
Abstract
Multiple sclerosis (MS) is one of the most common, nontraumatic, disabling diseases diagnosed in adults. Self-empowered patients and families are valued members of the MS research team. The objective of this study was to explore patient and family perceptions of the influence of psychosocial state on their willingness to be research partners. Researchers conducted 5 focus groups with MS patients and family from the Upper Midwest Chapter of the National Multiple Sclerosis Society. The researchers asked questions addressing psychosocial factors influencing ability and willingness to work with MS researchers as partners. Relevant themes were identified including comfort level of individuals in formulating research questions, comfort level engaging in research, understanding of the meaning of research and self-perception about skills, research training, and knowledge needs. The findings of this study support the role of MS patients’ perspectives about MS, their understanding of the science of MS, and role of their psychosocial states as all these factors were patient identified as being key to their ability to be active, engaged and willing research participants.
Introduction
Multiple sclerosis (MS) is a disorder of the central nervous system (CNS) characterized by inflammation, demyelination, and degenerative changes. Multiple sclerosis is multifactorial in its etiology or triggering event (1). Multiple sclerosis is an immune-mediated, CNS disease causing both white and gray matter damage leading to widely variable symptoms (2). The impact of MS and its symptoms and severity vary by disease types and can manifest as either relapsing, purely progressive, or progressive with relapsing disease types (2). There is wide variation in symptoms and disability frequency and severity (3 –5). Even patients with the same MS type may have different, fluctuating symptoms (1).
Multiple sclerosis research has increased over the past decade leading to more therapeutic and symptomatic management options and increased focus on patient quality-of-life measures. The 15 disease modifying therapies (DMTs) are neither curative nor improve prior symptoms. Therapies suppress inflammation, relapses, and new lesions on magnetic resonance imaging (6). Multiple sclerosis has a significant impact on quality of life and is one of the most commonly occurring disabling, neurological diseases, most often diagnosed in adults 20 to 40 years. Multiple sclerosis has lifelong, physical, social, mental, and economic complications. The continuum from initial symptoms to diagnosis acceptance and daily symptom management is complex for all involved. Furthermore, patients must be committed to self-empowerment and health promotion in order to optimize symptom management over the course of this lifelong disease (7). With self-empowerment, the patient believes in their ability to influence change, like innovative MS treatments, that may improve their health (8).
Patient-centered outcomes research requires patients to be active partners with scientific investigators. The larger research project aimed to help patients and their caregivers make informed decisions about participation as research partners. Patients as research partners is core to Patient Centered Outcomes Research Institute (PCORI) mission (9). The PCORI sees empowered patients as valued members of the patient-centered research team. As such, they contribute an understanding of diseases through lived experiences. Personal experience aids researchers in streamlining creation and application of new knowledge of treatments and services (10). When patients are actively engaged as research partners, they are empowered to offer a first-person perspective and there is potential to heighten the credibility and validity of the results and democratize the research process (11). As research partners, patients offer unique insights that may impact research translation into clinical practice (10). For MS patients and their families such insights include sharing psychosocial or quality-of-life disease implications with researchers potentially influencing research direction and results (10). The research results will ultimately better serve those affected, particularly if patient partners are engaged authentically, are not included simply as tokens, and the research is inclusive of the most highly affected (11,12). However, previous studies indicated that the psychosocial state of MS patients and families may impact their willingness and motivation to engage in patient-centered outcomes research (11,13). To successfully engage MS patients and their family members, efforts to understand their perspectives are needed. Therefore, this study aims to explore patient and family member perceptions of how their psychosocial state influences their willingness to serve as research partners alongside researchers.
Methods
As part of a larger study, semistructured, qualitative focus groups were used. A total of 5 focus groups were conducted from April to June 2017. Groups were selected from 5 Mid-western states. Researchers recruited a representative sample of patients and family members from an established network of approximately 17 000-member, Upper Midwest Chapter of the National Multiple Sclerosis Society (NMSS), an organization raising funds for quality of life, MS research (14). Participants were recruited from Fargo, North Dakota; Sioux Falls, South Dakota; Des Moines, Iowa; Hudson, Wisconsin; and Minneapolis, Minnesota. After the invitation to participate in the study, those who agreed were given detailed, written information about the project. Contact information was requested to provide notification of focus group meetings. Participant information was deidentified to maintain confidentiality. Study procedures were approved by the Institutional Review Board at South Dakota State University.
