decline has the potential to impact quality of life, negatively impact a patient’s view of their health status, and can potentially have economic impacts as well. A recent study by Garland et al (32) found that there are significant economic consequences of cardiac events such as myocardial infarction or cardiac arrest, with loss of earnings ranging from 8% to 31% for at least 3 years. If a patient’s self-reported cognitive dysfunctions impact their return to work, then this kind of earning drop can have significant impacts for patients, families, employers, and governments (32). Subjective cognitive decline has also been significantly associated with increased microvascular lesions and long-term objective cognitive decline with dementia diagnosed in 31% of CABG patients 7.5 years after surgery (10,30). The American Heart Association states that each patient is their own “gold standard” for their symptom burden, functional limitations, and HRQoL.(4, p. 2235) Patient-reported outcome measures are a reliable form of evaluating patients longitudinally and can give health care providers an accurate picture of patient clinical status while contributing to patient-centered care (1). Therefore, it is clear that PROMs that specifically evaluate cognitive function are needed.
Future Directions
This review highlights that although subjective cognitive decline after heart surgery is common, there is a lack of PROMs available that assess cognitive function. There is an opportunity for future research to either update or validate existing PROMs such as the CDS or CFQ for use within the cardiac surgical population, or for the development of a new cognitive PROM. Furthermore, a refreshed look at this issue using suitable PROMs, a formalized POCD definition, appropriate controls, and large enough sample sizes may encourage the use of PROMs in the practice setting addressing a significant knowledge gap.
Implications for Practice
Longitudinal assessment of perceived cognitive function using a PROM may be a cost-effective way to identify patients at risk of or currently experiencing POCD.
PROMs may allow health care providers to identify POCD before any objective measures have been identified and allow for earlier intervention (1).
Nurses may be in the best position to administer pre- and postsurgical PROMs.
Conclusion
The American Heart Association “advocates for the broader inclusion of patient-reported health status as a key measure of cardiovascular health in clinical research, clinical practice, and disease surveillance.” (5, p. 2345) This review was unable to identify any studies that used validated PROMs to assess cognitive function in the postoperative cardiac surgical population. Given that cognitive decline has the potential to impact not only quality of life, but the physical, mental, and emotional functioning of patients, the importance of validating and measuring cognitive functioning from the patient’s perspective pre- and post cardiac surgery cannot be overstated.
Supplemental Material
Supplemental Material, sj-docx-1-jpx-10.1177_2374373521989250 - Patient-Reported Cognitive Outcomes Following Cardiac Surgery: A Descriptive Review
Supplemental Material, sj-docx-1-jpx-10.1177_2374373521989250 for Patient-Reported Cognitive Outcomes Following Cardiac Surgery: A Descriptive Review by Amanda Robinson, Edith Pituskin and Colleen M Norris in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.