
Abstract
One-third of patients report disruption of sleep by overnight light. Importantly, light causes both immediate sleep disturbance and influences circadian function, a fundamental process underpinning high-quality sleep. Short bursts of light at night and/or lack of bright daytime light disrupt circadian alignment, leading to sleep deficiency. To improve understanding of 24-hour light patterns, we conducted a longitudinal study of light levels in intensive care unit (ICU) rooms. Over 450 room-days, we observed high variability, dim daytime light, and active dimming of natural sunlight in occupied rooms. Such noncircadian light patterns have multifactorial influences on sleep and are a key target for sleep improvement in the ICU.
Introduction
Poor sleep in the hospital, particularly in the intensive care unit (ICU), is a key determinant of patient satisfaction and healing (1, 2). Poor sleep in the ICU includes all domains of sleep deficiency: poor sleep quality, insufficient sleep duration, and irregular circadian rhythms. Promotion of circadian alignment is a critically important strategy for improving sleep in all of these domains (2).
Circadian alignment is controlled by a master biologic clock which is synchronized with the 24-hour day by external cues via a process called entrainment. Light is the most influential entrainment cue. The robustness of entrainment and vulnerability to disruption is determined by the timing, intensity (lux), and duration of a light dose (3). Normal human entrainment requires bright light exposure during the day (wake) period and dim or no light during the night (sleep) period. Daytime bright light interventions deliver at least 1000 lux and more typically deliver 2500 to 10 000 lux over 30 minutes to several hours (4, 5). During the night, when lux levels should be <10 lux, short bursts of bright light (eg, 5 minutes) at relatively lower intensities (eg, 100 or 250 lux) can cause circadian abnormalities (3).
Approximately one-third of patients report that nighttime light is disruptive to their sleep, and light is second only to noise for its impact among disruptors from the ICU environment (6). Studies of light measurements in the ICU demonstrate problems with both overnight and daytime light levels. During the overnight period, investigations show a pattern of dim overnight light punctuated with multiple, brief exposures to bright light. During the day, light levels are low and insufficient to promote normal circadian entrainment (7 –13). Median light levels in the morning can be especially low, and peak light intensity appears to be delayed occurring in the late afternoon (14).
Previous studies have obtained data regarding ICU light levels. However, these studies have been limited by short periods of observation and a focus on nighttime measures. To expand on these limited data and to assess both daytime and nighttime light levels as they change seasonally, we designed a longitudinal study of ICU light levels. The objective of this work was to improve understanding of 24-hour light patterns by measuring light intensity in medical ICU (MICU) rooms in each of 4 cardinal directions over several months and tracking changes in light levels with room occupancy.
Methods
Institutional review board approval was obtained for all study activities (HIC #1112009428). A waiver of consent was obtained. Light meters (Extech SDL400) were mounted in a standard location on the wall behind the patient head-of-bed in selected MICU rooms (14 –17). Five rooms were selected to represent all sectors of our MICU and the 4 cardinal directions of our exterior windows (Supplemental Figure 1). Rooms faced southwest (206), northwest (218, 228), northeast (240), and southeast (250). Light measures were taken every 10 seconds on a continuous basis from August 8, 2016, to January 4, 2017, with brief (minutes) interruptions each week to exchange SD cards and thus retrieve data. We also tracked room occupancy. No other patient data were recorded.
We analyzed light data overall, by room, by day-night status, by hour, by 4-hour time blocks, and by occupancy status. Day was defined as 06:00:00 to 21:59:59; night was defined as 22:00:00 to 05:59:59. Morning was defined as 08:00:00 to 11:59:59; afternoon was defined as 12:00:00 to 15:59:59. We analyzed light data via calculation of medians and interquartile ranges (IQRs); we tested differences in median lux between occupied/unoccupied rooms via Mann-Whitney analysis. We also analyzed the occurrence of light peaks. “Peaks” were defined as lux readings greater than 250 lux; “high peaks” as lux readings greater than 1000 lux. During data cleaning, we removed extreme outliers that occurred in room 228 and room 250 (values > 2000 lux) on a single day; this resulted in the removal of 290 out of 3.7 million light readings. No other day or room had extreme outliers.