Data Collection, Coding, and Analysis of Qualitative Data
The researchers used relevant literature to devise 36 guiding questions (15 –18). Questions aimed to address the overall study objective to determine perceived information patients and family members need to work as effective research partners. Examples specific to psychosocial state and MS research engagement on which participants were asked to elaborate include: How do you feel about the MS treatment? What are your concerns with working side by side with MS researchers? How comfortable are you if you need to raise a research question? Why or Why not? How comfortable are you if you need to give feedback or comments on how MS scientists or researchers design their research studies? How comfortable are you if you need to help MS Scientists and researchers interpret results? How comfortable are you if you need to help disseminate the research results?
For participant convenience, focus groups were juxtaposed with other scheduled NMSS activities. Written, informed consent was obtained from all participants prior to participation. Focus groups opened with an experienced group facilitator describing the goals of the project. Permission was obtained to audiorecord each session. Participants received US$100 honoraria for participation, travel, and incidentals.
Focus group responses were digitally recorded. Sessions were transcribed verbatim by a single researcher and then reviewed and analyzed by 2 research team members. To help ensure integrity, the content analyses followed guidelines recommended by Shenton and colleagues (19).
For data analysis, 2 researchers analyzed content to generate keywords and themes to create a coding scheme using both deductive and inductive methods. Initial coding categories were based on the discussion topic framework. Both researchers reviewed each transcript and identified relevant themes and codes. The 2 researchers compared codes and arbitrated differences.
N-Vivo 11 qualitative software (QSR International) was used for analysis. This program generated a Jaccard’s coefficient calculated to compare similarity of 5 different site responses to one another and determine saturation of information. It is important to note, however, that attaining saturation was not an intended goal of this project. The Jaccard Similarity Index is a single number, a function of scores resulting from value comparisons measured between the same attributes in each sample calculated as J = C/N, where C = # of themes represented in common between 2 focus groups and N = # of new themes emerging for each site (19). Jaccard scores range from 0 (no agreement) to 1.0 (complete agreement). A score of 1.0 suggests saturation. Indices > 1.0 = dissimilar, between group data or emergence of new information (20). Additional content analysis was also performed. Findings are summarized below.
Results
Twenty-nine participants attended focus groups: 15 MS patients and 14 family members, caregiver, or friend. White participants = 26 (90%) and African American = 3 (10%) (Table 1). Wide-ranging employment included a retired military service person, politician, farmer, physician, and city employee.
Focus Group Participant Demographics.

Abbreviation: MS, multiple sclerosis.
Recordings were transcribed verbatim and pages reviewed for accuracy by the research team. Responses referred to psychosocial state based on MS diagnosis, understanding of treatments, research understanding, and willingness to engage as a research partner.
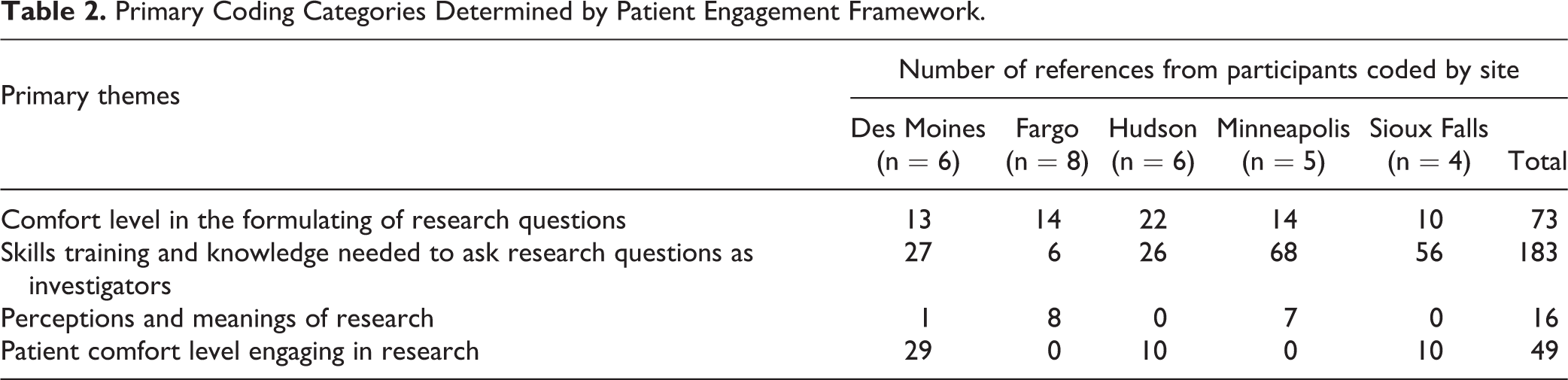
Participants were most vocal about Skills, Training and Knowledge Needed to Ask Research Questions as Investigators (total 183 mentions among all sites). Few comments were made about Perceptions and Meanings of Research (total 16 mentions among all sites). Knowledge, Skills, and training were recognized most often by Minneapolis and Sioux Falls participants (Table 2). Table 3 provides the results of the Jaccard Similarity Index. The greatest amount of word/phrase symmetry occurred between Hudson, Wisconsin, and Des Moines, Iowa (.588). Hudson and Fargo and Fargo and Sioux Falls had the greatest difference in words/phrases. Use of similar words or phrases were most common between WI and IA.
