
Abstract
The aim was to examine the association of patient-reported physician awareness of biological CAM use and patient perceptions of care experience and quality with a population-based study of patients with incident lung and colorectal cancer. This was a secondary data analysis using regression models. Outcomes of interest were patient reports of medical care experience and quality ratings. Among 716 patients who reported biological CAM use, 69% reported their physicians were aware of this. Patients who reported physician awareness of biological CAM use had higher adjusted scores for medical care experience ( + 5.4, 95%CI:2.3,8.6) and care quality ( + 3.6, 95%CI:−0.3, + 7.5). These associations suggest that physicians should be encouraged to inquire about biological CAM use.
Introduction
Patients with cancer frequently use complementary and alternative medicines (CAM), (1) which refers to “medical products and practices that are not part of standard medical care.” (2) The term CAM encompasses practices such as yoga and massage as well as biological products including vitamins, supplements, and botanicals including herbs (henceforth “biological CAM”). (2) Use of CAM by patients with cancer ranges from 11–95%, (3) and reasons for use include managing treatment side effects. (2) A study of patients who recently completed chemotherapy found that 51% reported the use of biological CAM during treatment. (4) Communication regarding biological CAM is especially important in the oncology setting, as these products may interact with anti-cancer therapies. (5) Interactions were considered likely to occur for approximately 37% of patients with cancer using CAM in a German study. (6) Decreased efficacy of anti-cancer therapies is also a concern; for example, St John's Wort may impact the efficacy of anti-cancer therapies. (2)
Although communication is important, 20–77% of patients using CAM may not discuss their use of it with health professionals. (3) When communication does occur it appears beneficial: oncology consultations involving such communication are longer and more patient-centered. (7,8) However, these studies focused on a few practices in specific geographic areas of the US, and the generalizability of these results is therefore unclear.
The question of this association is especially relevant as patient-reported experience measures (PREMs) are of increasing interest, particularly in the oncology setting. Recently, a cancer care-specific Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey was developed; CAHPS is a widely used measurement system for patient experience in the US. (9) CAHPS surveys are publicly reported and play an important role in quality improvement. (10) We sought to examine the association of patient reports of physician awareness of biological CAM and patient reports and ratings of care and experience and quality using cross-sectional data from a population-based study of patients with incident lung and colorectal cancer in the US. Among patients who reported using biological CAM, we evaluated if 1) patient reports of medical care experience and 2) ratings of care quality differed based on patient reports of physician awareness of biological CAM use.
Method
We used data from the Cancer Care Outcomes Research and Surveillance (CanCORS) study, a large, population-based study of patients with incident lung and colorectal cancer. (11) The data collection (11) and analytic (12) approaches for CanCORS have been described previously. Briefly, CanCORS collected data from approximately 10,000 patients with incident lung or colorectal cancer diagnosed between 2003 and 2005. Patients aged ≥21 years were identified using rapid case ascertainment and enrolled from geographic areas (including Alabama, Iowa, California, and North Carolina) and health systems (including the Veterans Health Administration) across the United States. (11) Over half of CanCORS patients were age 65 or older. (11) CanCORS patients were similar to patients in Surveillance, Epidemiology and End Results areas with new onset lung and colorectal cancer during the same period. (13) A computer-assisted telephone interview was used to survey patients in English, Spanish or Chinese. (11) The survey included questions about patient health, demographics and perceptions of care experience and quality. (14) The CanCORS study was approved by human subjects research committees (IRBs) at all participating institutions and informed consent was obtained from participating patients.
For this study, we used data from patients who were alive and completed the CanCORS full baseline survey (conducted a median of 5 months after diagnosis) and also answered “yes” to the question, “Since you were diagnosed with [lung or colorectal cancer], have you taken any herbal remedies or other supplements to treat your cancer or boost your immune system?”
Patients who reported using biological CAM were asked to name the products they used. For up to three products interviewers then asked: “Is your doctor aware that you are using this therapy?” A positive response to this question was categorized as “physician awareness.”
