
Abstract
We conducted a retrospective cohort study using a difference-in-differences design to estimate differences in primary care outpatient clinic visit utilization among high- and low-risk Medicare aging beneficiaries from an Accountable Care Organization during the COVID-19 pandemic compared to a control cohort from the previous year. High-risk was defined as having a Hierarchical Condition Category score of 2 or higher. A total of 582 101 patient-month records were analyzed. After adjusting for patient characteristics, those in the high-risk group had 339 (95% CI [333, 345]) monthly outpatient encounters (in-person and telehealth) per 1000 patients compared to 186 (95% CI [182, 190]) in the low-risk group. This represented a 22.8% and 26.5% decline from the previous year in each group, respectively. Within each group, there was lower utilization among those who were older, male, or dually eligible for Medicaid in the high-risk group and among those who were younger, male, or non-white in the low-risk group. Telehealth use was less common among patients who were older, dually eligible for Medicaid or living in rural/suburban areas compared to urban areas. All results were significant at the 95% level. We found significant disparities based on age, gender, insurance status, and non-white race in primary care utilization during the pandemic among Medicare beneficiaries. With the exception of gender, these disparities differed between high- and low-risk groups. Interventions targeting these vulnerable groups may improve health equity in the setting of public health emergencies.
Introduction
The outbreak of the COVID-19 pandemic rapidly changed the landscape of the healthcare system and the delivery of care services worldwide (1–3). In the United States, non-COVID healthcare utilization declined by an average of 30% to 40% after the national public health emergency announcement on March 13, 2020 (4). This decline reflected an across-the-board decrease in emergency department (ED) visits (5), hospitalizations (6), acute and elective procedures (7,8), and outpatient care (9–11). Preventive and chronic disease management care utilization were subject to sharp declines of greater than 50% (12–14). In response, telehealth was rapidly adopted to provide an alternative to in-person care (15–19). The total increase in telehealth encounters in April and May 2020 has been estimated to be more than ten times the volume in March 2020 (17,19).
However, it remains unclear how older patients’ care utilization was impacted by the pandemic relative to the general population, especially those with higher baseline levels of care utilization. In addition, there may also have been a disproportionate impact of the pandemic on care utilization by historically disadvantaged groups, such as those with advanced age (86+ years), racial/ethnic minorities, low-income, disabled, and rural/suburban residents. These patient characteristics are known to be associated with limited access to care and limited adoption of new technologies such as telehealth. (3,14,20–22). Yet the extent to which telehealth accounted for total clinical encounters since the pandemic began suggests its great potential to expand access to care (10,16). Furthermore, patterns of patients’ telehealth utilization over time may provide insights into future directions to promote more equitable care access (23,24).
Telehealth expansion imposed unique challenges for older patients, who face greater technological and logistical barriers to care access (21,22,25,26). Unlike private health insurers (27,28) and other locally or privately managed public health insurers such as state Medicaid programs or Medicare Advantage (23,29,30), the Centers for Medicare & Medicaid Services (CMS) had not allowed billing for telehealth visits for traditional fee-for-service Medicare beneficiaries (ie, public health insurance covering US patients 65 years or older) before March 2020 (4). Notably, telehealth visits in traditional fee-for-service Medicare increased from 0 to nearly 1.8 million visits per week by the end of April 2021 (4). The new availability of telehealth among these Medicare beneficiaries offers a valuable opportunity to study patterns of telehealth utilization among older patients, with implications that may be relevant for non-Medicare populations beyond the United States (24,31,32).
Our study addressed these gaps in the literature with 3 objectives. First, we investigated the impacts of the pandemic on non-COVID outpatient care in primary care settings among Medicare beneficiaries served by an Accountable Care Organization (ACO) in southern Wisconsin, United States (4,17). We stratified our analysis into a high-risk group (those with a Hierarchical Condition Categories [HCC] score of 2 or higher) and a low-risk group (HCC score less than 2) (17). Second, we estimated the extent to which telehealth was able to compensate for the decline in in-person clinical visits (15,19). Third, we quantified disparities in pandemic impacts on non-COVID-related primary care outpatient visits and telehealth utilization based on patient-level characteristics (14,20).
