
Abstract
Health organizations want to measure patient-reported outcome measures (PROMs) longitudinally. Two medical assistants called people selectively at 6 weeks and routinely at 6 months to obtain PROMs as part of routine musculoskeletal specialty care. Only 47% of patients (123 of 263) were reached by phone at 6 weeks and 41% (246 of 594) at 6 months. Spanish speakers were more likely to answer. Eighty-nine percent of people reached at 6 weeks and 76% reached at 6 months were willing to complete PROMs. Speaking Spanish, older age, and fewer symptoms of depression were associated with completing PROMs when reached by phone at 6 weeks. Women and Spanish-speaking patients were more likely to participate at 6 months. The observation that most people do not participate in longitudinal PROM measurement in a system that devotes notable resources in the setting of musculoskeletal specialty care—with some variation by psychosocial factors—suggests that longitudinal PROM measurement may be infeasible. Future work can explore alternative measures of the value of care that account for the large percentage of people that deprioritize care after a single specialty visit.
Introduction
Patient-reported outcome measures (PROMs) are questionnaires that quantify symptom intensity and activity intolerance. Quantification of the subjective aspects of illness using PROMs can be used in research to monitor treatment effectiveness and help determine the value of health resources. They can also be used with patients as part of shared-decision making (1–3). PROMs are increasingly used in musculoskeletal specialty care, perhaps in part because a large proportion of orthopedic surgery is discretionary and addresses quality of life (4). Health systems want to track PROMs to demonstrate the value of their work (5). Alternative payment models attempt to measure the quality or value of care, which is supported by longitudinal completion of PROMs (2).
Prior research suggests that the majority of patients see a musculoskeletal specialist a single time and that few are still in care 6 months after their initial visit (6,7). This poses a challenge for clinicians and health systems that want to track PROMs over some minimum time after a specialty care episode to help establish the value of care. It is well known that research questionnaires sent via mail, email, or text have poor response rates (8). To inform attempts to improve participation we sought patient characteristics associated with completing PROMs remote from initial care.
Using a practice-wide database of upper-extremity patients, in a setting where an alternative payment model included longitudinal measurement of PROMs and two full-time bilingual medical assistants were hired for this purpose, we asked: (1) among patients who are scheduled for a 6-week or 6-month follow-up phone call, what factors are associated with the ability to successfully contact patients? (2) For patients who are successfully reached, what factors are associated with willingness to complete repeat PROMs? (3) What factors are associated with completing repeat PROMs for all patients?
Methods
Study Design and Setting
In this institutional review board-approved study, we performed a retrospective database study of all adult (≥18 years) patients with upper-extremity conditions who were scheduled for a 6-week and/or 6-month follow-up phone call after their initial office visit between October 17, 2017, and January 29, 2019. A notable percentage of the patients in this unit are part of an alternative payment model with a reporting metric based on longitudinal measurement of PROMs designed to help measure the value and quality of care. During the time of this study, the organization hired two full-time, bilingual medical assistants to contact all patients routinely 6 months after an initial specialty care visit, with selective use of a 6-week call as an alternative to a return office visit or for patients the team wants to monitor more closely. Patients who were not called by the medical assistants at any time point and patients who spoke languages other than English or Spanish were excluded from the study.
Two hundred sixty-three patients were called 6 weeks after their initial visit; the mean age was 52 ± 14 years, 63% were women, and 65% were English speaking and 35% Spanish speaking (Table 1). At 6 weeks, 47% of patients (123 of 263) were successfully reached by phone. A total of 595 patients had a new patient visit during the study period and we attempted to reach all of them by phone 6 months after the visit to complete PROMs. The mean age of this cohort was 51 ± 14 years, 62% were women and 69% were English speaking and 31% were Spanish speaking. At 6 months, 41% of patients (246 of 594) were successfully reached by phone.
Patient Demographics.

Continuous variables as mean ± standard deviation or median (interquartile range); discrete variables as number (percentage).
