
Abstract
On January 1, 2020, the Compulsory Mental Health Care Act took effect in the Netherlands. It contains provisions for compulsory community treatment (CCT) and compulsory treatment at home (CTH). In this study, we collected the opinions of patients and their significant others on CTH and on their preferences regarding compulsory care in their homes. Patients and their significant others were involved in the experience-based co-design of a purpose-built online questionnaire. This questionnaire was completed by 624 patients and 531 significant others.
Sixty-one percent of the patients and 62% of the significant others did not want compulsory treatment to take place at home but in hospital or elsewhere. Patients’ and significant others’ opinion showed few differences, except with regard to the involvement of the significant others in CTH.
As the respective views of patients and significant others were mixed, we recommend that crisis plans and compulsory treatment plans should be individually tailored to the needs and wishes of patients and their significant others regarding CTH.
Introduction
On January 1, 2020, a new Compulsory Mental Health Care Act took effect in the Netherlands. It has 3 main objectives: to improve the legal position of people with mental health disorders who receive compulsory care, to promote their participation in society, and to prevent compulsory admissions to psychiatric hospital. To achieve this, it includes provisions for compulsory community treatment (CCT) and compulsory treatment in the patient’s home (CTH).
Compulsory community treatment was already an option under the Netherlands’ previous mental health law. It could be invoked under 2 conditions: upon a patient’s conditional discharge (ie, discharge after a period of involuntary hospitalization) or if a patient was at home and represented a danger to themselves or others that could be averted by complying with certain conditions while living in the community. The use of compulsory treatment (eg, forced medication) in the place where the patients live was not permitted in the Netherlands until January 2020. Compulsory treatment in the place where the patients live is further referred to as compulsory treatment at home (CTH).
In the Netherlands, CCT (including CTH) is ordered by a judge after he or she has been informed by the public prosecutor, who in turn has been informed about the patient’s mental health by others, including an independent psychiatrist. Elsewhere, many other countries already work with CCT(1,2), which usually means that patients need to comply with a treatment plan—such as taking medication—in order not to be admitted (or readmitted) to hospital. However, we are not aware of any other mental health laws that permit CTH, which includes the actual use of forced treatment in the patients’ home. Compulsory treatment in patients’ homes could entail forcing patients to take medication or food at home, searching their house for drugs, locking them up in their room, or preventing them from leaving the house or seeing specific people. Potentially, such measures have a great impact on patients and the people around them—those to whom we refer to as significant others. Various studies have explored mental health workers’, patients’, and significant others’ opinions of CCT (see the review by Corring et al, 2019). These stakeholders experience ambivalence toward CCT, but Corring et al (3) conclude that all 3 groups saw benefits that outweigh the coercive nature of community treatment orders. We have found no studies that explored stakeholders’ views on CTH.
Therefore, the aim of this study was to collect the opinions of patients and their significant others on CTH on their preferences regarding compulsory care in their homes. We hypothesized that the majority of patients and significant others would be against CTH.
Methods
This cross-sectional survey was conducted as part of a national guideline-development trajectory intended to inform the implementation of the new mental health law in the Netherlands. The survey was developed, and the data underlying it were collected, by MIND, a Dutch umbrella organization for mental health that unites different patient and carer organizations. MIND acts as an advocate for mental health patients and their significant others on several important issues, including patient rights and quality of care. It also runs Een Krachtige Stem (A Powerful Voice), a program that supports the representation of patient and family values within the development of guidelines.
To include the perspectives of patients and their significant others, the guideline-development group concerned with implementing the new mental health law used elements of experience-based co-design (4), an action-learning–based model for democratic patient participation. Usually, experience-based co-design consists of 8 consecutive phases, toward the end of which patients and health care staff discuss and develop service improvements (5). In this case, however, the guideline-development group decided to move discussions between representatives of patients, significant others, and health care professionals to the start and middle of the process. Between meetings, time was used for each representative (eg, patients and significant others, psychiatrists, a psychologist, a nurse, a general practitioner, and a therapist) to collect views from their respective stakeholders that would inform their input. By increasing the support base within stakeholder groups, it also increased the relevance of guideline recommendations for all the stakeholders involved.
Through this adaptation of experience-based co-design, the 4 patient and family representatives in the guideline-development project group could use the survey to ask patients and significant others for their opinions on several aspects of the new mental health law. The representatives were regarded as co-researchers. To gather the information they needed in order to represent their peer group, they compiled a questionnaire, holding a focus-group meeting with the 2 patient representatives and 2 family representatives to help specify the questions it should contain. During the meeting, which was held in mid-October 2019 and was led by MIND’s lead project officer for the program (D.M.), participants explored relevant issues and formulated questions that eventually constituted the definitive questionnaire.