Methods
Study Design
A difference-in-differences design was used to retrospectively estimate the change in primary care outpatient care utilization (in-person and telehealth) during the COVID-19 pandemic compared to the previous year, while controlling for the common time trends across years. Difference-in-differences is a statistical method that uses observational data to compare the difference between the change in a measured outcome in an exposed group versus the change in that outcome in a control group. In the current study, we used this method to calculate the impact of the pandemic on outpatient primary care utilization by comparing the change in care utilization within the pandemic cohort to that within the control cohort.
Data Sources and Study Sample
We analyzed claims for outpatient primary care among Medicare beneficiaries from an Accountable Care Organization (ACO) in southern Wisconsin, United States. The study sample included Medicare ACO beneficiaries who were 65 years or older with a primary care provider (PCP) within the ACO provider list. Within the study sample, the pandemic cohort was defined as those beneficiaries who were in the ACO beneficiary list in 2019 and 2020. The control cohort was defined as those who were in the list in 2018 and 2019. The 6-month study period was defined as from April 1, 2020, to September 30, 2020, for the pandemic cohort and the same months in the previous year for the control cohort (April 1, 2019, to September 30, 2019). For both cohorts, the 12 months preceding the study period were used as the baseline. March 2019 and 2020 were excluded from the study since pandemic announcements in the United States began during March 2020 and resulted in a decline in primary care outpatient visit utilization starting in mid-March 2020. As a result, monthly data on care utilization in March may yield mixed results that would not be as reflective of pandemic-related impacts compared to subsequent months (3,9).
The study sample was further stratified into a high-risk group of Medicare beneficiaries whose Hierarchical Condition Category (HCC) scores were 2 or higher, and a low-risk group of those with HCC scores less than 2. Our stratification selection is supported by the fact that high- and low-risk patients have very different care utilization patterns due to medical needs, and the high-risk population is always a targeted subgroup for care management in the ACO for quality improvement and cost control purposes (33,34). In addition, due to the difference in baseline utilization, high- and low-risk groups may also experience different pandemic impacts on care utilization (14,17).
Outcomes Measures and Explanatory Variables:
The primary outcome measure was the number of primary care outpatient care claims (both in-person and telehealth) for a beneficiary in a given month. The secondary outcome measure was a binary indicator of telehealth use. A telehealth user was defined as those in the pandemic cohort who had at least one outpatient telehealth encounter for primary care during the 6-month study period. Non-telehealth users were those in the pandemic cohort who did not use telehealth during the 6-month study period.
The major explanatory variable for outpatient care claims was the interaction between the 2 binary indicators—the study period and pandemic cohort, which captured the difference-in-differences estimates of changes in outpatient care utilization after controlling for the common time trend and the differences between the pandemic and the control cohorts. Monthly indicators were also included to control for seasonal changes over months.
For both in-person and telehealth visit claims, explanatory variables included baseline age, gender, race/ethnicity, dual Medicaid coverage, disability entitlement, rural/suburban/urban residence, and HCC scores. These variables were selected based on existing studies on health and healthcare disparities. It is expected that subgroups that are older, of non-white race, with low income and/or reside in rural areas have proportionally less resources, exposure, and access to both regular care and innovative care delivery that is highly dependent on technology and equipment, such as telehealth (3,14,20–22).
Analytical Approach
Two primary outcomes were analyzed in the study: (1) the change in outpatient primary care (in-person and telehealth) visits and (2) the use of telehealth in the pandemic cohort relative to the control cohort during the 6-month study period. For each outcome, we analyzed ACO system-wide aggregated outcomes by month and then performed a beneficiary-level regression analysis stratified by risk group (14,17) (33,34).
A negative binomial regression model was used to predict the average outpatient care encounters per beneficiary per month for each risk group. The negative binomial regression model was selected because of the outcome variable, the number of outpatient care encounters, which is a discrete variable assumed to follow a negative binomial distribution (35,36). Each beneficiary i's outpatient CareUse in month t was predicted by binary indicators of StudyPeriod, Pandemic Cohort, and their interactions, which captured the difference-in-differences estimates.

Our results were calculated as the predicted number of outpatient encounters per 1000 beneficiaries per month for the overall sample, as well as for each subgroup with the corresponding sociodemographic co-variates by risk-group. Chi-square tests were used to test the significance of the difference between the 2 risk groups for the overall change and within each sociodemographic co-variate.
For telehealth use, a logistic regression model was used to predict the likelihood of telehealth use in response to the explanatory covariates for each of the 2 risk groups. The predicted number of telehealth encounters over the 6-month study period among the pandemic cohort overall and among the subset of telehealth users were predicted by negative binominal models and presented per 1000 beneficiaries.