Abbreviations: GAD-7, Generalized Anxiety Disorder-7; PHQ-2/9, Patient Health Questionnaire-2/9; PSEQ-2, Pain Self-Efficacy Questionnaire-2; qDASH, quick disabilities of the arm, shoulder, and hand.
Measurements
Patients were asked to complete surveys at baseline, at 6 weeks, and 6 months after their initial visit. Arm-specific physical limitations were measured with the Quick Disabilities of the Arm, Shoulder, and Hand (qDASH), an abbreviated version of the DASH consisting of 11 items, with scores ranging from 0 (no disability) to 100 (most severe disability) (9). Coping strategies in response to nociception were measured using the two question version of the Pain Self-Efficacy Questionnaire (PSEQ) (10). Higher scores indicate better accommodation of pain. We measured symptoms of depression using the Patient Health Questionnaire-2 (PHQ-2), which inquires about the frequency of depressed mood and anhedonia in the past 2 weeks. Each item is scored in a 4-point Likert-scale, ranging from 0 (not at all) to 3 (nearly every day), with higher scores indicating more symptoms of depression (11). Patients with scores >3 on the PHQ-2 were asked to complete the 9-item version. The Generalized Anxiety Disorder-7 (GAD-7) was used to measure symptoms of anxiety in the last 2 weeks on a continuum, with a higher score indicating greater symptoms of anxiety (12). Additionally, patients completed a questionnaire of basic demographics (e.g., age, gender, and ZIP code). A research assistant marked whether they were able to contact the patient by phone, and, if reached, whether patients agreed to complete the survey (qDASH).
Statistical Analysis
Continuous variables were presented as mean ± standard deviation or median (interquartile range). Discrete variables were presented as frequencies with percentages. To detect variables associated with reaching patients at each time point and their willingness to complete the survey, we conducted bivariate analyses, accounting for age, gender, language (English compared to Spanish), city (Austin compared to other), GAD-7 at baseline, PHQ-2/9 at baseline, PSEQ at baseline, and qDASH at 6 weeks or 6 months. We used the Student t-test or Mann–Whitney U test for continuous variables, where appropriate. For categorical variables, Fisher’s exact were used. City had to be dichotomized into “Austin” and “other” due to low numbers. All variables with P < .10 were moved to multivariable logistic regression. We reported Odds ratios, standard errors, and P values. All P values <.05 were considered statistically significant.
Results
In bivariate analysis, greater odds of reaching patients at 6 weeks was associated with women and the Spanish language (Appendix in the Supplemental Material). In multivariable logistic regression, greater odds of contacting patients at 6 weeks after an in-person visit was independently associated with the Spanish language alone (Table 2). Greater odds of reaching patients at 6 months was associated with Spanish language and living in Austin in bivariate and multivariable analysis (Table 3).
Multivariable Logistic Regression Analysis of Factors Associated with Completing the Survey at 6 Weeks.