Primary Coding Categories Determined by Patient Engagement Framework.
Measure of Similarity/Dissimilarity of Concepts of Word/Phrase Symmetry Between Focus Group Sites.

In-depth qualitative analysis focused on 4 themes exemplifying patient and family ideas about research, design, and process. Specific emphasis was on psychosocial factors influencing willingness to engage in research alongside researchers. Prominent themes included Comfort level in formulating research questions, Skills Training and Knowledge Needed to Ask Research Questions as Investigators, Perceptions and Meanings of Research, and Comfort level Engaging in Research (as investigators). Thematic results are described below.
Theme 1: Comfort Level in the Formulating of Research Questions
Participants were asked: How comfortable are you raising a research question? Why or why not? Less than half of the participants who had a high comfort level developing research questions expressed interest in understanding why the phases of MS are different for each individual and why a particular treatment will work for 1 patient and cause problems for another. Participants expressed interest in exploring research questions on ways MS symptoms impact insurers and questions about how practitioners may intervene with payers to ensure treatment access.
Both patients and family members expressed discomfort or anxiety with sounding “dumb” or “uneducated,” affecting comfort level asking research questions. One participant said, “I try to learn but I feel that if I was talking to a researcher, I don’t know what I would add or give.” Several participants suggested they may be embarrassed to ask questions about symptoms such as sexual function, urination, and bowel movements.
Participants expected MS to “get in the way” of cognitive abilities. A few participants felt no need to participate in research having mild and atypical MS experiences. One participant suggested that he would ask questions that related to his own experiences with MS. Two participants expressed interest in complementary therapies but noted that some approaches like marijuana use may be sensitive or controversial topics.
Theme 2: Skills Training and Knowledge Needed to Ask Research Questions
When asked: What would make you feel confident or competent to engage in MS research? And, what kind of knowledge or skill sets do you need in order to engage in MS research? Participants discussed group qualities needed such as “group competence,” “understanding,” “resilience” or “coping,” and “honesty.” Participants emphasized that researchers should “be able to know how to explain…to somebody unfamiliar with [the disease] in a way that they’ll understand…” that trained researchers would require patience and need to be “exceptional teachers” to successfully instruct MS patients with “brain fog” and poor short-term memory. The majority of participants supported use of learning modules, simulation games, training manuals, and a shared vocabulary between MS patients and scientists.
When asked about knowledge needed to engage in patient-centered research, participants expressed a general interest in the biology of the MS disease, diversity in disease effects, inability to predict symptoms, biology of lesion formation in the brain, proposed causes of MS, and medication mechanism of action. Two participants suggested MS as part of a broader health policy agenda. Three participants asked to better understand and interpret complex statistical data. One participant was interested in disease heredity. Also, 2 participants noted needing assurance of continuity of care during research participation.
Theme 3: Perceptions and Meanings of Research
When asked: In your opinion, what is MS research? What does MS research mean to you? What does MS research do for you? Several participants said research meant increased MS treatment options for all disease forms. They cited frustration when reporting undocumented medication side effects, often told symptoms were unrelated to MS therapeutics. Participants suggested a willingness to participate as researchers in order to help discover better DMTs, curative options, and symptomatic alternatives to improve the quality of life for people living with MS.
Participants were asked: What do you think you know and the MS scientists or researchers don’t know? The majority shared that they did not believe researchers could fully understand MS if they did not themselves suffer from the disease. One participant noted that it would be helpful if MS researchers had personal experience with MS. The group suggested researchers do not understand emotional ramifications of the disease and how lack of personal experience may affect participation in research. Three participants suggested need for a skill set or experimental toolbox to allow them to effectively work those with varying perspectives.
Theme 4: Patient Comfort Level Engaging in Research
When asked about comfort level serving as research investigators, the majority of participants indicated they would engage if: they knew the research plan and goals. Several participants expressed motivation to engage was driven by the broken health care system, lack of treatment availability, care costs, and insurance issues. Patients were driven to participate in research that would improve health care delivery and access. Six participants emphasized the importance of incentives to patients who might take off work, drive long distances, or be the sole household earner. Patients stated they were willing to engage but not at great personal hardship or financial loss as this is also caused by the disease itself. Having an understanding of the value one brings to the research was also identified as a reason to engage and remain engaged. Lastly, 1 participant mentioned the ethical conduct of research as an important influence on willingness to engage as a research partner citing the Tuskegee experiment and the resulting research mistrust by African Americans.
