
Abstract
Diabetes group visits (GVs) have been shown to improve glycemic control and quality of care. However, little is known about the patient and clinician experience. We trained staff to conduct a 6-month GV intervention at six community health centers (CHCs) for adults with uncontrolled diabetes. Patient satisfaction was analyzed using postintervention surveys. Clinician satisfaction was analyzed through pre and posttraining surveys and 1:1 semistructured interviews. Twenty-seven staff and clinicians were trained. Fifty-one adult patients were enrolled and 90% reported high satisfaction with the program. Patients enjoyed longer visits with peer support and felt better equipped to manage barriers to diabetes control. 88% of staff reported that they enjoyed taking part in the program and noted improved team morale, professional development, and increased interdisciplinary collaboration. Perceived challenges of GVs included time investment for a new program, integration into workflow, and staff turnover. Patient and staff satisfaction was high across multiple domains. Staff noted many benefits but reported challenges with patient recruitment and retention as well as the time needed to implement GVs.
Introduction
Thirteen percent of U.S. adults carry a diagnosis of diabetes (1). Group visits (GVs), shared appointments that include both group education and individual medical visits, are one way to empower patients with self-management strategies (2,3). GVs can improve glycemic control, diabetes knowledge (4–10), and quality of life (7,11). Patients also benefit from increased face time with their clinician and more in-depth diabetes education (2). At a system level, GVs have been shown to decrease ED visits, specialist visits, and hospitalizations (4,5,8,11,12).
The Triple Aim of enhancing patient experience, improving population health, and reducing costs are accepted as a way to optimize healthcare delivery with a suggested (13) fourth aim of improving the work life of health care providers (14,15). Taking on new quality improvement projects may add to staff workload and burnout (16). To achieve the Quadruple Aim with GVs, we must have a better understanding of the clinician and staff experience with this model of care as they will play a critical role in implementing and sustaining it. Based on two recent reviews of group visits, data on clinician satisfaction with GVs appear generally positive (17) but is extremely limited (9,18).
Several older studies suggest that patients also have high overall satisfaction with GVs, perhaps related to improved perceptions of coordination of care and culturally competent care (17,19,20). One study noted that patients enjoyed peer support and having a longer visit; however, a formal analysis of these measures was not conducted (2). Additionally, these studies were single-center trials and did not evaluate patient perceptions of specific aspects of GVs such as peer support, knowledge gained, or confidence in addressing barriers to successful management. Also, few GV studies have been conducted in the community health center (CHC) setting, an important network of clinics that provides primary care to one in eleven Americans and serves a diverse and medically underserved population (21). This underserved group of patients is at high risk for poor glycemic control and subsequent complications (22).
We conducted a study of GVs at six community health centers (CHCs) in the Midwest. Our program has been previously shown to improve hemoglobin A1C, healthful eating habits, and levels of diabetes distress (23). Here, we will examine patient and clinician satisfaction with GVs from this multisite study. Our aim is to understand which aspects of group visits patients found most beneficial and to characterize clinicians’ reported benefits and barriers to implementation to facilitate the real-world adoption of GVs.
Research Design and Methodology
We conducted a prospective study in which CHC staff implemented a 6-month GV program at their sites. The academic team from University of Chicago partnered with the Midwest Clinicians’ Network (MWCN), a member organization of more than 120 CHCs in 10 Midwest states, in conducting this study. The University of Chicago Institutional Review Board approved all study procedures, and this study was registered at clinicaltrials.gov (NCT02347514).
