
Abstract
We analyzed (1) the correspondence of patient and clinician perceived patient involvement in decision making and ratings made by independent observer's independent ratings, as well as (2), factors associated with patient-perceived involvement, among patients seeking hand specialty care. During 63 visits, the patient, their hand specialist, and 2 independent observers each rated patient involvement in decision making using the 9-item shared decision-making questionnaire for patients and clinicians, and the 5-item observing patient involvement scale (OPTION-5). We also measured health literacy (Newest Vital Sign), patient and visit characteristics (gender, age, race, years of education, occupation, marital status, and family present). There was no correlation (ρ = 0.17; P = .17) between patient (median 42, IQR 36-44.5) and clinician (38, IQR 35-43) ratings of patient involvement in decision making. Independently rated patient involvement correlated moderately with specialist (ρ = 0.35, P <.01), but not patient (ρ = 0.22, P = .08) ratings. The finding that patient perception of their involvement in decision making has little or no relationship to independently rated clinician communication effectiveness and effort, suggests that other aspects of the encounter—such as empathy and trust—may merit investigation as mediators of the patient agency.
Keywords
Introduction
Shared decision making (SDM) is a collaboration between patients and clinicians to arrive at a mutually agreed-upon treatment plan. It is characterized by sharing information about potential harms and potential benefits of test and treatment options, guided patient exploration of what matters most to them, and decisions that match both patient and clinician preferences (1–3). It is increasingly considered fundamental to health since it is associated with greater patient satisfaction, adherence to therapy, healthcare outcomes, and limited litigation (4–7).
To our knowledge, there is little evidence on the correspondence of patient and clinician perspectives on SDM (8). A search yielded 6 quantitative studies which used the 9-item shared decision-making questionnaire to measure patient (SDM-Q-9) and physician (SDM-Q-Doc) perception of patient involvement in decision-making. Three studies—one each in vascular surgery, anesthesiology, and dermatology—all reported differences between 7% and 39% in mean patient and physician scores but did not report correlations (9–11). One study in pediatrics and 2 in otolaryngology reported weak to moderate correlations (Spearman rho between 0.16 and 0.41) (12–14). In all 6 studies, patients rated their involvement higher than physicians. A systematic review identified several potential patient-specific facilitators and barriers of patient-perceived involvement in decision making such as age, level of education, and ethnic background (15), but the findings were not consistent across studies. It would be helpful to better understand discordance between patient and clinician perceptions, concordance with independent ratings of SDM, and factors associated with patient-perceived involvement in decision making, in a field like hand surgery where multiple discretionary test and treatment options are available for most conditions, and the choice largely depends on patient preferences based on what matters most to them (their values) (8,16–19). The findings of this type of inquiry might help clinicians adapt their communication strategies in order to improve patient engagement and participation.
This study measured (1) the correspondence of patient and clinician perceived patient involvement in decision making and ratings made by independent observer's independent ratings, as well as (2) factors associated with patient-perceived involvement, among people seeking hand specialty care.
Methods
Study Design
This study is a secondary analysis of a prospective cohort of adult patients visiting one of 3 hand surgeons for a new problem at a secondary care center in the Netherlands. Every new patient fluent in Dutch and able to provide informed consent was informed of the study aims and requirements for participation by a researcher prior to the visit. Patients that agreed to participate signed an informed consent prior to the visit. The study design was approved by the medical ethics committee. Visits of patients who had no prior treatment for their current problem, and visits where at least 2 treatment options were available (including no intervention) were initially included. We refer to our previous paper for a detailed overview of the study design and outcome choices as well as a detailed overview of the included diagnoses (20). Enrollments took place between November 2019 and March 2020 after which enrollments were put on hold due to the pandemic. For this secondary analysis, we excluded 5 of the initially included 68 visits from the initial cohort since the 9-Item Shared Decision-Making Questionnaire was not completed by both patients and clinicians, which are the primary endpoints for this study. Sixty-three patients were used for analysis.
Outcomes
After obtaining informed consent, patients completed a questionnaire including demographics (gender, age, race, years of education, occupation, and marital status) and a validated Dutch version of the Newest Vital Sign (NVS) Health Literacy Test (Cronbach's alpha = 0.76) was administered (21). The NVS health literacy test is based on an ice cream nutrition label and results in an overall score ranging from 0 to 6. As in the original NVS study, we separated the resulting NVS scores into inadequate (0-3) and adequate (4-6) health literacy (22).