Results
Sample Demographics
The study sample included a total of 32 417 Medicare beneficiaries. There were 18 312 beneficiaries in the low-risk group (9554 from the pandemic cohort and 8758 from the control cohort) and 14 105 beneficiaries in the high-risk group (7202 from the pandemic and 6903 from the control cohort) (Table 1). Compared to the low-risk group, the high-risk subgroup was older (average age 77 vs 74 years), had fewer females (57% vs 64%), had a greater proportion of those with dual Medicaid coverage (9% vs 4%), disability entitlement (7% vs 2.5%), and were more likely to reside in rural/suburban versus urban areas (32% vs 29%). The high-risk group also had a higher proportion of beneficiaries with 3 or more chronic conditions (81% vs 24%), as well as higher enrollment in the ACO care management or integrated care programs (21% vs 6%) compared to the low-risk group. Within each risk group, clinical and sociodemographic factors were comparable across the pandemic and the control cohorts.
Baseline Characteristics of Pandemic and Control Cohorts by Risk Group.

Abbreviations: HCC, Hierarchical Condition Category; SD, standard deviation.
Outpatient Encounters During COVID-19
System-wide changes
The total number of primary care encounters (both in-person and telehealth) remained stable at an average of 6800 to 7000 encounters per month prior to the pandemic and decreased by about 49% in the first month after the pandemic began (3568 total encounters in April 2020). Although these encounters subsequently increased, the average monthly number of encounters over the 6-month study period was 5464 for the pandemic cohort, representing a 21.92% overall decline compared to the baseline period (Figure 1).
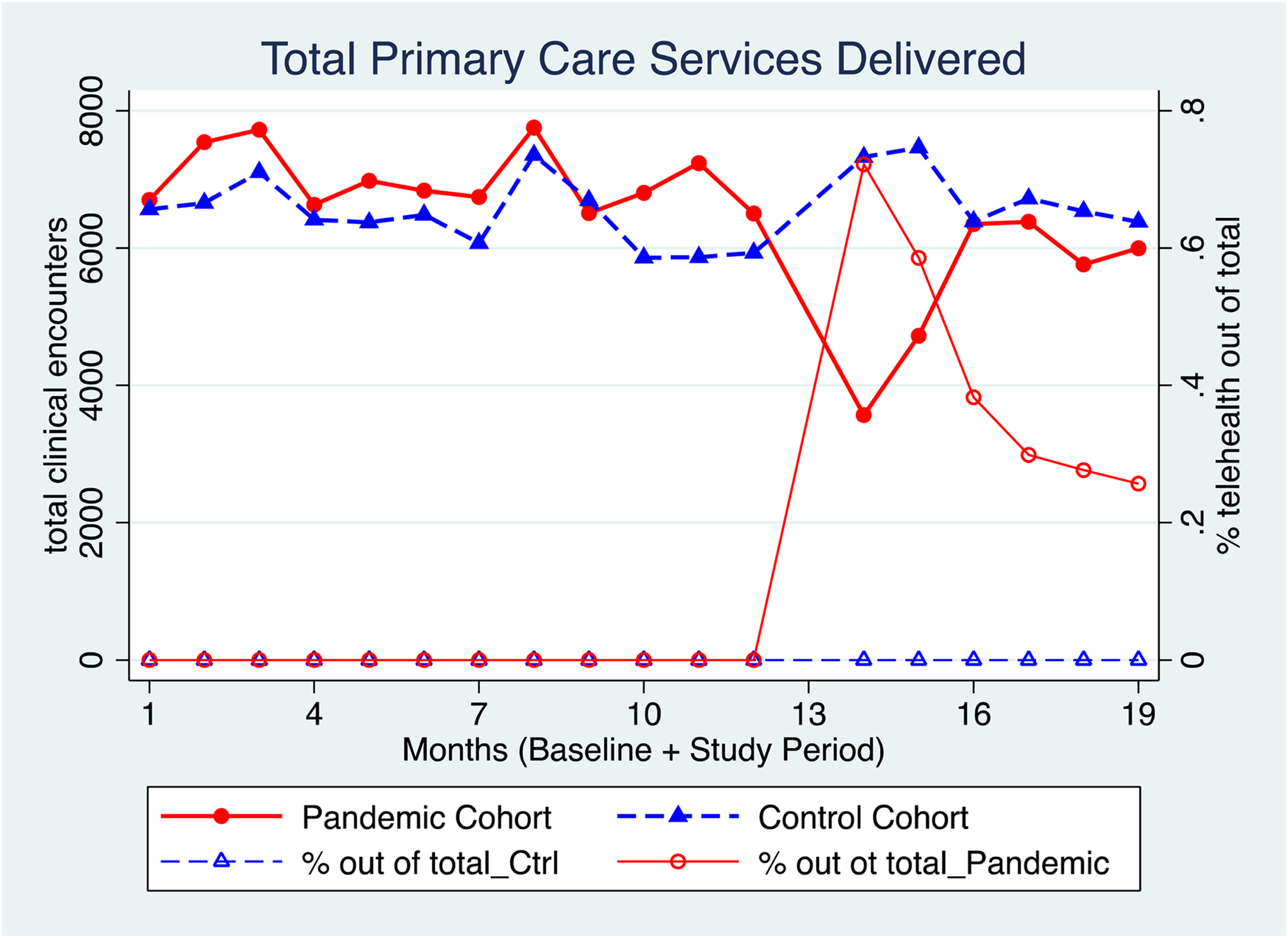
Number of primary care outpatient clinic visits and percentages of telehealth visits.