Results
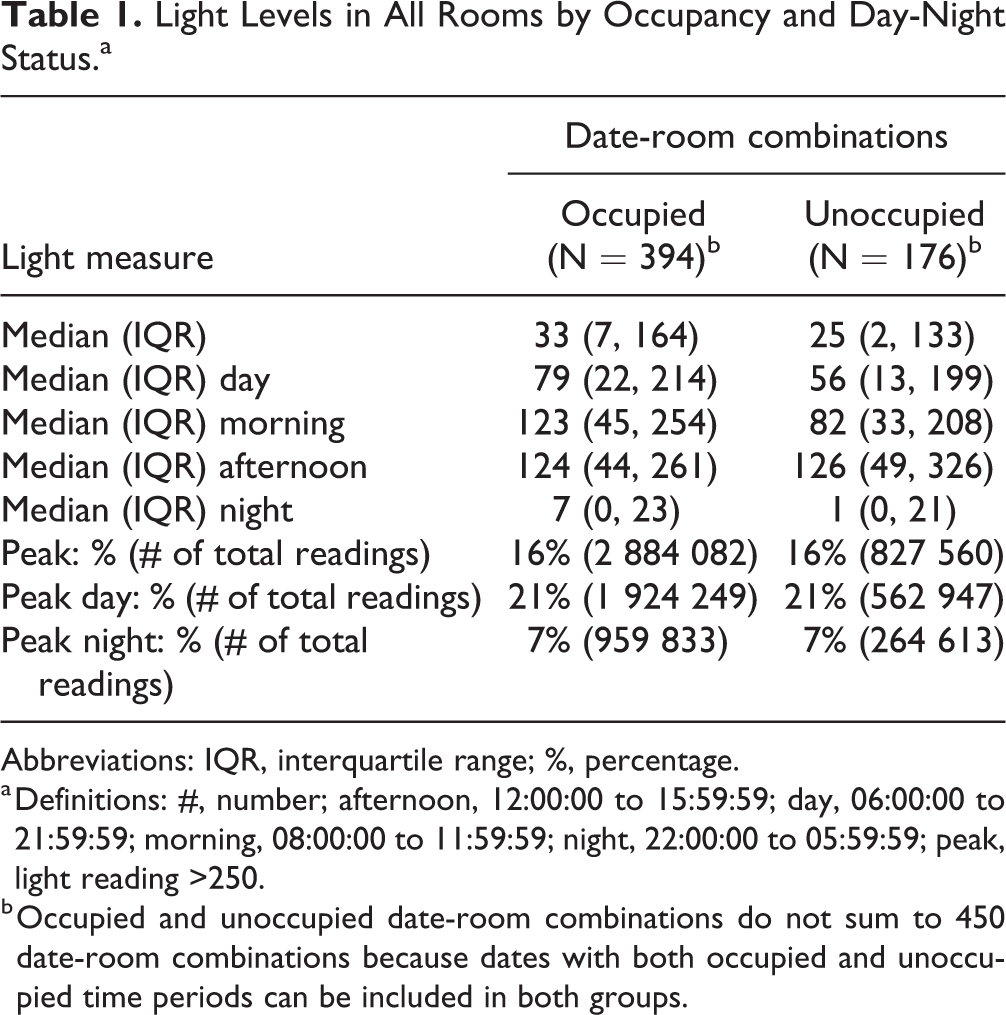
We analyzed light levels in 5 patient rooms over 143 unique dates and 450 room-day combinations (Table 1). The overall median (IQR) was 31 (6, 157) lux. The daytime median (IQR) was 74 (20, 210) lux, the morning median was 116 (41, 243) lux, and the nighttime median (IQR) was 5 (0,22) lux. By room, analysis demonstrated variation in light levels among rooms (Supplementary Table 1). Median daytime light levels ranged between 55 and 103 lux in occupied patient rooms and between 35 and 100 lux in unoccupied patient rooms.
Light Levels in All Rooms by Occupancy and Day-Night Status.a
Abbreviations: IQR, interquartile range; %, percentage.
a Definitions: #, number; afternoon, 12:00:00 to 15:59:59; day, 06:00:00 to 21:59:59; morning, 08:00:00 to 11:59:59; night, 22:00:00 to 05:59:59; peak, light reading >250.
b Occupied and unoccupied date-room combinations do not sum to 450 date-room combinations because dates with both occupied and unoccupied time periods can be included in both groups.
Analysis of peaks greater than 250 lux demonstrated peaks during the day and night with 16% of all readings being greater than 250 lux. Overall, 86% of all peaks greater than 250 lux occurred during the daytime hours and 14% occurred overnight; neither observation was altered by room occupancy. Regarding high peaks, <0.5% of all readings were greater than 1000 lux and, of these readings greater than 1000 lux, 62% of them occurred in unoccupied rooms; 0.0004% of them occurred at night in occupied rooms (eg, 5 instances of 12 074 readings greater than 1000 lux).