After the visit, patients (SDM-Q-9) and clinicians (SDM-Q-Doc) were asked to complete the 9-Item Shared Decision-Making Questionnaire. The SDM-Q-9 instruments are widely used, reliable and validated questionnaires (Cronbach's alpha SDM-Q-9 0.88; SDM-Q-Doc 0.87) (23) consisting of 9-items that quantify the patient and clinician perception of patient involvement in decision making (24–26). The items (eg, item 1: “My doctor made clear that a decision needs to be made” [patient], “I made it clear to my patient that a decision needs to be made” [clinician]) are scored on a 6-point Likert-scale ranging from “completely disagree” (0) to “completely agree” (5), with a maximum score of 45. Visits were audio-recorded to independently assess observed patient involvement in decision-making using the validated OPTION-5 instrument (moderate positive correlation with OPTION-12, r = .61 (95% CI 0.54-0.68) and a strong positive correlation of repeat ratings, r = .93 (0.83-0.97) (27). Patients were advised that the study evaluated patient–clinician communication without giving further details to minimize alternations in behavior. Clinicians knew they would be audio-recorded and were informed that the audiotapes would be used to assess patient–clinician communication. They received no training in shared decision making. OPTION (5) is used to rate the effort of a clinician to involve a patient in a discussion of treatment options based on 5 items (27–29). Each item is rated on a 5-point Likert-scale ranging from “no effort” (0) to “exemplary effort” (4) with a maximum score of 20. Two researchers trained to use the OPTION 5 tool and scored audio recordings. Both raters independently coded 10 randomly selected consultations with a moderate agreement (kappa = 0.67) (10,30–32). The raters discussed discrepancies in their interpretations of the scoring and then rated another set of 10 consultations with the strong agreement (kappa = 0.80).
Study population
We enrolled 30 (48%) men and 33 women with a mean (SD) age of 54 (20) years (Table 1). Almost all patients were White (92%), half were employed (52%), and almost half were married (44%). The mean (SD) educational experience was 15 (3.0) years. Two-third of the visits addressed nontraumatic conditions (64%; Appendix 1). Most patients came alone without a family member present (68%) and the mean (SD) visit duration was 9.0 (3.3) minutes. Nearly half of the patients had inadequate health literacy (44%). Three male hand surgeons participated in this study (Table 2).
Patient and Clinical Characteristics (N = 63).

Data for continuous variables are presented as the mean ± standard deviation, with the range in parentheses
Data for discrete variables are presented as the number of patients, with the percentage of total patients seen in parentheses
Clinician Characteristics.

Data for discrete variables are presented as the number of patients per clinician, with the percentage of total patients seen in parentheses.
Data for continuous variables are presented as the mean ± standard deviation, with the range in parentheses.
Statistical Analysis
An a priori power analysis indicated that 84 patients provide 80% power to demonstrate an at least moderate correlation of 0.3 between the SDM-Q-9 and SDM-Q-Doc at a significance level of 0.05. We had to prematurely stop enrollments due to the pandemic. In the analysis of data collected, we found a small correlation that would need 250 patients to reach statistical significance, which in our opinion is a clinically irrelevant association. Therefore, we closed the study and completed the analysis with 63 patients.
For variables with nonnormal distributions, we present median and interquartile ranges. Spearman correlations were used to evaluate relationships between SDM-Q-9, SDM-Q-doc, and OPTION (5) scores. The association of explanatory variables with SDM-Q-9 scores was assessed using Mann-Whitney U-test for dichotomous variables, Kruskal-Wallis test for categorical variables, and Spearman correlation coefficients for continuous variables. A Bland-Altman plot was also used to measure agreement between SDM-Q-9 and SDM-Q-Doc scores by noting systematic differences and magnitude of variation between the 2 scores across the range of scores, converted to a 0-100 scale for more intuitive visualization (Figure 1B). When the data on a maximum of 2 items of the SDM-Q questionnaires were missing, these missing items were imputed with the mean score per question of the entire SDM-Q questionnaire. The level of significance was set at P < .05. Statistical analysis was performed with R version 3.6.3.