Patient-level changes
Compared to the control cohort, the pandemic cohort experienced decreased care utilization during the study period relative to the baseline for both high- and low-risk groups. The high-risk group experienced less of a decline in primary care utilization than the low-risk group during the study period (χ2 = 727.06; P < .0001). Before adjustment, the average utilization was 220 to 230 encounters per 1000 beneficiaries per month in the low-risk group and 430 to 450 encounters in the high-risk group for both pandemic and control cohorts during the baseline period. In the study period, monthly care utilization slightly increased for the control cohort compared to the baseline period with the low-risk group at 257 encounters per 1000 beneficiaries per month and the high-risk group at 439 encounters. After fully adjusting for covariates, the low-risk group in the pandemic cohort had on average 186 (95% CI [182, 190]) encounters per 1000 beneficiaries per month during the study period and the high-risk group had 339 (95% CI [335, 345]) encounters, representing a 26.5% and 22.8% decline, respectively.
Disparities in utilization based on sociodemographic factors
There were differences by age, race/ethnicity, insurance coverage, and disability in the impact of the pandemic on primary care utilization (in-person and telehealth) across low- and high-risk groups. For the low-risk group, younger age (65-74 years), male gender, and non-white race/ethnicity were associated with lower primary care utilization during the pandemic. For the high-risk group, older age (86 years or older), male gender, dual Medicaid coverage, and being non-disabled were associated with lower primary care utilization (Table 2).
Number of Primary Care Outpatient Clinic Visits (in-Person & Telehealth) per 1000 Patients per Month.

Adjusted models were estimated using negative binomial regressions. Dependent variable was the number of clinics visits (both in-person and telehealth) per 1000 beneficiaries per month. Reference groups are control cohort residents in the baseline period who are aged 65 to 74 years or female or white or non-Medicaid or nondisabled or urban. Standard deviations (SD) or robust 95% confidence interval (CI) in parentheses.
Telehealth Utilization During COVID-19
System-wide utilization and penetration
In April 2020, telehealth accounted for 78% of total primary care encounters. However, this percentage decreased to about 22% by the end of the 6-month study period in September 2020 (Figure 1). There was a small proportion of beneficiaries (8%-17%) who used telehealth each month during the study period.
Predictors of telehealth utilization
Overall telehealth use over the 6-month study period was 38% for the low-risk group and 65% for the high-risk group (Appendix Figure 1). We predicted that over the 6-month study period, there were on average 574 telehealth encounters per 1000 beneficiaries for the low-risk group and 1340 encounters per 1000 beneficiaries for the high-risk group (Table 3).
Predictors of Telehealth Use in the Pandemic Cohort by Risk Group.

Abbreviation: HCC, Hierarchical Condition Category.
*** P < .01, ** P < .05, * P < .1.
Models were estimated using logistic regressions. Dependent variable was a binary indicator of telehealth adopter (=1) or non-adopter (=0) among the pandemic cohort during the study period. Reference groups are control cohort residents in the baseline period who are aged 65 to 74 years or female or white or non-Medicaid or nondisabled or urban. Entries are odds ratios (OR). Robust 95% confidence interval (CI) or standard error (SE) in parentheses.
