
Abstract
Informed consent has important ethical considerations for invasive procedures. Anecdotal evidence suggests an informed consent policy could heighten anxiety. We evaluated whether detailed information about breast biopsy prior to appointment negatively impacted patient experiences. Phase 1 surveyed patients receiving a standard appointment letter who underwent core biopsy (group A). Phase 2 surveyed two groups receiving standard letter plus biopsy leaflets: those who underwent core biopsy (group B) and those who did not (group C). The analysis included descriptive statistics and qualitative thematic analysis. Hundred percent of group A felt they were given enough information prior to biopsy and 72% felt it would not be helpful having information to read in the clinic beforehand. Hundred percent of group B and 94.1% of group C found it helpful to receive information with their letter. Common themes were good service, verbal explanation, and appreciation of written information. Despite concerns that too much information would heighten anxiety, this has not resulted in negative clinic experiences. Most patients found detailed information included with their appointment letter helpful, regardless of whether they had a biopsy or not.
Introduction
Informed consent is part of shared decision-making and has important ethical considerations when undertaking invasive procedures, such as core biopsy of the breast. The purpose of informed consent is to disclose information and ensure understanding (1). For consent to be valid, a patient must have the capacity to understand the information they have been given and must give their consent voluntarily (2).
The case of Montgomery versus Lanarkshire 2015 shifted the focus of the legal stance on consent to emphasize specific patient needs (3). The Supreme Court ruling confirmed that the law regarding consent should move away from a doctor-focused approach, to recognize that patients are autonomous and should be supported to make decisions about their own health. This notion echoes guidance from the General Medical Council (GMC) which has been in circulation since 2008. “Consent: patients and doctors making decisions together” (4) details the duties of a doctor in relation to informed consent; specifically mentioning the importance of working in partnership with patients, listening to their preferences, and giving information to patients in a way they can understand. This guidance has been further endorsed by other national organizations including the Royal College of Surgeons Edinburgh (5) and the Association of Breast Surgery (ABS) (6).
Anecdotal evidence suggests that a fully informed consent policy could potentially lead to increased confusion and heightened anxiety (7). Although it may seem excessive for relatively minor procedures, such as core biopsy of the breast, the principles of informed consent are just as important. Other breast centers in the UK have already adopted the addition of an information leaflet ahead of attending their “one-stop” breast assessment clinics.
While there is an increasing obligation to provide detailed information to patients, not all patients may wish such information. Our aim was to evaluate whether providing detailed information about breast core biopsy prior to symptomatic clinic appointment negatively impacted patient experiences.
Methods
All data were collected prospectively. As this was a service evaluation project, it was not necessary to obtain ethical approval. Caldicott guardian approval was not required as no patient identifiable data were collected.
Design and Sample Size
Between March and August 2018, a survey (phase 1) was conducted to evaluate the experience of consecutive patients who attended the symptomatic breast assessment clinic. The aim was to obtain 50 completed questionnaires (group A) which we felt would be a large enough sample to demonstrate a range of views while also allowing timely data collection. This also ensured that the study took place quickly enough that other changes in departmental policy would not confound the results. These patients received the standard letter clinic appointment letter only (Supplemental File 1) and underwent a breast core biopsy during their assessment.
Breast core biopsy was performed as indicated by clinical and radiological findings. Local anesthetic was infiltrated into the skin and breast tissue before a freehand or image-guided core biopsy was taken. Biopsies were taken using a 14G Bard Max-core® or 10G EnCor Probe® stereotactic biopsy gun. The number of cores taken was variable, designed to ensure a representative diagnostic sample was achieved, and operator dependent. Verbal consent was obtained for all patients and one practitioner obtained written consent for biopsies.
Phase 2 surveyed consecutive patients who received the detailed biopsy leaflet (Supplemental File 2) plus the standard appointment letter, divided into two sub-groups: those who underwent breast core biopsy as described above (group B) and those in whom biopsy was not clinically indicated (group C).
Procedure
During Phase 1, a total of 50 patients who underwent a breast core biopsy as part of their symptomatic breast assessment between March and June 2018 were asked to complete a questionnaire (Supplemental File 3) about whether they felt they had received enough information prior to attending. Patients were also asked how they would feel about a more detailed information leaflet. All questionnaires were given to patients to complete in the clinic waiting room after their core biopsy, to maximize the return rate. The number of patients who declined to participate was not recorded.
A detailed breast core biopsy information leaflet was designed, which was based upon information available from the ABS website but tailored to reflect our institutional working arrangements. During phase 2, patients who received the information leaflet were asked to complete a questionnaire (Supplemental File 4). The aim was to evaluate the impact of reading detailed information about breast biopsy before attending the symptomatic breast clinic, and whether this affected their clinic experience. The questionnaire was completed at the end of their clinic attendance to allow questions regarding the taking of a biopsy to be answered, where appropriate. Phase 2 data collection took place between June and August 2018, continuing until there was a minimum of 50 patients in each group.