Participants for the survey were approached in 2 different ways. First, we approached MIND’s panel of members who participate in surveys (n = 4200). This is composed of present and former mental health patients and significant others who voluntarily participate in surveys on a wide range of topics. Second, to reach a wider range of present and former mental health patients and their significant others, we used additional methods, such as social media (including Twitter and Facebook) and online newsletters from MIND and their affiliates.
The final questionnaire consisted of 28 questions: 3 open-ended questions, 13 closed questions, and 12 questions that respondents were asked to rate on a Likert-type scale. The questionnaire is available upon request. Its questions were designed to elicit respondents’ opinions on 3 subjects: (1) the prevention of all compulsory care, (2) compulsory treatment in the community and in the patients’ homes, and (3) the role of significant others in CCT and CTH. For the patients, 1 question was added about personal experience with compulsory care in the past (yes or no) and, for significant others, whether they had experience with compulsory treatment for the patients they cared for.
The following textbox shows the questions that specifically targeted opinions on CTH, which we analyze in this article.

Results
Participants
This study had 1155 participants: 624 patients and 531 significant others (Table 1). Two hundred twenty (35%) patients did have previous experience with compulsory care, either in a hospital or in the context of CCT or both, as did 383 (72%) significant others. Most of the respondents were members of the MIND panel (78%).
Patients and Significant Others With and Without Experience of Compulsory Care.

Opinions of Patients and Significant Others on CTH
Table 2 summarizes the results of the questions on CTH. Sixty-one percent of the patients and 62% of the significant others would not want compulsory treatment to take place at home but in hospital (45% of patients; 43% of significant others), or elsewhere (16% of patients; 19% of significant others). Thirty-five percent of the patients with experience of compulsory care and 42% of those without experience would prefer CTH rather than compulsory treatment in a hospital or elsewhere. The percentages for the significant others were similar: 36% with experience would prefer CTH, and 41% without experience would do so.
Patients’ and Significant Others’ Responses to Several Statements Concerning CTH.
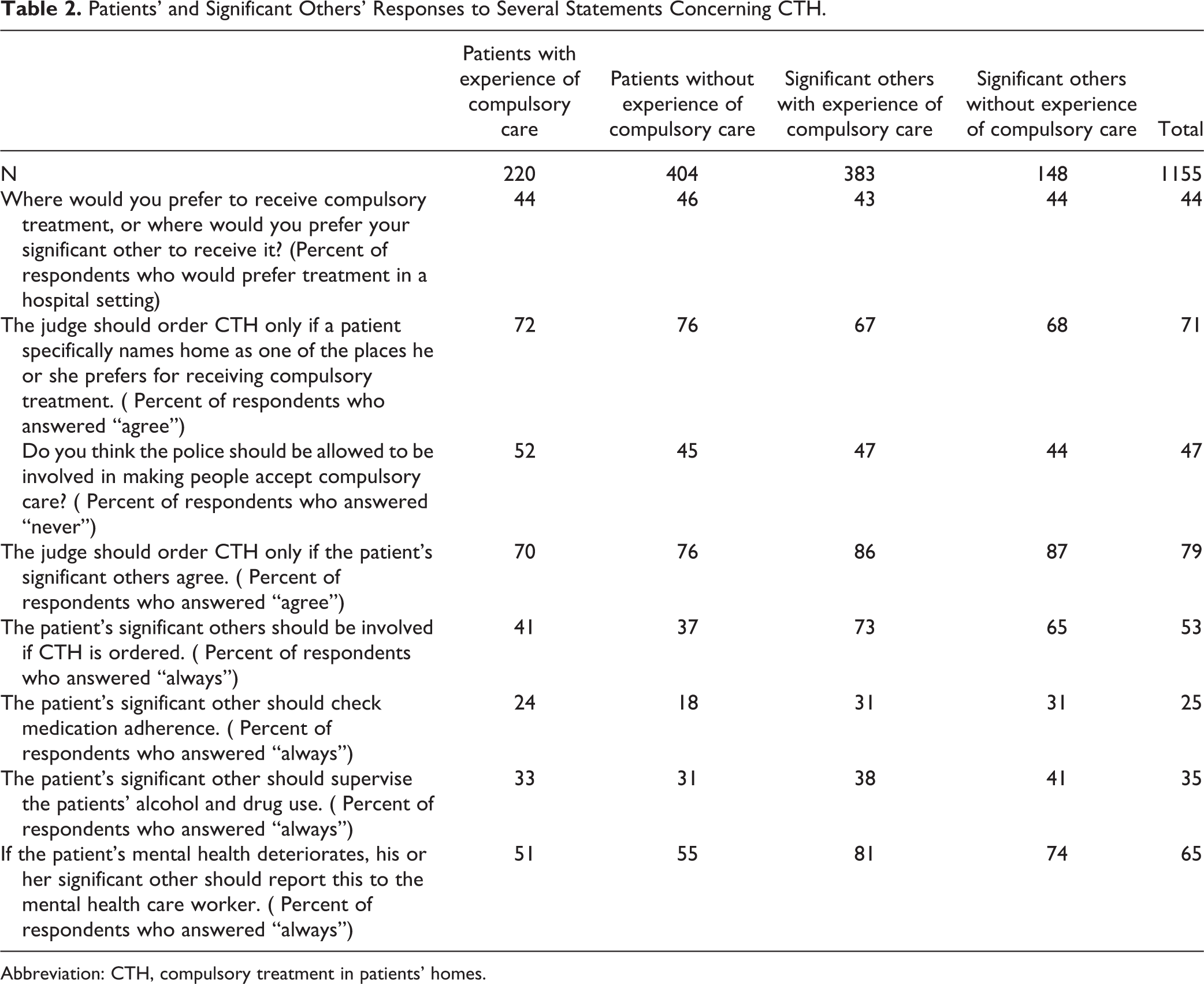
Abbreviation: CTH, compulsory treatment in patients’ homes.
Most participants (71%) agreed with the statement that CTH should be ordered by a judge only if a patient expressed a clear preference for CTH rather than for involuntary treatment in hospital. There were only small differences between patients with experience of compulsory care (72%) and those without (76%) and between significant others with experience (67%) and those without (68%).
Regarding the involvement of police at home, a little over half of the respondents (53%) thought that there were circumstances in which police involvement should be allowed, even at home. This held for 52% of the patients with experience and 45% of those without experience and for 47% of the significant others with experience and 44% of those without.
Involvement of Significant Others in CTH
