
Abstract
A paper-based questionnaire was used to measure out-of-pocket expenses, income loss, and informal (unpaid) care from the cancer patient’s perspective. A total of 181 adult solid cancer patients on chemotherapy for at least 3 months were recruited from 1 teaching hospital in Riyadh, Saudi Arabia. The majority were female (66%) and 41% were 60 years of age or older. A total of 107 respondents used their own car for transport to and from the hospital to receive chemotherapy (median distance 42 km). Over the last 4 weeks, 21% purchased medications, 18% visited a physician, and 8% visited a physiotherapist, spending a median amount of $47, $220, and $793, respectively. A total of 47 participants were employed at the time of their cancer diagnoses, and 32% of them reported some loss of income. A total of 85% of respondents were escorted by a carer during chemotherapy sessions. Approximately 64%, 31%, 61%, 43%, and 28% reported getting help from a carer for housework, child care, shopping, medicine taking, and personal care, respectively. The carer spent on average 50 h per week looking after the patient.
Introduction
The current evidence indicates that costs borne by patients and their families, that is, out-of-pocket costs, as a result of a cancer diagnosis, are significant. A systematic review of studies describing the financial burden experienced by cancer patients and/or informal caregivers in countries with predominant publicly funded healthcare systems identified 32 studies published up to 2019. The review found a range of financial impacts including patient/caregiver out-of-pocket costs (range US$17-US$506/month), lost income (range 17.6-67.3%), travel and accommodation costs (range US$8-US$393/month) (1). According to the World Health Organization, total out-of-pocket spending, an important indicator of progress toward universal health coverage, is high in low- and middle-income countries compared to high-income countries (2). Understanding the magnitude of financial hardship that accompanies cancer diagnosis is important for developing a patient-centered plan that meets the needs of cancer patients and their families (3).
Economic evaluation research from the patient perspective could contribute to achieving cancer care that is patient-centered and evidence based (4). Conducting an economic evaluation from a patient's perspective entails the estimation of direct and indirect costs. For instance, direct medical costs are associated with resources used to deliver healthcare services to prevent, detect, and treat cancer, while direct nonmedical costs are associated with resources supporting the medical services delivered, such as travel costs to attend a chemotherapy treatment in the hospital. Indirect costs refer to costs that result from productivity loss such as work income lost due to cancer. A systematic review published in 2016 examined health economic evaluations conducted from the patient's perspective and identified 30 studies in different patient populations: 29 studies included direct medical costs, 17 studies included direct nonmedical costs, and 15 studies included indirect costs (5).
Cost assessment in economic evaluations involves the identification of relevant costs based on the study perspective, the measurement of costs by determining the quantity of resources utilized, and the valuation of costs by assigning a unit cost or price to resource items. Data on resource utilization may be obtained from different sources: medical records, administrative data, disease registries, self-reported, and expert opinion. Each method has its advantages and disadvantages (6–8). Self-reported methods for measuring resource use data include questionnaires, interviews, and diaries. Patient-completed questionnaires are a feasible and reliable method of measuring estimates of resource utilization and out-of-pocket costs when compared with accessing administrative databases or diaries (6,7,9–11). These instruments are valuable, especially for economic evaluations conducted from the patient and societal perspective (8). A review on self-reported questionnaires capturing resource utilization identified 15 papers (11). The majority of the included studies measured resources such as visits to general practitioners and inpatient stays, and few examined nonmedical resources and productivity. Therefore, patient self-reported instruments to capture resource use utilization in general and those that capture nonmedical costs and productivity loss in particular appear to be scarce. The availability of such instruments would help to understand the full impact of cancer and facilitate conducting economic evaluations from the perspective of the patient and society as a whole.
The primary aim of this paper was to measure the resources use from the cancer patient perspective, including out-of-pocket expenses, income loss, and informal (unpaid). Medical costs covered by the healthcare provider are outside the study scope.
The study setting is in Saudi Arabia, where healthcare is provided by a combination of the public sector through governmentally funded facilities and the private sector. The governmentally funded facilities provide comprehensive care, including diagnosis and treatment, at no cost to the Saudi citizens. Schemes exist to support patients; for instance, if patients are referred for diagnosis or treatment outside their city, they are entitled to claim travel costs for themselves and an escort if needed. The private sector is required to provide health insurance policies to cover their Saudi and non-Saudi employees and their dependents. For those who work in the private sector, insurance companies are obliged to cover cancer treatment up to the US $133333, including costs of diagnosis, treatment, and reconstructive surgery.