Data Analysis
Once the target number of completed questionnaires was obtained, responses were transcribed electronically verbatim by a single researcher and collated under each question heading. Descriptive statistical analysis was conducted on questionnaire responses using Microsoft Excel© software, along with qualitative thematic analysis of free-text comments. Manual complete coding was undertaken by a single researcher to generate key concepts, which were then reviewed and revised into candidate themes by grouping similar codes together. A second researcher reviewed the raw data and candidate themes to improve validity.
Results
A total of 50 patients were included in group A, 51 patients in group B, and 51 patients in group C. All participants were females attending the symptomatic breast clinic, but no patient demographic details were collected for this study.
Questionnaire Results
All patients in group A (n = 50) felt they were given enough information about what a biopsy involves before they had their biopsy (Table 1). Seventy-two percent of group A (n = 36) felt they would not have found it helpful to have been given written information to read in the clinic before the biopsy was taken. Forty percent (n = 20) thought it would be helpful to have had an information leaflet included with their appointment letter. One patient did not answer question 3.
Group A Questionnaire Results.

A total of 102 patients were included in phase 2. Hundred percent of group B (n = 51) and 94.1% of group C (n = 48) found it helpful to have an information leaflet about breast biopsy included with their appointment letter. A 3.9% of group B (n = 2) and 5.9% group C (n = 3) admitted they did not actually read the information leaflet on breast biopsy before their appointment and one patient did not answer this question. All patients in group B (n = 51) felt they were given enough information about what a breast biopsy involves before it was taken (Table 2).
Group B & C Questionnaire Results.

Qualitative Thematic Analysis
The common themes identified from the analysis of the free-text comments are highlighted in Table 3, supporting patient satisfaction with the verbal information in group A.
Summary of Common Themes From Qualitative Analysis of Free-Text Comments.
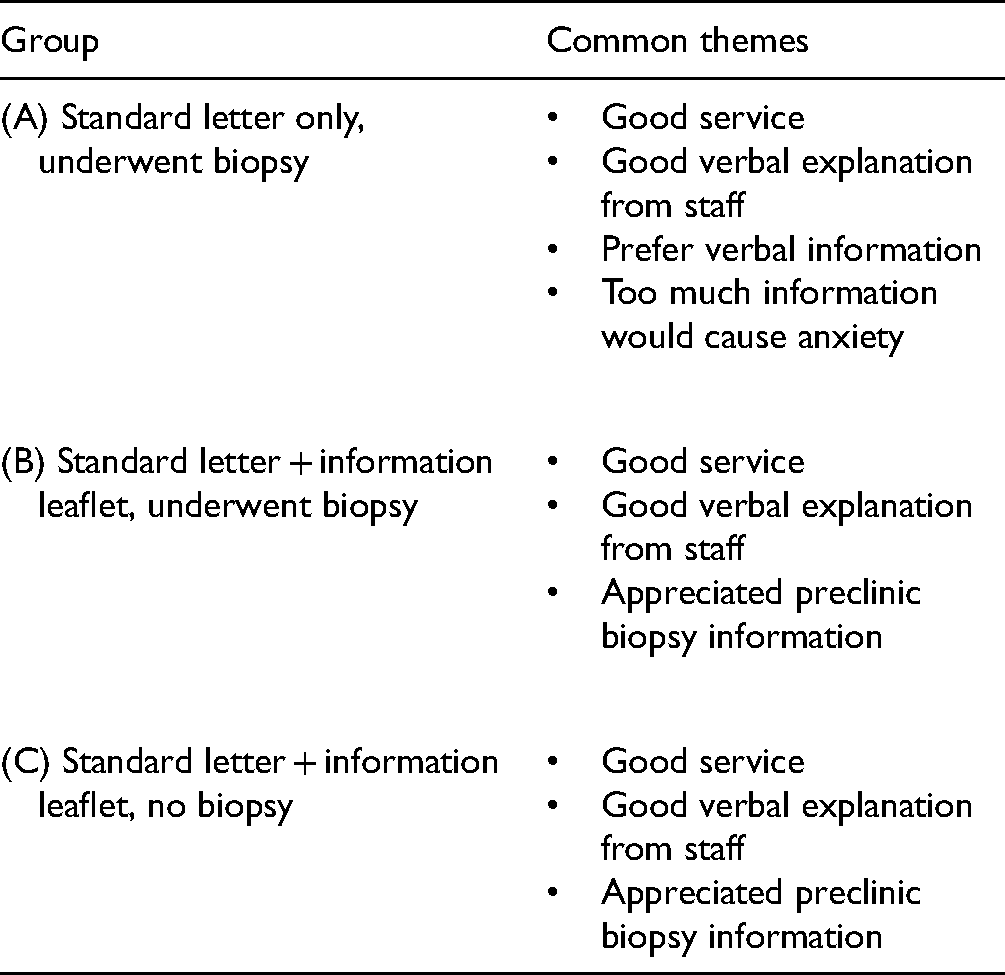
One common theme from group A was concern that too much information may cause anxiety, as noted by several patients: “Not everybody has to have a biopsy, so wouldn't [information leaflet] be unnecessarily scary for some?”, “I think too much info before appointment would have scared me”, and “too much information causes worry.” Other patients mentioned they would prefer information to be given verbally during their consultation, stating: “prefer to hear what's happening from the Doctor at the actual appointment.”