Discussion
This study sought to explore MS patients’ and family members’ perceptions of the influence of their psychosocial state on their willingness to be research partners. Our research found 4 key themes concerning facilitators and barriers. Themes included comfort level forming research questions and engaging in research, understanding the meaning of research, and self-perception about skills, training, and knowledge needs. Themes were articulated in focus groups across 5 states.
Our study found participants who had minimal disability were more interested in a research partner role. Conversely, those experiencing debilitating symptoms expressed lack of interest to engage, suggesting consistent fatigue, mobility issues, cognitive deficits, and time commitment as constraints. For these participants, participation was perceived as a potential hardship.
The results revealed a need for preparation to engage in patient-centered outcomes research specific to MS. Recent research suggests appropriate training for patients in research partner roles (21–22). The PCORI also provided educational materials, Methodology 101 Training for Patients and Stakeholders, for this purpose.
Participants unlikely to engage shared little enthusiasm about potential research roles. For instance, participants who felt self-conscious indicated that MS impacted their cognitive abilities and caused insecurities. When asked about knowledge and skills they would need, participants could not visualize this role.
The MS disease experience has been associated with self-degradation and need for affection or social support. Hearld and colleagues found patients seeking social support were more likely to express interest in serving as a research partner (23). Our study, however, showed those expressing decreased self-perception to be less likely to express a willingness to engage in research or other productive activities. Since self-perception is a person’s self-portrait which includes intelligence, attractiveness, and individual needs among other characteristics (14), the research trainings for the patients with MS need to specifically accommodate certain MS-related insecurities that may surface and serve as a barrier to participate as a research partner.
Intuitively, one major concern for both the patients and family members concerned their own research skills. Although the majority of participants were able to demonstrate an adequate understanding of MS, its etiology, unpredictability, debilitating symptoms, and therapeutic options, several within the groups cited a desire to be able to read and interpret data from existing research studies. The majority of this group also expressed the need for researchers to articulate research findings in a way that would be meaningful to MS patients. Not understanding the need for the research or the value of their role in the study was of great concern to many participants and they acknowledged it as a key factor in deciding if to engage as a research partner.
Results from our study further suggest that the lived experience with MS varied among individuals in different geographic settings. Jaccard similarity results showed that patient and family member responses to focus group questions were at most 59% similar or they only mentioned similar themes a little over half the time. Jaccard responses between Hudson and Fargo were the least similar at 33% with participants addressing comfort level with asking questions and engaging in research and training needs more frequently in Hudson. These results are consistent with previous reports on differences in understanding and acceptance of uncertainty of the MS prognosis across geographic locations (23). They also confirmed the recommendation for diversity in stakeholders to ensure a variety of viewpoints and also inclusion of those experiencing the greatest illness burden, ensuring a health equity lens is incorporated into the research design and analysis (24,25). Although we were able to capture a diverse responses over 5 states, ours was a relatively small and nondiverse geographic area, within the Midwest. Future research, therefore, should assess these factors in other regions of the United States.
This research is strong in its focus on patient and family member perspectives on their willingness to serve as researchers alongside trained professionals. The patient and family member narrative provides the potential for new areas of research which may be driven by those most affected. Another strength is the geographic spread of the respondents in urban and rural areas within 5 Midwestern states. The researchers are allowed to discover differences in the MS experience that may be due to social determinants of health that vary within each of the participating sites. Particularly an area for future research should investigate access to services and care options that may vary across geographic locations and health systems and how these may impact health outcomes and the quality of life of both patient and family members. The ability to quantify participant responses is a strength that allows us to better illustrate the themes that emerged and clearly indicate which areas were of greatest concern and need for further study.
Although the qualitative methods capture the voice of the affected individuals, the inability to generalize findings to the population at large is a clear limitation. Future studies may conduct large scale surveys to determine whether the concepts identified in this research truly represent patient and family member attitudes and perceptions about the lived, MS experience and their willingness to participate as fellow researchers alongside trained scientists. This information may also serve as preliminary data to survey MS consortiums and support groups in other regions of the United States.
Conclusions
To enhance MS patient care, outcomes, and quality of life, patient-centered research is tantamount. Conducting patient responsive research while appreciating their values and preferences will result in the most meaningful data. Our findings contribute to research on the patient and family voice and their ability to serve as research partners. Many patients and family have difficulty visualizing themselves in an active, investigator role despite their lived experience. We should strive to appreciate these contributions. Doing so will improve the quality and applicability of such studies to the MS community as a whole.
Footnotes
Authors’ Note
Informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.