Methods
This was a questionnaire-based study. The study was conducted in one teaching hospital in Riyadh, Saudi Arabia, during the period between May 2018 and April 2019. This means we included only patients receiving diagnosis and treatment services from a publicly funded institution and we did not recruit patients treated in the private sector.
Questionnaire Development
Building on a review of previous relevant literature (12–18) and interviews with cancer patients (n = 8), 2 of the authors with specialized training in clinical oncology (LA) and health economics (SA) developed the questionnaire. Another group of cancer patients (n = 8) and health professionals (n = 3) revised the questionnaire length, clarity, understandability, comprehensiveness, and acceptability. The suggested modifications resulted in a further revised version with wording changed, explanations added or splitting a question into 2 questions.
The questionnaire collected information on the following resources use categories: attending chemotherapy treatment, medical products, and service utilization such as purchasing nonprescription drugs, nonmedical costs, such as housing adjustments, days off work, and help received as a result of the patients’ limited ability to do household chores or childcare. Patients were instructed to recall the volume such as the number of visits or hours of care and the amount paid, if applicable. The recall period was the previous 4 weeks. The questions were mainly closed-end (yes/no or choose from a list) with filter questions to clarify whether any of the subsequent cancer-related resources used were consumed and only if the participants answered “yes” were they required to specify the frequency and/or cost of utilization. The questionnaire was written in the Arabic language (the English version is provided in the Additional file 1).
Participants
We included patients with solid cancer in stages I to III who were on active chemotherapy treatment for at least 3 months. We excluded patients on radiotherapy, stage IV patients receiving palliative treatment, and those unable to comprehend and answer the questionnaire.
Patients waiting for or receiving chemotherapy infusions in the hospital were recruited to participate in the study. Two of the authors and 4 PharmD students identified eligible patients, provided them with information sheets about the study, answered their questions, and obtained their consent to participate in the study. The paper-based questionnaire was filled by the patients and/or their care giver.
Statistical Analysis
The feasibility and acceptance of the cost questionnaire were assessed by the response rate and completeness of data. Completeness of data is reported as the number of missing items. For filter questions, missing items were either missing information on the filter question itself or if the filter question was checked “Yes” and further information is missing.
Out-of-pocket costs were used directly as listed by the participants. Costs were converted to US dollars ($) using the exchange rate of $1 = 3.75 Saudi Riyals.
Descriptive statistics (percentages, means, and standard deviations) were used to summarize demographic, resource utilization, and cost data.
The study was approved by the King Saud University Health Sciences Colleges Research on Human Subjects Institutional Review Board (number E-18-3215). Informed written consent was obtained from each participant.
Results
A total of 215 patients were invited, and 183 patients completed the questionnaire (85% response rate). Two questionnaires were excluded because of incomplete answers, and the final number of questionnaires analyzed was 181. Patients completed the questionnaire in ∼20 min. There was zero nonresponse or missing items for 19 questions, 1 for 19 questions, 2 for 5 questions, and more than 2 in 13 questions.
Seventy-four of the respondents (41%) were 60 years of age or older and 118 (66%) were female (Table 1). Thirty-nine patients (22%) were illiterate, and the carer had to read and complete the questionnaire for them. Sixty-one (34%) patients were colon cancer patients, 41 had (23%) breast cancer, 13 (7%) had lung cancer, and 65 (36%) had other types of cancer. Fifty-four (31%) patients had metastatic cancer. The average number of months since diagnosis was 19.7 (SD 21.9).
Participant Characteristics.