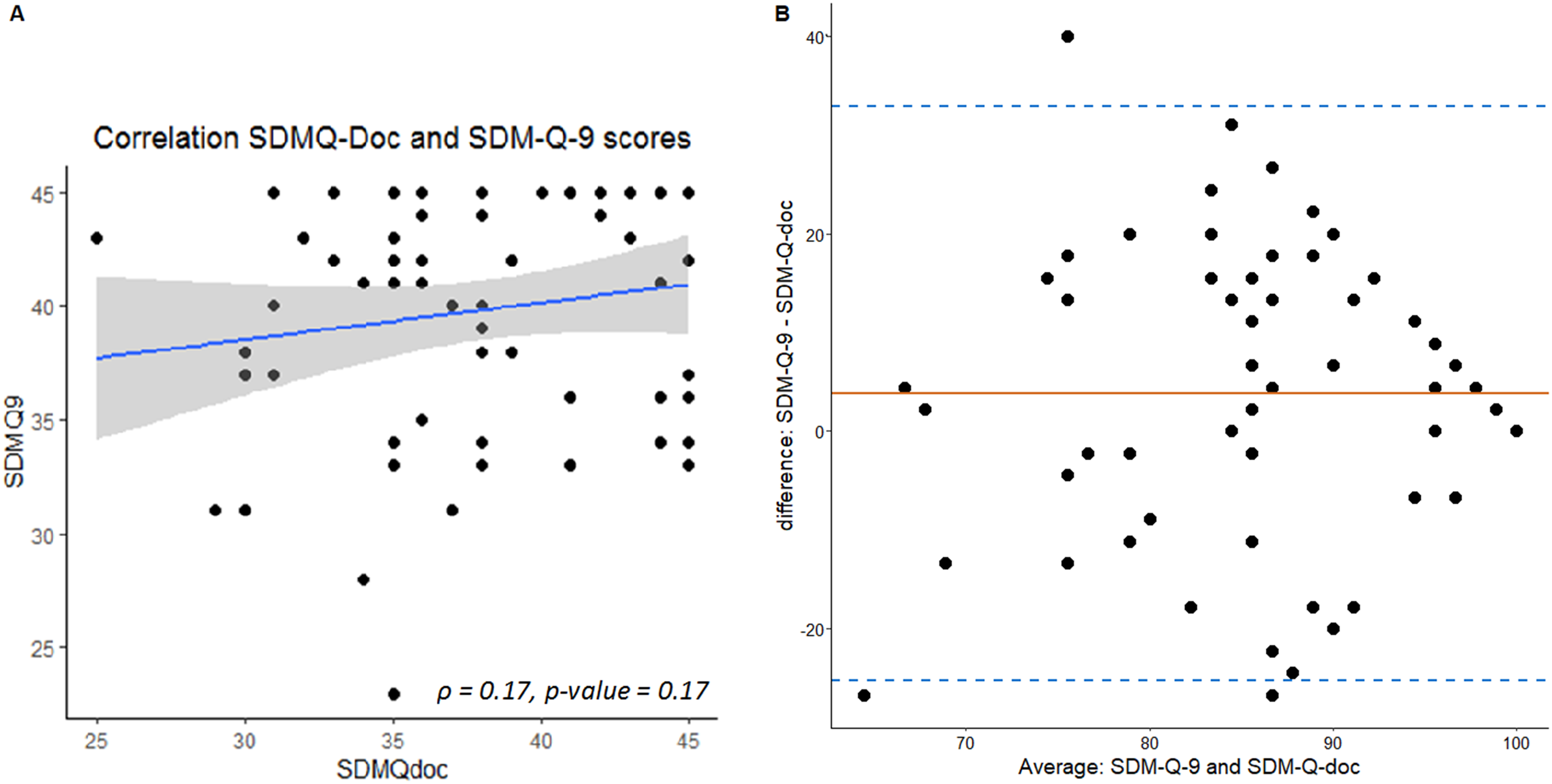
Correlation plot with SDM-Q-9 scores on the y-axis and SDM-Q-Doc scores on the x-axis. The blue line indicates the correlation.