Differences in sociodemographic factors between telehealth users and non-users varied by risk group. In the low-risk group, telehealth users were older, more likely to be female, and more likely to have dual Medicaid coverage and disability entitlement than telehealth non-users. In the high-risk group, however, telehealth users were younger and were less likely to have Medicaid coverage than the telehealth non-users. For both high- and low-risk groups, telehealth users were more likely to reside in urban versus rural/suburban areas, had higher HCC scores, were more likely to have 3 or more chronic conditions, and hence, had a higher enrollment in the care management or integrate care programs than telehealth non-users (Appendix Table 1).
After adjustment for covariates, beneficiaries with older age (86+ years), rural or suburban residence were much less likely to be a telehealth user relative to the reference group (65-74 years old [White male without Medicaid coverage non-disabled] urban residents) (OR 0.72 95% CI [0.58, 0.89], OR 0.81 95% CI [0.70, 0.93] and OR 0.77 95% CI [0.69, 0.86]), respectively for the low-risk group. We found similar results for the high-risk group, with the odds ratios being even lower, suggesting even greater telehealth use disparities relative to the reference group.
Discussion
Main Findings
Among US Medicare ACO beneficiaries in our study, the high-risk group experienced a smaller decline in primary care outpatient utilization than the low-risk group during the pandemic. Sociodemographic factors contributed differently to the changes in utilization between these risk groups. Although there was a substantial increase in telehealth encounters, telehealth use declined significantly during the 6-month study period and did not fully mitigate the decline in in-person outpatient visits during the pandemic. Older patients, those with lower income (ie, dual Medicaid coverage), and rural/suburban residents were less likely to use telehealth.
Implications and Contributions to the Literature
Primary care outpatient utilization
Our study of Medicare beneficiaries supported findings from prior studies demonstrating that US primary care outpatient encounters experienced a sharp 30% to 40% decline once the pandemic began (3,4,19). The magnitude of the decline in care utilization was comparable to that among younger patients with private health insurance coverage and older patients with Medicare Advantage plans nationally and from other geographic locations (3,11,17). In addition, our study demonstrated 2 unique findings for Medicare beneficiaries. First, the high-risk group experienced less reduction in care utilization than the low-risk group during the pandemic (χ2 = 727.06; P < .00). Potential explanations for this include: (1) high-risk beneficiaries had greater medical needs and less flexibility to reduce care utilization discretionally than their low-risk counterparts (3,4,9), (2) more high-risk beneficiaries were enrolled in a care management program than those in the low-risk group, and (3) beneficiaries from the high-risk group were also supported and coached differently by their care team due to being in an ACO, regardless of care management program enrollment. Thus, these care management programs might have played an essential role in mitigating the impact of the pandemic through improved care coordination. Further studies on the effects of such programs during and after the pandemic will provide additional insights into these possible mechanisms. Second, our study is the first to explicitly test the impact of the pandemic on disparities with regards to sociodemographic factors among Medicare beneficiaries (14,20,25). There were differences by age, race/ethnicity, insurance coverage, and disability in the impact of the pandemic on primary care utilization (in-person and telehealth) across low- and high-risk groups.
Telehealth use
Since traditional fee-for-service Medicare did not allow reimbursement for telehealth until the pandemic began (4,29), our study was uniquely positioned to investigate the use of telehealth services among older patients. Older patients who face added challenges to adopting new technologies, yet may also stand to benefit more from using telehealth than younger patients due to challenges in obtaining transportation needed to attend in-person clinic visits. We found that despite rapid initial adoption, the proportion of outpatient encounters that used telehealth declined from 78% to 22% over the 6-month study period. The penetration of telehealth use was also low, with only 60% of beneficiaries having used telehealth during the study period. Our findings suggest that additional interventions, such as care coordination programs, as well as institutional regulations and payment models, could contribute to more equitable expansion of telehealth by engaging older and low-income Medicare beneficiaries to avoid increasing disparities in healthcare access.
Limitations
There are several limitations to our study. First, the study sample was from one healthcare system and may not be representative of the entire US Medicare population or the traditional Medicare fee-for-service beneficiaries nationally. A larger sample including multiple care systems would further address the generalizability of these findings.
Second, the study focused only on the volume of care services but did not link the services or encounters with any specific preventive care or chronic disease management activities. Short-term changes in these preventive or care management activities may have influenced our outcomes. Future studies would benefit from making such linkages to further refine our estimates (15,19).