Recruitment and Training
CHCs were recruited through the MWCN. To be eligible, a CHC had to assemble a team of three to four clinicians and staff to organize the GVs; it was required that at least one team member from each CHC be a medical provider (advanced practice nurse, physician assistant, or physician). Twenty-seven total staff from seven sites at six CHCs (three urban, three rural) located in Ohio, Nebraska, Michigan, Illinois, and Indiana enrolled in the study and were invited to a one-and-a-half day in-person Learning Session in Chicago. Staff from the University of Chicago and MWCN trained attendees on the structure and implementation of GVs, strategies for patient and staff recruitment, and barriers to implementation. There was a second one-and-a-half day Learning Session during the implementation of GVs. In addition to in-person training, we organized 16 monthly webinars to review educational objectives, answer questions and share experiences among the sites. Of the seven teams recruited, one dropped out after the first learning session and before implementing GVs due to the team leader retiring, and one team completed only one GV; the remaining five teams completed the six GVs as planned. Our staff training is described in more detail in a previously published manuscript (24).
Group Visit Structure
Patients were recruited by their CHC. Inclusion criteria were: age ≥18, English or Spanish speaking, most recent hemoglobin A1C ≥8% and active in the clinic (≥2 visits in the past year and ≥1 visit in the past 6 months). Exclusion criteria were: pregnancy, uncontrolled psychiatric problem, dementia, cognitive impairment, hearing impairment, or severe physical disability barring participation (e.g., homebound) as these may pose barriers to the attendance of GVs and benefit from group activities. A patient's primary care provider (PCP) could also exclude them if they were deemed unlikely to benefit. Written informed consent was obtained from all patients, clinicians, and staff.
GVs were conducted monthly for six months with a goal of 8–10 patients per group and had a median visit length of 120 min. Each GV included an individual medical exam, group diabetes education led by either a staff member or guest speaker and a facilitator-led discussion to review information, assess goals and encourage peer support. Formal training from the University of Chicago included a framework for the visits. Publicly available sample diabetes education curricula were provided; sites could elect to use these or choose other resources.
Measures: Patient Satisfaction
CHC staff surveyed patients before the initial group visit and again at the completion of the six-month program. The baseline survey included demographics and diabetes-related health history. A baseline chart abstraction was conducted to obtain baseline glycosylated hemoglobin (A1C), blood pressure, low-density lipoprotein (LDL), and body mass index (BMI). Since no validated scales exist to measure patient and staff satisfaction with group visits, we developed survey questions to assess patient and staff satisfaction based on a literature review, previous group visit studies we have conducted, and site visits to clinics with experience implementing them. The domains of the surveys were based on the Consolidated Framework for Implementation Research (25). Questions were iteratively revised through pilot testing with researchers at the University of Chicago and assessed for external validity through input and review from health center stakeholders. The six-month survey assessed overall satisfaction with the program and included questions about specific aspects of GVs such as length of the visit, patients’ preference for their PCP as the group leader, and their perception of improvement in health due to GVs (Supplemental 1). Patients answered questions on a four-point Likert-type scale of “Not at all,” “A Little,” “Some,” and “A Lot.” Patient surveys were administered on paper and then entered in REDCap.
Measures: Clinician Satisfaction
Staff were surveyed before the first training session (electronic survey via REDCap) and then again after the second training session six months later (paper survey). Survey questions were designed to evaluate the impact of GVs on clinicians, the CHC itself, and community perceptions of the CHC (Supplemental 2). Clinicians rated their level of agreement with statements using a five-point Likert scale of “Strongly Disagree,” “Disagree,” “Neither Disagree nor Agree,” “Agree,” and “Strongly Agree.”
Clinician interviews were conducted twice: first, three months after the initial training (as GVs were underway) and then again at the conclusion of the GVs. All staff and clinicians were invited for the first round; for the second round, only the team champion and one other team member were invited to interview. All five subdomains of the Consolidated Framework for Integrated Research (25) were used to develop interview questions. Forty-five minute semi-structured interviews were conducted over the telephone by trained research staff. All interviews were audio-recorded. A professional company then transcribed interviews verbatim.
Analysis: Patient Satisfaction (Survey Data)
Descriptive statistics were assessed for patient survey data and demographic data.