Results
Correlation of Patient and Clinician Perception of Patient Involvement in Decisions
There was no correlation between the patient and clinician ratings of patient involvement in decision making (median [IQR] SDM scores: 42 [36-44.5] for patients, 38 [35-43] for clinicians; ρ = 0.17; P = .17; Figure 1A). When comparing individual items, only item 3 (discussing the availability of more than one treatment option) had a moderate correlation (ρ = 0.30, P = .02) between questionnaires (Appendix 2).
Correlation of Patient and Clinician Assessment of Patient Involvement in Decisions and Independent Rating of Specialist Communication Effectiveness
Independent ratings of shared decision making (OPTION (5) scores) correlated moderately with clinician perception of patient involvement (SDM-Q-Doc; ρ = 0.35, P < .01), But not with patient perception of their involvement (SDM-Q-9; ρ = 0.22, P = .08; Table 3).
Comparison of Observed (OPTION (5)) and Perceived (SDM-Q) Levels of SDM.

Data for continuous variables are presented as the mean ± standard deviation, with the range in parentheses.
Factors Associated With Patient Perception of Their Involvement in Decisions
In bivariate analysis, older age (ρ = 0.40, P = < .01), women (41 ± 4 vs 38 ± 6; 95% CI 0.21-5.30; P = .047), inadequate health literacy (45 [34-42] vs 37 [42-45]; 95% CI 3.39-7.84; P = < .01), fewer years of education (ρ = −0.37, P = < .01), and being married (41 ± 4 vs 39 ± 5; 95% CI 0.37-5.47; P = .02) were associated with higher patient perception of involvement in decision making (Table 4).
Bivariate Analysis of SDM-Q-9 Scores per Independent Variable.

Data for dichotomous variables are presented as mean ± standard deviation or median (IQR).
Data for continuous variables are presented as correlation values.
Indicates a P-value below .05.
Discussion and Conclusion
Discussion
Introduction
Patient involvement in the discussion of treatment options is considered beneficial (4–7), especially in a field such as hand specialty care where most tests and treatments are discretionary. This is a good setting to analyze the correspondence of patient and physician ratings of patient involvement in decisions and independent ratings of clinician involvement of patients. We studied (1) the correspondence of patient and clinician perception of patient involvement in decision making and ratings made by independent observer’s independent ratings, as well as (2) factors associated with patient-perceived involvement.
Limitations
Limitations of our research can be considered. First, only 3 male surgeons with clinical experience as a specialist of 1.5 to 6 years participated in this study, which may limit generalizability. Studies show that women clinicians are more participatory in terms of empathy and information sharing (33,34). It can also be argued that more experienced clinicians might be better at reading patient signals, using strategies to increase patient participation, and detecting signals from the patient that they have not understood the information. In addition, the patients were mostly White, and societal and cultural context might be important. On the other hand, the finding that patient and clinician perceptions of patient involvement are discordant is in line with other studies on the topic (35,36), and the discordance between independent ratings and patient and clinician ratings was also observed in another study (10). Second, we had to prematurely stop enrollment due to the pandemic before reaching our enrollment target. However, based on the data we had when enrollment was paused, we would need 250 patients to demonstrate significance, which we interpreted as a difference that would be unlikely to be important to patients and clinicians. Third, the smaller sample is at greater risk of overfitting and biased estimates in multivariable analysis. In our opinion, the observed associations have sufficiently strong associations that they seem reliable. Fourth, both patient and clinician were aware they were being audio-recorded—and clinicians were aware of the study aims—which might have altered behavior (37). On the other hand, there is evidence that being audio recorded does not appreciably influence behavior (38–40). Fifth, patient involvement in decision making is complex and can only be partially measured using questionnaires (41). This partial measurement should provide useful information.
Discussion
The finding of no (or at most a very small) correlation between patient and clinician ratings of the patient's involvement is consistent with similar studies in pediatrics (r = .16; P = .12) and otolaryngology (r = .24; P < .01 and r = .23; P < .05) (12–14). One study included cancer survivors with many visits over an extensive period and reported a moderate correlation (r = .41; P < .01) (26). It is possible that the more developed relationship between patient and clinician contributed to greater concordance. The finding that the only individual item that correlated (item 3) addressed the discussion that there are multiple treatment options was observed in other studies. Fiks et al (8) interviewed 60 parents of children with ADHD and 30 clinicians and found that clinicians tended to view the interaction as an attempt to convince parents to follow their recommendations, while parents viewed it as a collaborative partnership.