Chemotherapy Sessions Resources Use and Out-of-Pocket Costs
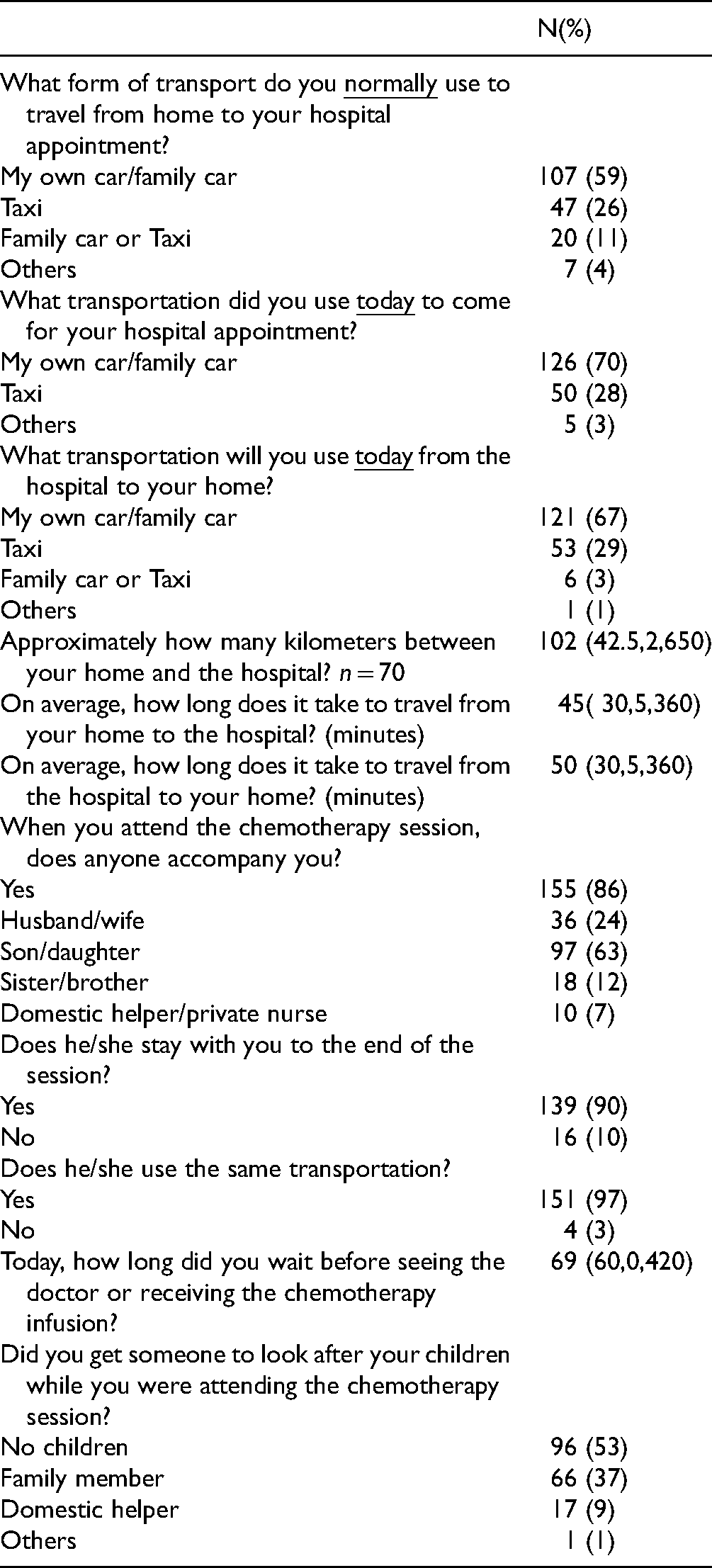
The majority of respondents used their own car for transport to and from the hospital to receive chemotherapy (median distance 42 km). Patients and their carers spent considerable time in transportation to and from the hospital, and the time spent waiting to see the doctor or start the chemotherapy session is noteworthy (Table 2). The majority of respondents (86%) were accompanied by a carer during the chemotherapy session who stayed with them until the end of the session.
Chemotherapy Sessions Related Resources use. Values are Numbers (Percentages) or Mean (Median, Min, Max).
Seventy-four (41%) respondents were from outside Riyadh and half of them (n = 40, 53%) rented accommodations during their chemotherapy sessions. Thirty-nine patients rented for an average of 4 days (median 3, min 1, max 10) at a median cost of $67 per day (Table 3). Three patients were excluded from the analysis because they reported outlier renting days (360, 360, and 180 days). Of the 74 patients, 36 (49%) and 7 (9%) reported they received governmental support for airline tickets and aid for renting, respectively.
Summary Statistics of Costs Components as Reported by Participants (US$).

Assuming at 10 km/L of petrol at $0.41/L.