Analysis: Clinician Satisfaction (Survey and Interview Data)
Descriptive statistics were assessed on survey data. For the qualitative analysis, four investigators used a modified Template Analysis, using the interview guide to create an initial codebook used to analyze interview transcripts (26). The transcripts were then distributed randomly to pairs of reviewers; each member of the pair would independently code a transcript and subsequently meet with their partner to discuss to consensus and modify the initial codebook as indicated by their theme coding. HyperResearch software version 4.0.0 was used to organize and code the interview data. Codes related to the benefits and challenges of group visits were analyzed for specific sub-themes pertaining to satisfaction with the GV program. These sub-themes were organized into benefits for patients, clinicians, and the CHC. Challenges of the program were also identified.
Results
Patient Satisfaction: Survey Results
A total of 51 patients were enrolled. Table 1 describes patient demographics and baseline health status. Forty-five patients completed the baseline survey and 30 patients completed the six-month survey. Characteristics of the survey responders and nonresponders were generally similar although a higher proportion of low-income, Medicaid insured and Black patients did not respond while a higher proportion of Spanish-speaking patients did respond; exact percentages are noted in Supplemental 3. Overall, 90% of patients reported high satisfaction with the program (Figure 1). Fifty-three percent reported “a lot” of support from other participants and 45% learned “a lot” about diabetes management from the other members of the group. Sixty-seven percent felt more confident in managing their diabetes and 73% reported that their diabetes was better managed because of the group visits. Seventy-seven percent appreciated having a longer visit and 87% felt that the group visits were an effective use of their time. About two-fifths of patients would have strongly preferred that their PCP be the group leader (39%, “A Lot”), two-fifths were ambivalent (39%, “Some”), and one-fifth did not feel strongly (22%, “A Little” or “Not at all”). The vast majority reported that they did not find the group visits burdensome or boring. About a quarter (24%) of the patients surveyed reported difficulty in attending class; commonly cited challenges were transportation and childcare.
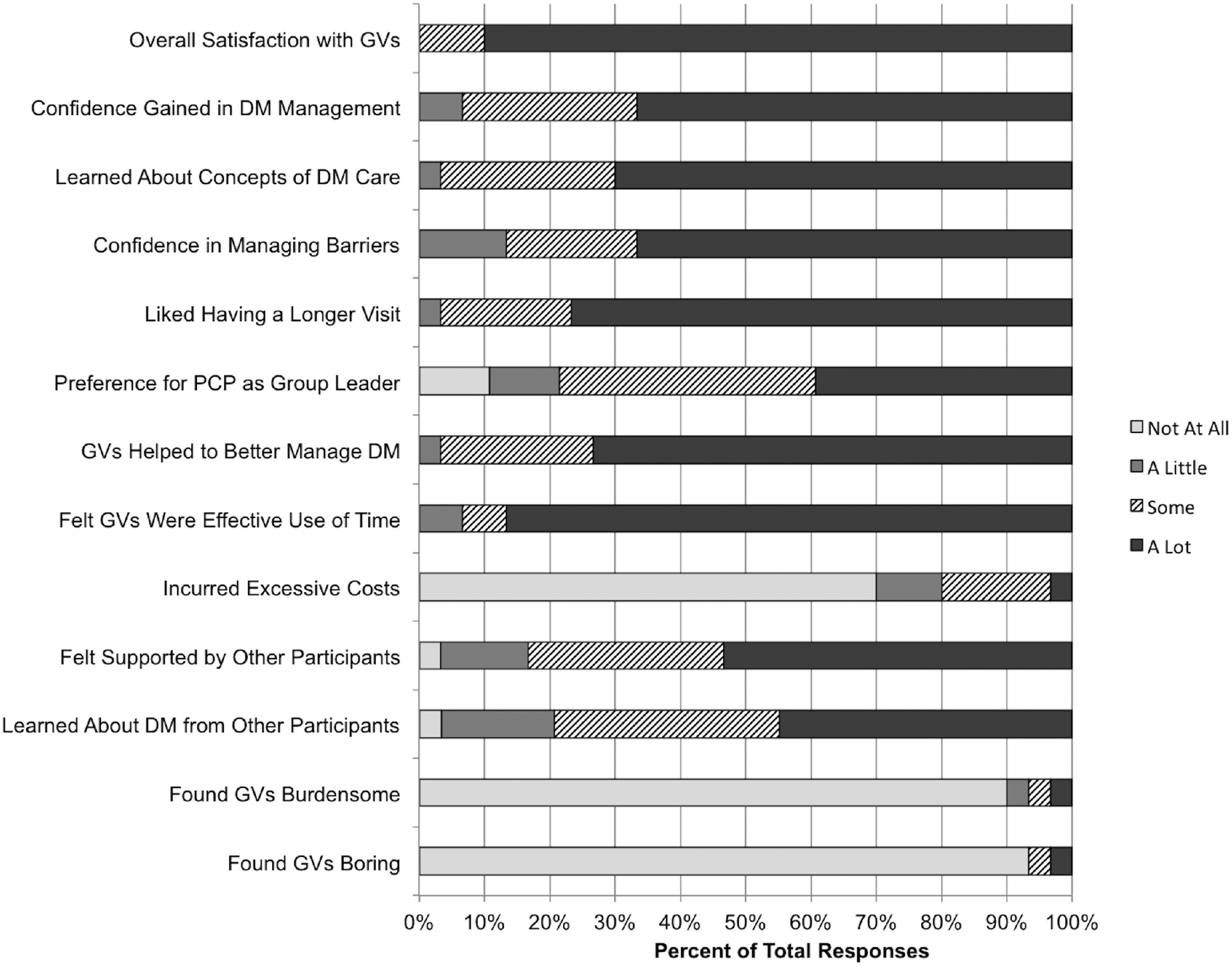
Patient satisfaction with diabetes group visits at six months (n = 30).
Baseline Characteristics of Patients (N = 51)a and Clinicians (N = 27)b.

Data not available for every patient for each metric, thus n < 51 for some metrics.