The observation that clinician ratings of patient involvement correlated moderately with independent ratings, while patient scores did not correlate, suggests that factors other than the involvement of patients in the decision-making process may be responsible for greater patient feelings of involvement. For instance, patients might answer questions about involvement in decision making in terms of their satisfaction with the consultation or the clinician, which—evidence suggests—may be driven largely by a sense that the clinician takes a genuine interest in them (emotional) rather than aspects of decision making (rational) (9,42–48). There is evidence that greater patient-perceived involvement in decision making is associated with greater trust in the clinician (49–51). Studies of communication training tools for clinicians and communication aids for patients suggest training clinicians is more effective than decision-making tools for patients, but neither improves patient experience (52–57). For instance, one trial in oncology randomized clinicians to receive SDM communication skills training or not, and patients to receive a communication aid or not. They found training clinicians had a large positive effect (Cohen's d = 1.12) on independent ratings of SDM using the OPTION12 tool and a positive effect (d = 0.73) on patient-perceived involvement using the SDM-9-Q. The patient communication aid did not improve independent SDM ratings. The interventions had no effect on patient or oncologist satisfaction with the consultation, decisional conflict, quality of life, consultation duration, or the decision made (55).
The finding that older age, women, inadequate health literacy, fewer years of education, and being married were associated with higher patient ratings of their involvement in decisions, is in contrast with a study conducted in America that found that older age, inadequate health literacy, and inadequate language proficiency are associated with lower perceived patient involvement (49). They used a different method to measure patient involvement and over a period of 12 months in multiple consecutive outpatient visits. Three studies conducted in China also contradict our findings as they report greater patient-perceived involvement in SDM in patients with adequate health literacy (58–60). The questions in the Chinese version of the SDM-Q-9 questionnaire seem to be focused on measuring how actively patients thought they contributed to the SDM process, rather than measuring how patients perceived the level of SDM that was present during the consultation. Both the American and Chinese studies used different measures, which perhaps explain these contrasts. Our patients with lower health literacy might be relatively deferential, wanting to express their appreciation across the power hierarchy with the clinician. The relationship between health literacy and perceived involvement in decision-making is still uncertain and merits additional study.
Conclusion
In musculoskeletal specialty care—where tests and treatments are largely discretionary and the choice depends on what matters most to a patient—patient perceived involvement may be influenced by factors other than effective clinician communication and effort as graded using the OPTION tool. That tool focuses more on the rational rather than the relationship aspects of the interaction. Evidence to date suggests patient trust in the clinician (feeling comfortable enough, to be honest with the physician) and perceived physician empathy are associated with increased patient-rating of their involvement in decision making (49,51). Future qualitative and quantitative studies might evaluate the potential benefits of improved clinician communication strategies and empathetic approaches that nurture trust in patient engagement in developing their health strategies.
Practice implications
Involved patients are more likely to make decisions based on their preferences, less clouded by common misconceptions, and less influenced by the clinician's bias (8,10,50). Clinicians might focus not only on the rational aspects of guiding a patient through decision making, but also on tactics for creating a safe environment for patients to explore their values and their preferences and take agency for their health.
Footnotes
Appendix 1
List of Encountered Diagnoses of Included Patients (n = 63).

| Diagnosis | Percentage a | Number |
|---|---|---|
| Carpal tunnel syndrome | 6% | 9 |
| Tendovaginitis stenosans (trigger finger) | 5% | 8 |
| Metacarpal fracture | 4% | 6 |
| Dupuytren | 3% | 4 |
| Distal radial fracture | 3% | 4 |
| Carpalmetacarpal arthritis | 3% | 4 |
| Phalanx fracture | 2% | 3 |
| Ganglion cyst of wrist | 2% | 2 |
| Radiocarpal arthritis | 2% | 2 |
| Midcarpal instability | 2% | 2 |
| Carpal tunnel syndrome & tendovaginitis stenosans | 2% | 2 |
| De Quervain’s tenosynovitis | 1% | 1 |
| Distal radial fracture and ulna styloid fracture | 1% | 1 |
| Post-traumatic elbow arthritis | 1% | 1 |
| Nonunion distal radius | 1% | 1 |
| Nonunion of finger fracture | 1% | 1 |
| Distortion of distal interphalangeal joint | 1% | 1 |
| Pyogenic granuloma | 1% | 1 |
| Arthritis of the distal radial ulnar joint | 1% | 1 |
| Carpometacarpal arthritis and carpal tunnel syndrome | 1% | 1 |
| Finger contusion | 1% | 1 |
| Rupture of the extensor digitorum communis tendon | 1% | 1 |
| Digital mucous cyst | 1% | 1 |
| Phalangeal and metacarpal fracture | 1% | 1 |
| Post-operative residual symptoms | 1% | 1 |
| Wrist mass or lump | 1% | 1 |
| Hyper mobile thumb | 1% | 1 |
| Rectus diastase | 1% | 1 |
Percentages are rounded to full numbers.