We focused on two outcomes: medical care experience and care quality. Medical care experience was measured using a five-item scale adapted from CAHPS. (11,14) The five items evaluated how often “your doctors”: (1) listened carefully, (2) explained things in an understandable way, (3) gave as much information as desired about cancer treatments, including potential benefits and side effects, (4) encouraged asking questions, and (5) treatment was with courtesy and respect. For each item, the available response options were “always/usually/sometimes/never;” patients could also answer “don’t know;” however, these responses were not included in the total score. Consistent with previous analyses, we transformed the care experience score to a 0−100 point scale (worst-best). (11) Although the primary outcome was the care experience score, we also evaluated each item in the score individually. Quality was assessed by a single question: “Overall, how would you rate the quality of your health care since your diagnosis;” response options included “excellent/very good/good/fair/poor.” This was transformed to a 0-100 (worst-best) score for consistency. As a sensitivity analysis, we also dichotomized all outcomes (100; always)/not top-box; this approach has been used with CAHPS because patient ratings tend to be highly positively skewed. (15)
Based on a review of the literature, we also sought to account for covariates that might affect patient report of their care and experience, as well as those associated with biological CAM use. These included disease stage, cancer type, survey language, race/ethnicity, age, educational attainment, gender, smoking history, health status, wealth and prior use of the biological CAMs discussed. We used two questions for health status that covered both general and mental health because these covariates are used when analyzing care experience data for surveys such as CAHPS; (16) both were drawn from the SF-12. (14)
We conducted univariable and multivariable linear regression analyses to evaluate the association of interest, adjusting for covariates. Each outcome was modeled separately. We also conducted analyses examining the association of interest at the item level for each item of the medical care experience scale. Logistic regression models were used for the sensitivity analysis. Multiple imputation (MI) was used for missing data; the imputation approach for CanCORS has been described previously. (12) Analyses were conducted in SAS (v9.4) and Stata (v16.0). Modeling assumptions were checked by examination of the residuals for linear regression and the Hosmer-Lemeshow test for logistic regression. Because of the use of MI, assumptions checking was implemented in each imputed dataset.
Results
Sociodemographic Characteristics
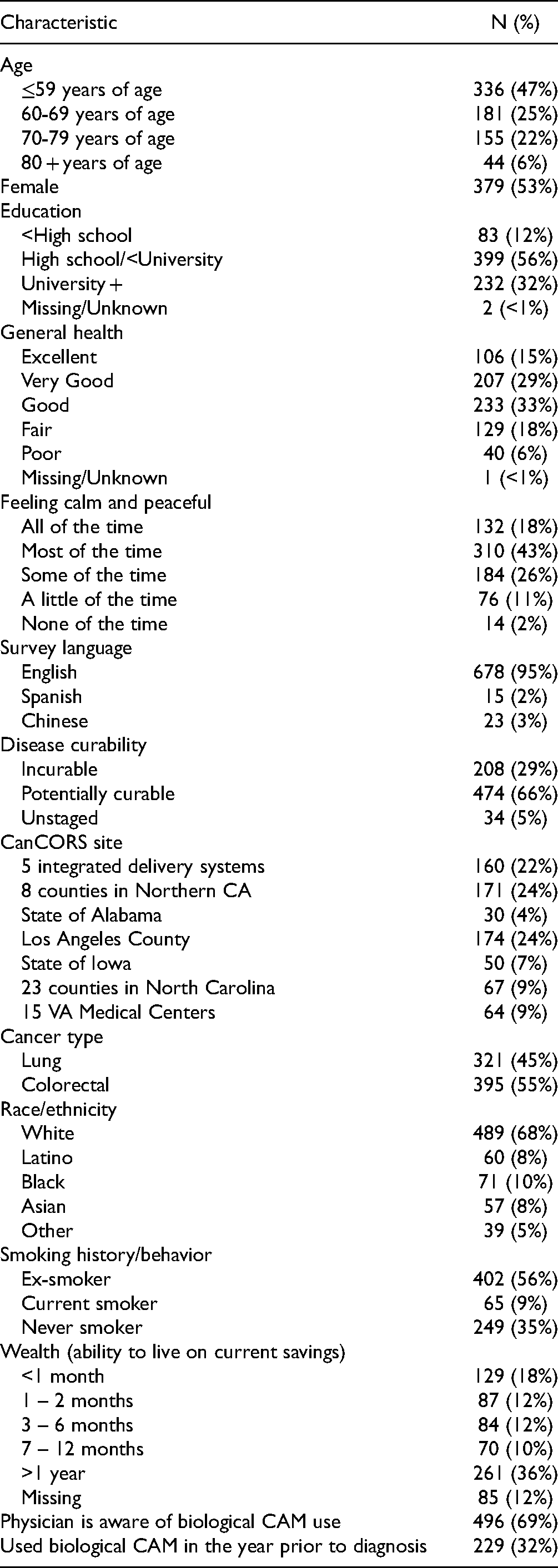
Of the 716 patients who reported using biological CAM (∼13% of the patients who completed the full baseline survey), nearly half (47%) were 59 years of age or younger. Most patients (69%, (n = 496)) reported that their physicians were aware of their biological CAM use (Table 1).
Characteristics of Patients who Report Biological CAM Use: Observed Data (N = 716).