Variation in light levels depended on both time-of-day and occupancy (Figure 1). The highest median light levels were observed in room 250 in the morning period and room 206 in the afternoon period. Room 250 faces southeast and receives bright morning sun; room 206 faces southwest and receives bright afternoon sun. When unoccupied, room 250 had a median (IQR) lux of 408 (39, 672) during the 08:00 hour and a median (IQR) lux of 417 (52, 662) during the 09:00 hour. When occupied these values dropped significantly to 175 (41,398) and 203 (60, 465) for the 08:00 and 09:00 hours, respectively (P < .0000 for both). Similarly, when unoccupied, room 206 had a median (IQR) lux of 309 (119, 675) during the 13:00 hour; this dropped to 147 (74, 383) when the room was occupied (P < .0000). This pattern continued in room 206 during the 14:00 and 15:00 hour. Rooms 218, 228, and 240 had more moderate light levels that did not differ significantly by occupancy.

Hourly median light levels were calculated for each room by occupancy and are plotted as a solid line. Shaded regions show the first and third quartiles for each room.
Discussion
This longitudinal observational study of light levels in 5 MICU rooms demonstrates low day and night light levels. Light levels were noted to have high variance. This variance seems to be related to directionality and occupancy. Peaks are relatively rare, particularly in occupied rooms and in rooms without strong sun exposure.
The observed light levels are well below entrainment thresholds. Such low morning and daytime light levels would be expected to contribute significantly to circadian disruption in critically ill patients. Other studies have observed a similar pattern of low daytime light, high variability, and dim overnight light punctuated with multiple, brief exposures to bright light (14 –17). In addition, such observations are consistent with observed delays in circadian alignment in MICU patients (13).
Interestingly, increased light levels in rooms with higher natural light (eg, eastward room in the morning hours and westward room in the afternoon hours) are blunted when patient rooms are occupied suggesting that window blinds are being adjusted by staff or visitors (patients are not able to reachwindow blinds). Furthermore, this dimming of light may reflect a purposeful decrease in light due to staff, visitor, or patient preference. It is frequently the case in the MICU that patients cannot express their preference due to mechanical ventilation or delirium. This raises the possibility that in some cases staff preference or assumed patient preference is influencing light levels. This possibility is further supported by prior investigations showing that the most significant change in overnight light due to a sleep promotion protocol is for intubated patients (18).
Overall, we noted very few instances of patient exposure to bright light at nighttime. The more pressing concern in terms of circadian entrainment for critically ill patients may be insufficient exposure to bright light during the daytime, an observation also noted by several other studies (7 –13). However, since light levels in ICU patient rooms are extremely variable, it would be beneficial for institutions to implement baseline monitoring of light levels to identify the most problematic types of light exposure in individual rooms.
Limitations
There were limitations to this study. Most significantly, the details of patient illness severity and care needs such as mechanical ventilation were unknown which limits our ability to interpret the need for light as support of lifesaving medical care. Also, patient preferences were not known, and we thus cannot interpret fully the reason for lower light levels in occupied patient rooms. Our measures were done from a representative subset of MICU rooms, but the high room-to-room variation suggests that each local room environment is important. Finally, we measured light via a standard lux meter and did not incorporate more detailed spectral data; this may be an important avenue for future studies.
Conclusions
Our longitudinal study of ICU light revealed high variability, dim daytime light, and dimming of light levels during the day in occupied rooms. Such noncircadian light patterns have multifactorial influences on sleep and are a key target for sleep improvement in the ICU. Future research should investigate optimal lighting-based interventions that promote circadian alignment, sleep, and patient satisfaction.
Supplemental Material
Supplemental Material, sj-pdf-1-jpx-10.1177_23743735211033104 - Light Levels in ICU Patient Rooms: Dimming of Daytime Light in Occupied Rooms
Supplemental Material, sj-pdf-1-jpx-10.1177_23743735211033104 for Light Levels in ICU Patient Rooms: Dimming of Daytime Light in Occupied Rooms by Elizabeth R Lusczek and Melissa P Knauert in Journal of Patient Experience
Supplemental Material
Supplemental Material, sj-pdf-2-jpx-10.1177_23743735211033104 - Light Levels in ICU Patient Rooms: Dimming of Daytime Light in Occupied Rooms
Supplemental Material, sj-pdf-2-jpx-10.1177_23743735211033104 for Light Levels in ICU Patient Rooms: Dimming of Daytime Light in Occupied Rooms by Elizabeth R Lusczek and Melissa P Knauert in Journal of Patient Experience
Footnotes
Authors’ Note
Original data can be provided upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Knauert was supported by the National Center for Advancing Translational Science (KL2 TR000140) to conduct this project. Dr. Knauert is currently supported by the NHLBI (K23 HL138229) and the American Academy of Sleep Medicine Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.