Appendix 2
Differences of Patient and Clinician SDM-Q Scores per Item and Correlation Analysis.

| Simplified descriptive of SDM-Q-9/Doc items | Patients | Clinicians | Correlation | |
|---|---|---|---|---|
| Mean ± Sd a | Mean ± Sd a | Spearman rho | P-value | |
| Item 1: Informing a decision needs to be made | 4.44 ± 0.64 | 4.33 ± 0.82 | 0.09 | .47 |
| Item 2: Investigating patients preferred involvement | 4.14 ± 1.08 | 3.76 ± 0.93 | 0.11 | .40 |
| Item 3: Stating there are multiple treatment options | 4.40 ± 1.10 | 4.24 ± 1.10 | 0.30 | .02* |
| Item 4: Clarifying pros and cons | 4.52 ± 0.67 | 4.13 ± 0.91 | 0.004 | .97 |
| Item 5: Investigating patients understanding | 4.59 ± 0.56 | 4.38 ± 0.61 | 0.16 | .20 |
| Item 6: Identification of patient’s preference | 4.26 ± 1.05 | 4.00 ± 1.02 | 0.14 | .28 |
| Item 7: Weighing all treatment options | 4.35 ± 0.94 | 4.32 ± 0.64 | 0.09 | .47 |
| Item 8: Reaching a shared decision | 4.43 ± 1.07 | 4.32 ± 0.80 | −0.02 | .88 |
| Item 9: Agree upon follow up arrangements | 4.67 ± 0.76 | 4.60 ± 0.64 | −0.03 | .83 |
Each item on both versions is ranged by a Likert scale from 0 to 5.
*Only significant correlation, significance is set at a P-value < .05.
Disclosures
BTH, LXR, XJ, GS, and MH certify that they have no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article. One of the authors (DR) certifies that he, or a member of his immediate family, has or may receive payment or benefits from Skeletal Dynamics (USD < 100 000, Wright Medical for elbow implants (USD < 10 000), the Deputy Editor for Clinical Orthopaedics and Related Research, Universities, and Hospitals, and Lawyers outside of the submitted work.
Highlights
Patient and clinician perception of patient involvement in decision making. 5-item observing patient involvement instrument (OPTION5). 9-item Shared decision-making questionnaire (SDM-Q). Health literacy (Newest Vital Sign). Clinician training programs in motivational interviewing.
Author Statement
Luke X. van Rossenberg: Conceptualization, Methodology, Investigation, Formal analysis, Visualization, Writing—Original Draft; Bastiaan T. van Hoorn: Methodology, Formal analysis, Writing—Review & Editing; David Ring: Validation, Writing—Review & Editing; Xander Jacobs: Investigation, Resources; George Sulkers: Investigation, Resources; Mark van Heijl: Investigation, Validation, Supervision.
Declaration of Conflicting Interests
All ICMJE Conflict of Interest Forms for authors are on file with the publication and can be viewed on request.
Each author certifies that his institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Ethics Statement
Each author certifies that his institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Ethical Approval
Ethical approval to report this case was obtained from medical research ethical committees united R19.077.
Statement of Human and Animal rights
All procedures in this study were conducted in accordance with the medical research ethical committees united. Approved protocols R19.077.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Statement of Work
The work was performed at the Diakonessenhuis Utrecht, affiliated with the Medical University of Utrecht, Utrecht, the Netherlands.