Unadjusted Analyses
In unadjusted linear regression analyses, there was a positive association between patient reports of physician awareness of herbal product use and medical care experience (scores + 7.6 points on average, 95% CI: 4.4, 10.7) and care quality (scores + 6.4 points on average, 95% CI: 2.6, 10.3) (Table 2). This was also seen for top-box scores (Table 2). At the item level, all associations were positive.
Unadjusted and Adjusted + Association of Patient Reports of Physician Awareness of Biological CAM Use Among Users with Medical Care Experience and Quality Ratings.

Adjusted for: age, sex, education, general health status, mental health status, survey language, disease stage, CanCORS site, cancer type, race/ethnicity, smoking history, wealth, and prior use of biological CAM; ¶Could not model with logistic regression as too few respondents gave <top score.
Adjusted Analyses
In adjusted linear regression analyses, the differences were attenuated (Table 2). Patients who reported physician awareness of biological CAM use had adjusted medical care experience scores that were + 5.4 points higher on average (95% CI 2.3, 8.6). Adjusted scores for care quality were + 3.6 points higher on average and the confidence interval included zero (95% CI −0.3, + 7.5). For both outcomes, similar trends were observed for the top-box scores (Table 2).
At the item level, the associations remained positive but were smaller in most cases and the confidence intervals for two items contained zero. The association was strongest for the items relating to physician provision of information and encouragement of questions. For these two items, patients who reported physician awareness of biological CAM use had adjusted scores that were on average + 0.3 points higher (95% CI 0.1, 0.4) on a 4-point scale (Table 2). Similar trends were seen for the top-box scores (Table 2).
Discussion
Our findings of a positive association between patient reports of physician awareness of biological CAM use and patient-reported medical care experience and care quality are consistent with other studies. A recent study of patients with breast and prostate cancer receiving treatment in academic centers found that 64% of patients using biological CAM discussed this with their oncologists, (4) similar to the 69% of patients in this study who reported physician awareness. In that study, 34% of patients felt the discussion of biological CAM positively affected communication. (4) Our findings for the care experience items are consistent with this. In another oncology study, patient satisfaction scores were higher for visits that discussed CAM compared to those that did not. (7) Although experience and satisfaction are not equivalent, this does indicate that our findings are consistent with the literature.
This study had several strengths. As noted, it is one of the few population-based studies that evaluates the association between patient-reported physician awareness of biological CAM use and patient reports of care experience and ratings of care quality. This assessment is particularly important for newly diagnosed patients given the potential for biological CAM to interact with anti-cancer treatments. Thus, despite the age of the data the findings are relevant. Furthermore, the use of measures similar to those in CAHPS makes these findings highly relevant as PREMs continue to expand in oncology and a cancer-specific CAHPS has been developed. These positive associations suggest that physicians should be encouraged to inquire about biological CAM use.
Limitations
A limitation of this study is that the CanCORS data were collected several years ago and this cross-sectional study may therefore not reflect current use of and communication regarding biological CAM among patients with cancer. It also did not ask specifically about marijuana/cannabis products, which are increasingly available in recent years. Second, the question about biological CAM in the study did not separate ‘herbal remedies’ from ‘other supplements’; as not all supplements may be biological, it is possible that our sample is not limited to patients using biological CAM. Third, our cross-sectional analysis only permitted the assessment of an association rather than a causal relationship. Furthermore, we do not know if physician awareness was a result of doctors asking patients about biological CAM use, or if patients volunteered the information in the absence of physician inquiry. Our assessment of physician awareness is indirect, as it is reported by patients rather than physicians. Finally, the question about physician awareness referred to “your doctor,” the questions about medical care experience referred to “your doctors,” and the question about care quality referred to “the quality of your health care.” As many professionals are involved in cancer care, it is possible that patients may have interpreted these questions as referring to different physicians.
Footnotes
Ethical Approval
Approvals were obtained from the Dana-Farber Cancer Institute, the site of the CanCORS Statistical Coordinating Center (2002-P-000196) as well as each Primary Data Collection Research (PDCR) site.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with CanCORS IRB protocols.
Statement of Informed Consent
Participants at 2 PDCR sites provided written informed consent. The other site IRBs waived this requirement, and verbal informed consent was obtained.
Data Availability Statement
The data are not publicly available due to privacy and ethical considerations.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Xxxxxxx. Dr Roydhouse reports personal fees from Amgen outside the submitted work. Dr Gutman reports personal fees from Johnson & Johnson/Janssen, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Cancer Institute [grant numbers U01CA093324, U01CA093326, U01CA093332, U01CA093339, U01CA093344, U01CA093348], National Institute of General Medical Sciences [grant numbers U54GM115677]. Providence/Boston Center for AIDS Research [grant number P30AI042853]. Select Foundation: Fellowship, US Department of Veterans Affairs [grant number CRS02-164].