With regard to the involvement of significant others, nearly 75% of the patients and over 86% of the significant others agreed that CTH should only be ordered if significant others agreed. About 40% of the patients would want their significant other to be involved in the planning and monitoring of CTH. In contrast, 70% of the significant others thought they should indeed be involved in this.
Twenty-four percent of patients with experience of compulsory treatment and 18% of those without this experience agreed that their significant other should check on their medication adherence. Thirty-one percent of the significant others also thought this, irrespective of their experience of compulsory care.
With regard to patients´ alcohol and drug use, 33% of patients with experience and 31% of those without it thought that the significant other should check on this. Thirty-eight percent of significant others with experience agreed with this, as did 41% of those without.
A little over half of the patients (51% of the patients with experience and 55% of the patients without) indicated that they would always like their significant other to report any deterioration in their mental health to the mental health services. Eighty-one percent of the significant others with experience agreed, as did 74% of those without experience.
Discussion
As we hypothesized, the majority (two-third) of patients and significant others were against CTH. However, one-third was not. Interestingly, our findings also suggest that the opinions of participants with and without experience of previous compulsory care do not differ greatly on this topic. Neither do the opinions of patients and their significant others.
The fact that one-third of patients and significant others was not opposed to CTH means that this option should be considered when deciding on a compulsory treatment plan, given that it is now allowed by Dutch mental health law. The Dutch Association of Psychiatrists, however, states that psychiatrists are advised not to use this option in practice (6), given doubts about the physical safety issues that arise when applying CTH. So far, anecdotal evidence indicates that indeed in 2020 CTH is rarely applied, although no formal statistics are available yet.
The majority of the participants (79%) agreed that CTH should be ordered by a judge only when (1) the patient specifically preferred home as the place he or she wishes to receive compulsory care and (2) his or her significant others agreed with the use of CTH.
The Netherlands’ 2020 Compulsory Mental Health Care Act states that admission to hospital should always be a last resort and that treatment at home is to be preferred if the circumstances allow it; yet, we found that 44% of the participants would prefer hospitalization to CTH. Literature into the experience of patients with CCT illustrates that CCT also has disadvantages such as the loss of autonomy and the degree of coercion experienced at home (7,8). Which in our opinion means that we should keep options open and evaluate patients preference.
One matter on which the patients’ opinions clearly differed from those of the significant others concerned the extent to which the latter would be involved in CTH. The number of significant others who wanted to be involved was much higher than the number of patients who wanted this involvement. There are several possible explanations for this: that patients would not wish their significant others to become their mental health workers; that they would wish to maintain their autonomy in the relation to their significant others; or perhaps that they would not wish to impose on their significant others.