Medical Resources Use and Out-of-Pocket Costs
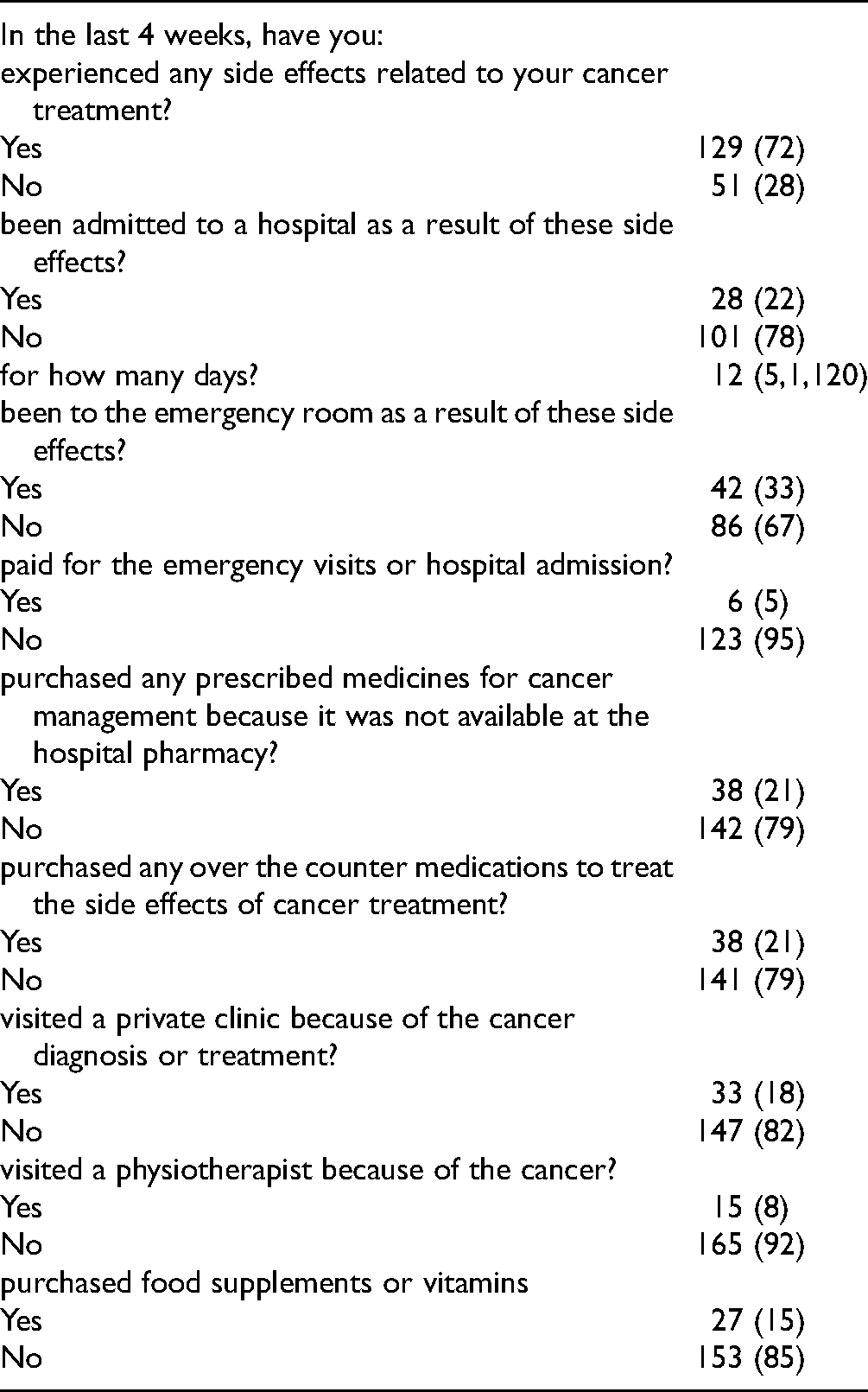
Twenty-eight participants reported being admitted to the hospital as a result of cancer treatment side effects (Table 4). Over the last 4 weeks, 38 (21%) purchased medications, 33 (18%) visited a private clinic physician, and 15 (8%) visited a physiotherapist, spending a median cost of $47, $220, and $793, respectively (Tables 3 and 4).
Medical Related Resources Use and Out-of-Pocket Costs. Values are Numbers (Percentages) or Mean (Median, Min, Max).