Some staff answered more than one role.
Clinician Satisfaction: Survey and Interview Results
Twenty-seven clinicians with a variety of professional backgrounds were enrolled in the group visit program (Table 1); 18 of these completed the 6-month survey. Characteristics of the survey responders and nonresponders were generally similar and are noted in Supplemental 3. Thirteen clinicians participated in the first round of interviews and seven clinicians were interviewed a second time. Clinicians noted several benefits to patients, health center staff, and the health center itself (Table 2).
Selected Clinician Quotes Related to Perceived Benefits and Challenges of Group Visits.

Clinicians perceived social support to be a major benefit of GVs for their patients, frequently commenting on the camaraderie built during GVs:
They would support each other, they encouraged each other, they tried to hold each other accountable; it was a really good dynamic.
Clinicians felt that patients had improved diabetes knowledge due to high quality education in the GVs, specifically regarding diabetic foot care, insulin administration, nutrition, and weight loss. All clinicians felt that GVs could increase patient confidence in managing their disease (Figure 2). GVs seemed to motivate and empower patients to take control of their own health:
The biggest benefit is just engaging the patients and getting them more interested in taking part in their health care.

Clinician satisfaction with group visits at 6 months (n = 18).
Clinicians noted that a longer visit better addressed detailed aspects of diabetes care by allowing more time for questions. They felt that GVs provided a high level of attention which patients perceived as increased prioritization of their care. Seventeen out of eighteen felt that GVs could increase patient satisfaction and improve efficiency in patient care.
Clinicians also perceived benefits of GVs for themselves including improved team morale, professional development, and increased inter-professional collaboration. They reported that they thoroughly enjoyed taking part in the program with 88% (16 of 18) reporting that GVs could increase staff morale and all but one saying that GVs could deepen clinicians’ relationships with their patients. They appreciated the opportunity to grow as leaders by implementing a new program and gained a better appreciation for other team members’ roles; 94% (17 of 18) felt that GVs could increase multidisciplinary collaboration. They also appreciated a space to focus on one medical problem in-depth. Clinicians felt that GVs could improve the use of CHC resources (89%, 16 of 18) and coordination of care (83%, 15 of 18).