Third, we did not differentiate between high- versus low-value care, or limit our analysis to care specific to widely-accepted quality measures. Results would then be more relevant to the best clinical practice and long-term health outcomes and care system performance.
Fourth, due to limitations in our data, this study did not explicitly account for beneficiaries’ socioeconomic and educational status, residential distance to the primary care clinics, familiarity with technology, or access to technology equipment. These factors may also be important for evaluating the impact of the COVID-19 pandemic on telehealth utilization.
Finally, regional and care system-level factors may have contributed to our findings, such as infrastructure provided to the beneficiaries to support telehealth and in-person care utilization, local culture, and logistics unique to the ACO. Future qualitative studies may provide complementary information to our quantitative study regarding the impact of patient satisfaction, as well as patient and provider experience, on disparities in telehealth utilization.
Conclusion
Among US Medicare ACO beneficiaries in our study, the high-risk group experienced a smaller decline in primary care outpatient utilization than the low-risk group during the pandemic. We also found significant disparities based on age, gender, insurance status, and non-white race in primary care utilization during the pandemic among beneficiaries. However, beneficiaries, including those in the high-risk group or dually eligible for Medicaid, were able to make use of telehealth for primary care outpatient visits, though disparities in telehealth utilization still existed. Interventions targeting these vulnerable groups may improve health equity in the setting of public health emergencies.
Footnotes
Acknowledgment
Cao, Chen and Smith are supported by the Patient-Centered Outcomes Research Institute (PCORI) HSD-1603-35039. Cao is also supported by the Wisconsin Alumni Research Foundation (WARF) AAI2989. Liu is supported by an institutional award from Research to Prevent Blindness, New York City, New York, USA to the University of Wisconsin-Madison's School of Medicine and Public Health, Department of Ophthalmology and Visual Sciences.
Authors’ Note
The University of Wisconsin-Madison Institutional Review Board does not require ethical approval for this study because it involves secondary analysis of de-identified data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research to Prevent Blindness (grant number HSD-1603-35039, AAI2989),the Patient-Centered Outcomes Research Institute (PCORI) (grant number HSD-1603-35039) and the Wisconsin Alumni Research Foundation (WARF) (grant number AAI2989).
Author Biographies
Appendix
Baseline Characteristics of Telehealth Users and Non-Telehealth Users.

| Low risk | High risk | |||
|---|---|---|---|---|
| Baseline characteristic | Telehealth users (N = 3666) | Non-Telehealth users (N = 5888) | Telehealth users (N = 4649) | Non-Telehealth users (N = 2553) |
| Sociodemographic Factors | ||||
| Mean Age (years, SD) | 74.35 (5.97) | 73.75 (5.77) | 76.57 (6.91) | 77.10 (7.23) |
| Age (years, %) | ||||
| 65-74 | 60.23 | 64.28 | 45.24 | 43.95 |
| 75-85 | 33.06 | 29.79 | 39.79 | 37.17 |
| 86+ | 6.71 | 5.93 | 14.97 | 18.88 |
| Female (%) | 64.21 | 62.81 | 56.59 | 56.72 |
| Race (%) | ||||
| Non-Hispanic White | 96.56 | 96.25 | 95.93 | 96.08 |
| Other | 3.44 | 3.75 | 4.07 | 3.92 |
| Medicaid Insurance Ever (%) | 3.71 | 3.04 | 8.32 | 10.42 |
| Disability Entitlement (%) | 2.92 | 2.02 | 7.08 | 6.58 |
| Rural/Urban (%) | ||||
| Urban | 73.35 | 68.55 | 70.34 | 62.71 |
| Suburban | 17.40 | 20.87 | 17.83 | 20.96 |
| Large town | 8.16 | 9.15 | 10.39 | 14.92 |
| Small town/isolated rural | 1.09 | 1.43 | 1.42 | 1.41 |
| Mean HCC score (SD) | 0.54 (0.50) | 0.38 (0.49) | 3.98 (2.35) | 3.41 (2.01) |
| Chronic Conditions | ||||
| 3 or more chronic conditions (%) | 33.06 | 18.89 | 84.86 | 75.44 |
| Subsample indicators | ||||
| Case management (%) | 3.98 | 2.75 | 19.01 | 15.63 |
| Integrated care (%) | 4.61 | 2.97 | 23.66 | 18.96 |
Abbreviations: HCC, Hierarchical Condition Category; SD, standard deviation.