Nonmedical Resources Used and Out-of-Pocket Costs
A small number of respondents reported the need to buy a house (n = 17, 9%) or make a house adjustment (n = 31, 17%) as a result of their cancer diagnosis. The median cost of housing adjustments was $2093. Thirty-six respondents (20%) reported the need to buy equipment to facilitate movement at a median cost of $133. Sixty-nine percent of the respondents reported buying more fruit and organic food since their diagnosis with a median cost of $40 weekly (Table 3). Respondents reported that they had employed a nurse (6, 3%), a full time (57, 31%), or part time (36, 20%) domestic helper as a result of their cancer diagnoses.
When asked to indicate any other out-of-pocket costs not examined in the questionnaire, a few respondents repeated the items from the questionnaire, mainly travel costs, while others reported the following: dressings (n = 3), special clothing due to weight changes, or a new body shape after a mastectomy or discomfort from wigs, hats, and scarves (n = 2), obtaining a second medical opinion (n = 1), organic shampoo and soap (n = 1), immune-boosting supplements (n = 1), and personal items (n = 3).
The Impact of Cancer on Productivity at Work
A total of 74% of the respondents were not working when diagnosed with cancer (n = 133). We asked the respondents who reported that they were working (n = 47) if the diagnosis impacted their work. The majority (31, 91%) stated that cancer resulted in paid time off work. A small number of patients reported working fewer hours (13, 28%) or income changes (15, 32%) as of result of the cancer diagnosis. On average, respondents reported 38 h were lost from work due to cancer in the preceding 4 weeks (median 29 h).
The Impact of Cancer on the Need for Help With Activities of Daily Life
We asked the participants about the provider of support in activities of daily life, whether she or he was a family member or a domestic helper, family members were frequently reported to be the helper with house chores (64%), childcare (31%), shopping (61%), medicine taking (43%), and personal care (28%). Family members were a son or daughter in the majority of our respondent's answers (87, 48%). Fifty-eight (32%) respondents reported that the family member had to take a leave from work to provide care. According to our respondents, the family member spent on average 50 h a week providing care for the cancer patient (median 24 h).
Discussion
The aim of this study was to measure out-of-pocket expenses, income loss, and informal (unpaid) care. The insight obtained from this study may prove invaluable for planning economic evaluations from the societal or patient perspective.
Our findings agree with findings elsewhere (1,13,14–17,19–22,23) that the economic burden for out-of-pocket costs of cancer patients is significant, although the magnitude differs according to differences in healthcare, social welfare, and legal systems. Similar to previous research (1,13,14–17,19–22,23), we identified a range of out-of-pocket costs due to a cancer diagnosis or treatment including travel, accommodation if patients lived some distance from their treatment centers, house modifications, food supplements, and the purchase of medical equipment. Other costs reported elsewhere and not reported in our sample include counseling, higher energy bills for heating and cooling a house, extra wear and tear on a car from frequent appointments, telephone calls, complementary therapies for wellness such as meditation and yoga, and exercise classes (12,24). In agreement with previous research (25), attending treatment and the management of adverse events have considerable effects on patient and carers time and activities.
The economic burden of wage loss attributable to cancer is significant (19,26). Although only 26% of our sample were employed at the time of their cancer diagnosis, our findings offer useful insight into the impact of cancer on work productivity. For instance, although 74% of those working reported taking days off work, only 32% reported an income change. Possible reasons for this could be having paid sick leave benefits to cover the period of the disease, mitigating the negative impact on income. Other researchers reported that the impact of loss of income can be minimized with adequate sick pay (12,19,24). Future research including a larger sample size with a younger and more diverse population, such as those who are self-employed, is required to identify real challenges around income reductions.
An interesting finding is that half of the eligible patients failed to reclaim their entitlement to support for travel expenses. Possible explanations for this include a lack of information on their entitlement or lengthy bureaucratic procedures. Céilleachair et al (19) described the confusion of patients when their application for support had been denied because they received wrong information about their entitlement. Future research in this area is recommended.
The magnitude of family support identified in our study reflects the strong family bonds in Saudi Arabia. Similar observations were reported in other settings with strong family cohesion, such as Ireland (19). The accessibility to family support can also impact the economic stress of cancer patients. Furthermore, failure to acknowledge these costs in future research will grossly underestimate the potential economic burden faced by patients and their relatives.