At the health center level, clinicians felt that GVs communicated to patients the CHC's commitment to them:
It has showed [patients] that the center is really interested in helping them with this disease.
Most agreed that adoption of GVs could make a health center more competitive (94%, 17 of 18) and improve community outreach (100%, 18 of 18). Clinicians saw a potential for cost savings, particularly if group size was increased. They enjoyed participating in a research project that would provide benefit beyond their community.
The primary burden of GVs identified by clinicians was the time needed to implement them. Research-specific tasks such as data collection, chart abstraction, recruitment, and participation in webinars were noted to be particularly time-consuming. Clinicians felt recruitment was limited by the inclusion criteria, especially the high A1C and requirement to be an “active patient” in the clinic. They also found it challenging to achieve the goal group size due to a high no-show rate. Clinicians discussed the initial time investment needed to develop any new program and several felt that GVs would be less time-consuming once they were finished with the research project and the program was smoothly incorporated into the clinic workflow:
The only downside would be just the time involved but I think a lot of that, of course, is just the nature of the research project […] it's going to be easier to do once we’re out of the research realm.
Responses were mixed regarding productivity; some thought the team was breaking even while some believed that they were seeing fewer patients than in their traditional schedule. This was reflected in the survey data; 22% (4 of 18) disagreed that GVs could improve clinician productivity, 39% (7 of 18) neither agreed nor disagreed, and 39% (7 of 18) agreed with this statement.
One person expressed concern about maintaining patient privacy in a group setting; others said this was not a concern. Finally, some logistical challenges, such as staff turnover and last minute speaker cancelations, added to the time burden of GVs. Workflow was an issue, especially in the beginning of the program, as clinicians struggled to find time to pull each patient out of the group for the one-on-one visit. However, several clinicians noted that despite these initial challenges, their health center would be continuing GVs after the research project was over:
We will continue with diabetes [group visits] for sure because that is one of our missions, but we’ve […] already expanded to asthma and ADHD.
Discussion
We sought to understand various aspects of the group visit model of care from the patient and staff perspective. In our multisite study of community health centers in both rural and urban settings, we found that overall patient and staff satisfaction with GVs was high. Patients reported increased self-management skills and positive peer support, which will provide a sustainable basis for lifelong management of diabetes. Patients felt that GVs improved their health and were an efficient use of their time. Clinicians enjoyed the diabetes-focused nature of the visits and the opportunity for professional development, but responses were mixed about the program's impact on their productivity. Barriers included recruitment/attendance, data collection, and time management.
Previous studies of patient satisfaction with GVs have found generally positive results (17); patients have perceived improved coordination of care (19) and enjoyed having a longer visit with peer support (2). Our study confirms these findings in the CHC setting and adds to them. Patients noted the quality education they received and felt that their diabetes was better managed as a result. Importantly, the majority felt increased confidence in their own ability to manage barriers to diabetes control. By having patients take an active role in the group visit (e.g., setting their own goals), they become empowered and begin to see themselves as an important members of their healthcare team. About half of patients felt strong support from other group members and another third felt some support, echoing previous findings that self-management is facilitated by peer support (2,8). While group visits are longer than a typical appointment, patients felt they were an efficient use of time. The majority did not feel strongly about having their own PCP lead the visit, allaying concerns about the logistics of scheduling groups with patients from multiple clinicians.
Staff noted many benefits to GVs. They felt that GVs allowed them to know their patients more deeply, demonstrating that GVs do not detract from the doctor-patient relationship built during traditional appointments. A longer visit may allow more time for patients to share their stories and feel heard by their doctor. The depth of relationship may contribute to increased staff morale; GVs also gave them an opportunity to lead a new program. The professional diversity of GV leaders highlights the team-based, inter-professional approach needed to manage the complexity of diabetes. Furthermore, GVs could benefit the health center as a whole by improving image and outreach.