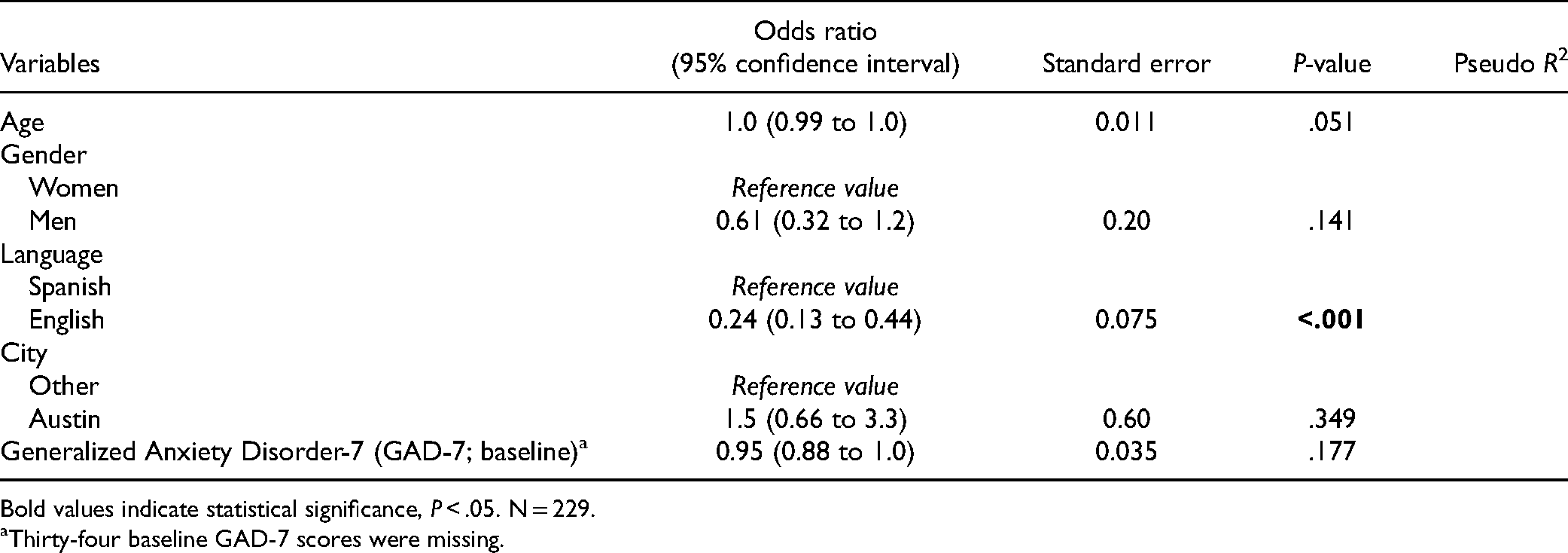
Bold values indicate statistical significance, P < .05. N = 229.
Thirty-four baseline GAD-7 scores were missing.
Multivariable Logistic Regression Analysis of Factors Associated with Completing the Survey at 6 Months.

Bold values indicate statistical significance, P < .05. N = 594.
When patients were successfully reached, greater odds of completing the survey at 6 weeks was associated with older age, women, speaking Spanish, fewer symptoms of anxiety, and fewer symptoms of depression in bivariate analysis. In multivariable analysis, greater odds of completing PROMs at 6 weeks were independently associated with older age, Spanish language, and lower symptoms of depression at baseline (Table 4). Greater odds of patients completing the survey at 6 months were associated with women and speaking Spanish in both bivariate and multivariable analysis (Table 5).
Multivariable Logistic Regression Analysis of Factors Associated with the Ability to Reach Patients by Phone at 6 Weeks.

Bold values indicate statistical significance, P < .05. N = 263.
Multivariable Logistic Regression Analysis of Factors Associated with the Ability to Reach Patients by Phone at 6 Months.

Bold values indicate statistical significance, P < .05. N = 594.
Among all patients, greater odds of completing PROMs at 6 weeks was associated with older age, women, Spanish language, living in Austin, and fewer symptoms of anxiety. In multivariable analysis, greater odds of completing the survey were associated with speaking Spanish (Table 6). Greater odds of completing the survey at 6 months were associated with women and speaking Spanish in bivariate and multivariable analysis (Table 7).
Multivariable Logistic Regression Analysis of Factors Associated with Completing the Survey at 6 Weeks for Patients Who were Reached by Phone.

Bold values indicate statistical significance, P < .05.
The Generalized Anxiety Disorder-7 was omitted from the model due to multicollinearity with the PHQ-2/9 (ρ = 0.66; P < .001). N = 107. Sixteen baseline PHQ-2/9 scores were missing.
Multivariable Logistic Regression Analysis of Factors Associated with Completing the Survey at 6 Months for Patients Who were Reached by Phone.

Bold values indicate statistical significance, P < .05. N = 246.