In group B and group C, the common themes from the analysis of free-text responses were the same: good service, good verbal explanation from the staff and they appreciated the written information provided beforehand.
Although there were no comments of the information leaflet creating feelings of anxiety in those whose biopsy was clinically indicated (group B), one patient from group C (no biopsy) stated: “the biopsy info worried me a little as I had not attended before and I wondered why I was getting told about biopsies so soon.”
Patients who had a biopsy (group B) commented: “I found all the information helpful” and “I had complete knowledge of what was going to happen and how the procedure was going to be.” Whereas patients who did not need to have a biopsy (group C) also appreciated the information, stating: “Although I did not have a biopsy, I felt fully prepared to have one as per the leaflet” and “I really appreciated the information provided. I am quite an anxious person and this helped me to be prepared with what may be involved.”
Discussion
The main aim of this study was to evaluate whether the introduction of a more detailed information leaflet prior to attending would negatively impact the patient experience in the symptomatic breast clinic. The majority of patients in phase 1 (72%) did not think it would be helpful to have been given written information to read in the clinic before their biopsy was taken, echoing the notion that more information may increase anxiety related to proposed procedures (7). However, 40% thought an information leaflet included with their appointment letter may be helpful.
In light of legal decisions, we felt that this preliminary study supported an inappropriate standard for consent in modern medicine. Therefore, despite phase 1 results, an information leaflet was developed and evaluated during phase 2 to introduce information on core biopsy earlier in the patient pathway. The aim of providing the information leaflet to patients ahead of their clinic appointment was to ensure patients had the opportunity to consider and reflect on relevant and important content before they attended the unit. We felt this would then allow discussion about biopsy with a more informed patient and aid the informed consent process.
Our unit covers a geographical area of ∼16,000 square miles. Some of our patients can travel in excess of 110 miles on the mainland, each way, to attend an outpatient clinic. For others, for example, traveling from the Western Isles can involve flights as well as vehicular transport. Our geography means that routinely providing a cooling-off period of hours or days after proposing a biopsy would completely disrupt our service and may well introduce unwanted delays. An effective one-stop clinic remains our preferred model and contributes to efficient patient care and timely diagnosis, but it would be unacceptable if patients were not comfortable with the process.
Nevertheless, the reality of giving more information did not appear to negatively impact our patient cohort during phase 2. Interestingly, the majority of the patients in the group who did not have a breast core biopsy felt it useful to have the information ahead of time. All patients who underwent a core biopsy during phase 2 felt they were given enough information ahead of time, although it is difficult to ascertain from the free-text comments whether this was due to the written information provided ahead of their appointment, the verbal explanation during their consultation, or a combination of both.
The literature describes participants’ understanding of informed consent, mostly in relation to participating in medical research (1,8). These studies have shown there is no consistent method proven to increase understanding for all patients, which demonstrates the individuality of the consent process and the importance of tailoring it to each patient. Other studies suggest that patients “feeling” informed is most important to them, rather than specific information (9,10). Studies describing parents’ experience of giving consent for their child to undergo surgery suggest that receiving comprehensive but understandable information is important to parents, but their reaction to such information was considerably different with some experiencing heightened anxiety and others feeling reassured (11,12).
What is clear from this survey is that our patients feel they are being provided with enough information to make an informed decision, regardless of whether that is given verbally or in writing. However, one patient who received the written biopsy information but did not have a core biopsy, commented that they found the information ahead of time concerning. Again, this reflects that consent is an individual process. While it is not our intention to overly worry our patients, this would not be a reason to discount the positive reception of the information leaflet by the rest of the patient cohort. Although we should respect requests for limited information, we need to ensure our patients understand the process and how we can support them in making decisions regarding their care.
There are no guidelines from ABS/SIGN/NICE that mandate written consent for needle core biopsy, and the GMC state: In the case of minor or routine investigations or treatments, if you are satisfied that the patient understands what you propose to do and why, it is usually enough to have oral or implied consent.