Implications for Practice and Future Research
The Saudi Ministry of Health and other healthcare providers should acknowledge the impact of financial hardship that accompanies a cancer diagnosis and support must be provided to ensure that travel, child care, and other out-of-pocket expenses do not constitute barriers to access healthcare services. We recommend that at the time of diagnosis, appropriate financial advice is given to empower patients with information about their rights in the workplace and any entitlement or schemes benefiting patients.
Other studies shown out-of-pocket expenses were influenced by variables such as age and tumor type (14). The economic burden accrued based on the patient's clinical course, that is, early versus late stage of diagnosis, sociodemographic characteristics, and insurance status, were not explored by the current research due to the small sample size and warrant further investigation.
Thorn et al (27) used a Delphi survey technique to identify resource use items that should be included in a standardized adult instrument from a UK provider perspective. The use of a similar approach to specify resource use items from the cancer patients’ perspective is recommended.
The emotional impact on cancer patients caused by cancer financial burden (23) warrants further investigation in future research. The out-of-pocket expenditures reported by our sample are different from how much cancer patients need to spend but were unable to do so. This is an important issue for future research.
Strengths and Limitations
A strong point in our approach lies in the use of self-reported instruments that examined patient out-of-pocket costs, including medical and nonmedical, productivity, and informal care issues concurrently to provide a complete picture.
A strength of this instrument is that it builds upon previously developed questionnaires and involved patients at the early stages of the questionnaire development to account for the local context.
The response rates were high (85%), and the item-level missing data were minimal, which is comparable to similar research (9).
We assessed resource use, not just costs, to increase the clarity and transparency of the analysis and to allow readers to understand how the costs of attributable resources may be similar or different in their own setting.
This is the first study on the costs from the patients’ perspective in our region, and the lack of such research is not surprising given that economic evaluation studies in general are limited in the region (28,29).
This study has some limitations. First, we were unable to corroborate the reported values of healthcare utilization with medical and administrative records. Future validation of the questionnaire criterion validity could be achieved by comparing the questionnaire information on medical health resources utilization and days off work with medical and administrative records. However, patients’ clinical records in Saudi Arabia are currently fragmented across the health system, and therefore accurate estimates may not be possible because of a lack of readily available information. Additionally, future validation of its convergent validity could be achieved by comparing the questionnaire findings with a prospective cost diary. Second, the results of this study were not derived from a nationally representative sample of cancer patients. Third, the sample size is small, although comparable with similar research (9,10,30,31). Further validation in larger and more representative samples is encouraged. Also, patients on radiotherapy and stage IV patients receiving palliative care were not included in our study in an attempt to achieve a homogenous sample, therefore, their financial difficulties should be explored in future research.
Fourth, in accordance with Bhandari and Wagner (32)'s recommendation, we used a shorter period of 4 weeks for frequent utilization, as more is forgotten over longer periods of recall. However, recall bias may have produced errors in the reports of resource use. Finally, the findings of the current study are not generalizable to other countries with different health and social care system.
Conclusion
The potentially significant impact that nonmedical direct and indirect costs can have on the total cost warrants including these data in estimates of the costs of cancer care.
Footnotes
Acknowledgments
The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding this work through the Undergraduate Research Support Program, Project no. (URSP-3-18-144). The authors thank Almarzouqi H, Almalki H, Almutairif A, Alonazi G for their help in patient recruitment.
Authors' Contributions
SA: Conceptualization, Methodology, Writing—Original Draft LA, JA, and LA: Methodology, Writing—Review & Editing. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deanship of Scientific Research at King Saud University for funding this work through the Undergraduate Research Support Program, Project no. (URSP-3-18-144). The funder played no role in the design, analysis, or conduct of the study.
Disclosure
The authors declare that they have no competing interests. The abstract of this paper was presented at the ISPOR Europe Conference 2019 as a poster presentation with interim findings (abstract number PCN167). The poster's abstract was published as “Conference Abstracts” supplement in Value in Health Journal, 2019; 22 Supp 3: S403-S940: (![]() ).
).
Ethics Statement
The study was approved by the King Saud University Health Sciences Colleges Research on Human Subjects Institutional Review Board (number E-18-3215). Informed written consent was obtained from each participant.
Informed Consent
Informed written consent was obtained from each participant.