Discussion
Health care organizations would like to measure PROMs longitudinally to be able to measure the value of their care, but it is not clear this is feasible. In research settings, there is some evidence that phone calls have higher response rates than other forms of communication (8), but in our experience, response rates are low no matter the method of communication. In the setting of an alternative payment model that includes longitudinal PROM measurement as a quality/value metric, substantial resources were devoted, and yet it was difficult to reach people, and participation was limited, with some variation by psychosocial factors.
This study has several limitations that should be kept in mind. First, readers should take care when interpreting the data regarding patients receiving 6-week phone calls (which was selective) and patients receiving 6-month phone calls (routine). That said, the similarities in the rate of response and factors associated with participation are notable. Second, the specific rates may apply best to our setting, although, based on parallels with research in several settings in the United States, they seem representative. And the statistical associations only depend on variation within the sample and are likely more easily reproducible. Third, there are socioeconomic factors that may influence whether patients can be reached by phone (e.g., not being able to pay the phone bill) and we could not account for these factors in our analysis. Finally, while our research assistants called patients into the evenings and occasionally on weekends, the fact that most of the calls were during business hours may bias response in favor of patients who are retired, who have flexible jobs, or who are unemployed.
The finding that Spanish speakers were more likely to answer a 6-week and 6-month phone call and complete PROMs, may indicate the influence of personal and cultural factors on patient interest in participating in research or differences in care utilization (13,14). Cultural differences between Spanish and English-speaking patients—such as greater deference or respect, greater appreciation for the care, or other factors—may account for the difference in response rate, but we did not study these factors. Within our practice, a noteworthy proportion of clinicians are proficient in Spanish, which may increase the response rates. There is evidence suggesting that Spanish speakers tend to be more satisfied by language–concordant relationships with their physician (15–17).
The observation among the subset of patients who were reached by phone that fewer symptoms of depression and speaking Spanish were associated with completing PROMs suggests that longitudinal collection of PROMs will be less successful among people experiencing mental health opportunities. It is known that greater symptoms of depression are associated with greater symptom intensity and magnitude of incapability (18–23), which may be related to willingness, or perceived capability, to participate. These findings are in line with the notion that there are important psychological differences between people who stay in care and those who do not. The overall low participation in the longitudinal collection of PROMs is consistent with the published experience of others. People may not participate unless they feel it benefits them directly or unless they feel gratitude for the benefit received in the form of a diagnostic or therapeutic intervention.
This study of patients with upper-extremity illness found that participation in longitudinal completion of PROMs is low even when patients receive a personal call in their preferred language. We also found that the most important factor influencing participation is psychosocial. We know from other studies that most patients see a specialist once and then deprioritize care (24). The current study adds that people also tend not to answer a phone call from the office and that even if reached, may decline to repeat PROMs. It would be useful to know whether people that deprioritize care or participation in longitudinal PROM measurement had their needs met, felt the care was not useful and worthwhile to continue, or if the symptoms have resolved or been accommodated. Future research might also address strategies for improving participation in longitudinal completion of PROMs in musculoskeletal specialty care. And it is possible that longitudinal tracking of PROMs is not possible and other strategies such as text messages with a facile response addressing whether or not a person’s needs have been met. These findings may also support efforts to transform the way we monitor care toward more objective and feasible measures of health (e.g., tracking of mobility and activity using smartphones).
Footnotes
Authors’ Note
This study was approved by the institutional review board at the University of Texas at Austin (FWA #00002030). This article does not contain any studies with human or animal subjects. Informed consent for patient information to be published in this article was not obtained due to a waiver of informed consent because the data is anonymous.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David Ring received royalties from Wright Medical (Memphis, TN, USA) for elbow plates of less than USD10,000 per year and Skeletal Dynamics for an internal joint stabilizer elbow between USD10,000 and 100,000 per year. David Ring is a Deputy Editor for Hand and Wrist, Journal of Orthopaedic Trauma, and Clinical Orthopaedics and Related Research and has received or may receive payments or benefits amounting to USD5000 per year. David Ring received honoraria from meetings of the AO North America (Wayne, PA, USA), AO International (Davos, Switzerland), and various hospitals and universities.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.