Needle core biopsy may seem like a routine investigation, but the potential risk of pneumothorax and bleeding suggests that perhaps it should have written consent. Indeed, a signed consent form, while not ensuring informed consent, is standard care in many units in the UK and worldwide.
Across all 3 groups in our study, the overwhelming majority of free-text comments were related to the good service provided and generally positive experience of the Breast Unit. Our staff should be commended on providing a consistently positive experience to all of our patients, regardless of their diagnostic journey, and our patients are extremely grateful for this.
There are limitations associated with our study. Firstly, the sample size is small, and therefore it is difficult to draw generalized conclusions applicable to a wider population. The patients captured may not accurately represent the referrals for the whole year as the location of the mobile screening van affects the proportion and age range of symptomatic referrals from that area. However, we feel this is a representative sample of the patients who attend our unit and we are comfortable with accepting those conclusions at a local level.
Secondly, there are limitations with our chosen method of data collection. We demonstrated that almost all of the patients surveyed at our unit were in favor of the detailed information; however, we were unable to evaluate whether patients chose not to attend their appointment based on the information sent. Our focus was primarily based on the quality of the information provided, therefore we did not enquire about anxiety levels prior to attending and whether this was influenced by the information in the letter. The comments section was intended to enable patients to provide feedback on the process, but there were no specific questions related to anxiety levels. While a questionnaire is easy to administer and cost-effective, there can be limits in the amount of information gathered, and subtlety and context can often be missed by the generalized wording of questions (13). However, to obtain a more in-depth understanding of patient's feelings and understand differences, we would have needed to conduct focus group interviews, which were not feasible during the study time frame.
The timing of the survey delivered to patients in phase one may have influenced their responses. The survey was given to patients in the waiting room of the “one-stop” clinic to complete immediately after undergoing a core biopsy. Responses may be overshadowed by the heightened anxiety associated with the biopsy and awaiting a diagnosis, and answers may have been different if they had been surveyed at a different point in their diagnostic journey. There may have also been privacy/confidentiality issues generated by asking patients to complete the questionnaire in the waiting room. Patients may have been reluctant to provide negative feedback and be concerned they may be identifiable.
Individual consent practice varied between practitioners and could introduce bias, but unless there is a standard proforma which is followed as a script with no option for addressing patients’ questions, it is almost impossible to standardize verbal information giving.
Finally, it is worth noting that written information works well for people with English as their first language, but to ensure all patients are given the same information, consideration regarding literacy status and natively spoken language would need to be made. While this is not necessarily a large undertaking for our unit, other units may have a significant barrier to overcome to provide such information in numerous different languages.
Conclusion
Despite initial concerns that too much information would heighten anxiety; this has not resulted in negative clinic experiences. Almost all patients found it helpful to have detailed information included with their appointment letter, regardless of whether they actually went on to have a biopsy or not.
Providing detailed information prior to a clinic visit has increased patient awareness prior to their attendance, even though patients were already satisfied with the amount of information and the explanations given to them verbally by clinicians during their clinic visit. Satisfaction with our service may simply reflect a lack of familiarity with breast clinics in other units.
All future patients will routinely be provided with a breast core biopsy information leaflet included with their standard clinic appointment letter. We feel justified in making this change, although it was not necessarily indicated after our pilot survey, and would encourage other units to strongly consider this if they feel it enhances the standard of care provided.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735211049658 - Supplemental material for Breast Core Biopsy Information and Consent: Do we Prepare or do we Scare?
Supplemental material, sj-docx-1-jpx-10.1177_23743735211049658 for Breast Core Biopsy Information and Consent: Do we Prepare or do we Scare? by Jennifer Pollard, Heather Rose, Russell Mullen and Nick Abbott in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735211049658 - Supplemental material for Breast Core Biopsy Information and Consent: Do we Prepare or do we Scare?
Supplemental material, sj-docx-2-jpx-10.1177_23743735211049658 for Breast Core Biopsy Information and Consent: Do we Prepare or do we Scare? by Jennifer Pollard, Heather Rose, Russell Mullen and Nick Abbott in Journal of Patient Experience
Supplemental Material
sj-docx-3-jpx-10.1177_23743735211049658 - Supplemental material for Breast Core Biopsy Information and Consent: Do we Prepare or do we Scare?
Supplemental material, sj-docx-3-jpx-10.1177_23743735211049658 for Breast Core Biopsy Information and Consent: Do we Prepare or do we Scare? by Jennifer Pollard, Heather Rose, Russell Mullen and Nick Abbott in Journal of Patient Experience
Footnotes
Authors’ Note
Ethical approval is not applicable to this article. This article does not contain any studies with human or animal subjects. Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.