Possible reasons why significant others want to be involved in the treatment could be helping in the recovery of the patient, making sure the patient receives the best of care, their ability to recognize symptoms sooner than mental health workers because they know the patient better, and sometimes significant others are also involved in the day-to-day care.
While we think it is very important to respect the patients’ wishes, since he or she is most directly impacted by the compulsory treatment, we would advise to try and find out why it is patients would not want their significant others to be involved.
Significant others’ involvement can play an important role in the recovery of people with severe mental disorders (9). Also the involvement of significant others can improve significant others’ quality of life (10 –12). In a review of stakeholders’ perspectives on barriers to family involvement, Landeweer et al (13) found that different perceptions of barriers were a barrier in themselves. To guard against this, the authors recommended that stakeholders take a dialogical approach to identifying each other’s perceptions of family involvement (13). In our view, this might also foster mutual understanding between patients and their significant others and agreement regarding the distribution of responsibilities in cases of CTH.
Implications for Clinical Practice and Future Research
Given the patients’ and their significant others’ clear and sometimes diverging views on the mental health legislation, we recommend their further involvement in researching, developing, and implementing guidelines on compulsory care in each jurisdiction. To facilitate shared-leadership roles, this involvement should be organized democratically (14) at all levels of care. Delivery of care should best be tailored to the specific patient. This is key in using evidence-based practice as a guide to deliver patient-centered care (14).
We also recommend the development and implementation of tools for supporting significant others in the compulsory care of patients with serious mental illnesses. Although such tools for support are important for all types of carers, health care professionals and researchers need to be aware of those significant others that care for patients with serious mental illness based on feelings of obligation because of their relationship to the patient (11). Zegwaard et al (11) describe these type of significant others as “type 2 carers” and identify several important themes to address in supporting them. They describe the support of carers’ coping through helping them understand the severe mental illness, on one hand, and focusing on themes regarding psychosocial well-being such as relationship tensions, autonomy, social isolation and loneliness, feelings of grief, and feelings of entrapment, on the other hand.
Finally, we recommend to use the results of this study for the implementation and evaluation of new mental health acts. Especially when the possibility of the extension of CCT into CTH is considered.
Strengths and Limitations
Strengths
To our knowledge, this is the first study of patients’ and significant others’ opinions of CTH. It has been performed via shared leadership (10) with a patient-led approach. Its design in co-creation with these stakeholders ensured that the questionnaire covered the topics that were important to them. Furthermore, compared to other studies into the opinions of patients and carers regarding CCT and CTH, a large group of patients and significant others participated in this study.
Limitations
As the survey was strictly anonymous, we had no information on the participants’ age, gender, or diagnosis. For this reason, we could not explore any differences in opinions between specific subgroups.
A relatively small part of the participants were patients who had experienced involuntary care (19%), compared to relatives who had experience with involuntary care (33%). So the views of patients with experience might be underrepresented.
As the participants in the survey were patients and significant others who had signed up voluntarily and were, therefore, intrinsically motivated to express their opinions, they may not have been fully representative of the whole population of people who are likely to receive compulsory treatment.
Conclusions and Implications for Practice
Roughly two-thirds of the participants would not want compulsory treatment to take place at home, but would prefer an hospital or other setting. One-third, however, would prefer CTH to treatment in hospital. Most patients and significant others agreed that a judge should order CTH only if this was also what the patient preferred.
Patients and significant others seemed to agree on most points, except on the extent of the significant others’ involvement during CTH, with the patients wanting this to be lower than the significant others did.
We suggest on the basis of our findings that clinicians tailor compulsory treatment plans to an individual patients’ needs and wishes and, when possible, also involve their significant others.
Compulsory treatment plans should not be written in a situation of crisis, but in advance, if possible, and should be evaluated afterward.
Footnotes
Authors’ Note
DM collected the data. DW and DM wrote the first draft of the manuscript. AW conducted the analysis on the data. All authors took part in interpreting the data, writing, adjusting, and finalizing the manuscript. All authors read and approved the final manuscript.
The data set used during the current study are available from the corresponding author on reasonable request.
This study falls outside the remit of the Medical Research Involving Human Subjects Act, and no further ethical approval was, therefore, required. We did not collect any identifiable personal data. Participants were informed that the data would be used for a scientific publication.
Acknowledgments
The authors thank the patient and family representatives from the guideline-development project group from MIND for designing the questionnaire and the patients and significant others that filled out the questionnaire for participating in this survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.