While clinicians felt that patient care was more efficient, this did not translate to improved clinician productivity. Based on interview data, we have several hypotheses to explain this finding. First, there is the time investment needed to start any new program. Planning where and when visits would be held, which materials would be used, coordinating guest speakers, etc. can be quite time-consuming. Clinics should consider the optimal workflow in their clinic space and create structured lesson plans to prepare for unexpected changes in attendance and speaker availability. Clinicians largely felt that having had done GVs once, the program would be easier to continue in the future. Second, staff struggled with tasks specific to involvement in a research project such as chart abstraction and recruitment. We anticipate that once the research project ends, GVs will be less time-consuming. Clinicians were also disappointed by a significant no-show rate, which resulted in a smaller-than-expected group size for several sites. Despite these challenges, we were encouraged to hear that several clinics wished to continue with group visits in the future.
Limitations
Our study is limited by the relatively small number of participants. Our study was conducted in multiple Midwestern CHCs, which while diverse, may not be generalizable to all practice settings. Further studies would also benefit from patient interviews.
Conclusion
In summary, patients and staff were highly satisfied with group visits. Patients noted the importance of peer support and felt better equipped to manage barriers to successful diabetes management. Clinicians perceived multiple benefits of GVs but were burdened by research-specific tasks and the challenge of creating a new program. GVs shows promise as an effective model of care with high satisfaction for both adult patients with diabetes and CHC staff.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735211056467 - Supplemental material for Patient and Clinician Satisfaction With Diabetes Group Visits in Community Health Centers
Supplemental material, sj-docx-1-jpx-10.1177_23743735211056467 for Patient and Clinician Satisfaction With Diabetes Group Visits in Community Health Centers by Samantha E Mannion, Erin M Staab, Jefferine Li, Amanda Benitez, Wen Wan, Amanda Campbell, Cynthia T Schaefer, Michael T Quinn and Arshiya A Baig in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735211056467 - Supplemental material for Patient and Clinician Satisfaction With Diabetes Group Visits in Community Health Centers
Supplemental material, sj-docx-2-jpx-10.1177_23743735211056467 for Patient and Clinician Satisfaction With Diabetes Group Visits in Community Health Centers by Samantha E Mannion, Erin M Staab, Jefferine Li, Amanda Benitez, Wen Wan, Amanda Campbell, Cynthia T Schaefer, Michael T Quinn and Arshiya A Baig in Journal of Patient Experience
Supplemental Material
sj-docx-3-jpx-10.1177_23743735211056467 - Supplemental material for Patient and Clinician Satisfaction With Diabetes Group Visits in Community Health Centers
Supplemental material, sj-docx-3-jpx-10.1177_23743735211056467 for Patient and Clinician Satisfaction With Diabetes Group Visits in Community Health Centers by Samantha E Mannion, Erin M Staab, Jefferine Li, Amanda Benitez, Wen Wan, Amanda Campbell, Cynthia T Schaefer, Michael T Quinn and Arshiya A Baig in Journal of Patient Experience
Footnotes
Acknowledgments
We would like to thank Sandra Ham for assistance with data analysis and Valerie Press, MD for critiques on a prior draft of the manuscript.
Authors’ Note
SM analyzed the data and wrote the manuscript. ES researched the data and reviewed/edited the manuscript. JL researched the data and reviewed/edited the manuscript. AB researched the data and reviewed/edited the manuscript. WW analyzed the data and reviewed/edited the manuscript. AC researched the data and reviewed/edited the manuscript. CS researched the data and reviewed/edited the manuscript. MQ researched the data and reviewed/edited the manuscript. AAB is the principal investigator and designed the study, researched and analyzed the data, and reviewed/edited the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Chicago Center for Diabetes Translation Research (NIDDK P30 DK092949). Dr. Baig was supported by an NIDDK Career Development Award (K23 DK087903-01A1). Study data were collected and managed using REDCap, hosted and supported by University of Chicago Center for Research Informatics (UL1RR024999).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.