
Abstract
The American Academy of Pediatrics published expanded guidelines for infant safe sleep in 2011, expanding the definition from “back to sleep” to “safe to sleep,” more fully describing risk factors and guidelines. In 2016, the guidelines were revised to promote “providers modeling safe sleep behavior” to the highest level of recommendation. Previous studies have addressed the difficulty in creating clear, consistent communication between health care providers and families during an infant’s inpatient stay. This institutional update describes an interprofessional and family-centered quality improvement project to improve sleep safety for hospitalized infants through a multimodal approach. Five family-centered interventions were designed: a designated safe sleep web page, a clear bedside guide to safe sleep, additional training for nursing staff in motivational interviewing, a Kamishibai card audit system, and electronic health record smart phrases. These coordinated interventions reflect advantages of an interprofessional and family-centered approach: building rapport and achieving improvements to infant sleep safety.
Introduction
In 2011, the American Academy of Pediatrics (AAP) published safe sleep guidelines for infants younger than 12 months of age, which focused on recommendations regarding the sleep environment (1,2). Although it is not possible to change some risk factors associated with sudden unexpected infant death (SUID) and sudden infant death syndrome (SIDS), such as male sex, several of the greatest risk factors can be modified, including environmental factors such as bed-sharing, prone sleeping, or use of soft items in the sleep environment (3). In 2016, the AAP updated this guideline again, emphasizing the importance of health care providers modeling safe sleep behavior (4).
Hospitalization of an infant may be a critical time to improve modifiable risk factors for SUID and SIDS by providing education and support to families. Institutional policy change alone can influence safe sleep behaviors while infants are hospitalized, such as by transitioning infants from prone to supine, but may not reinforce enduring safe sleep behaviors (5). Bundled interventions can provide targeted education to caregivers regarding safe infant sleep (6). Direct education of nursing staff about tools for safe sleep interventions has also been shown to improve both nursing care provider knowledge, practice of safe sleep principles, and ease of communication with families (7). There are several challenges that can lead to poor adherence with safe sleep recommendations, including inconsistent messaging and lack of caregiver interest in safe sleep interventions (1).
Nursing staff at the Golisano Children’s Hospital have reported many of the same challenges and priorities that are present on a national level. In response to concerns about bed-sharing with hospitalized infants, caregivers were offered safe sleep videos via the GetWell Network, an in-room educational system. However, nurse managers reported rising incidence of bed-sharing despite education and reeducation efforts. An event reporting system captured some of these events, but nursing staff was not equipped with a toolset to address safe sleep concerns in real time.
In this project, tools were designed at Golisano Children’s Hospital that sought to clearly illustrate the importance of safe sleep, proactively partner with families, and support staff to prepare for and engage in sometimes challenging conversations with caregivers.
Materials and Methods
The working group for this project was composed of the Director of Quality Improvement for the Department of Pediatrics, a Pediatric Hospitalist, a Senior Advanced Practice Nurse in Pediatrics, Senior Associate Counsel for the Office of Counsel, and a medical student with a background in social work. The working group met several times to review literature and discuss improvements to safe sleep communication. The interdisciplinary nature of the working group allowed for a comprehensive approach to potential points of friction.
Five tools were developed to better communicate and reinforce safer sleep behavior throughout the course of a child’s care: prior to the hospital stay, during the hospital stay before unsafe sleep had been observed, and after unsafe sleep had been observed.
First, a designated page on the Golisano Children’s Hospital website was designed and implemented (Figure 1). For hospital staff, an intranet page was embedded in the web page. After a verified log-in, staff are able to access best practice guidelines from a single page. The designated safe sleep page also has a public interface that does not require a hospital-affiliated login. This page is useful for families prior to or during their infant’s hospitalization and can mitigate ambiguity with safer sleep guidelines. The web page can also serve as a community reference page for providers and families seeking general information on safer sleep.

Safe sleep web page.
Second, laminated bedside cards were devised to clearly communicate expectations and rationale for safer sleep for babies younger than 1 year of age (Figure 2). These cards are brightly colored and contain under 75 words, written at an approximately sixth-grade reading level with a photograph of an infant in a safe sleeping environment. The cards clearly communicate safe sleep expectations and allow families to initiate questions about safer sleep.
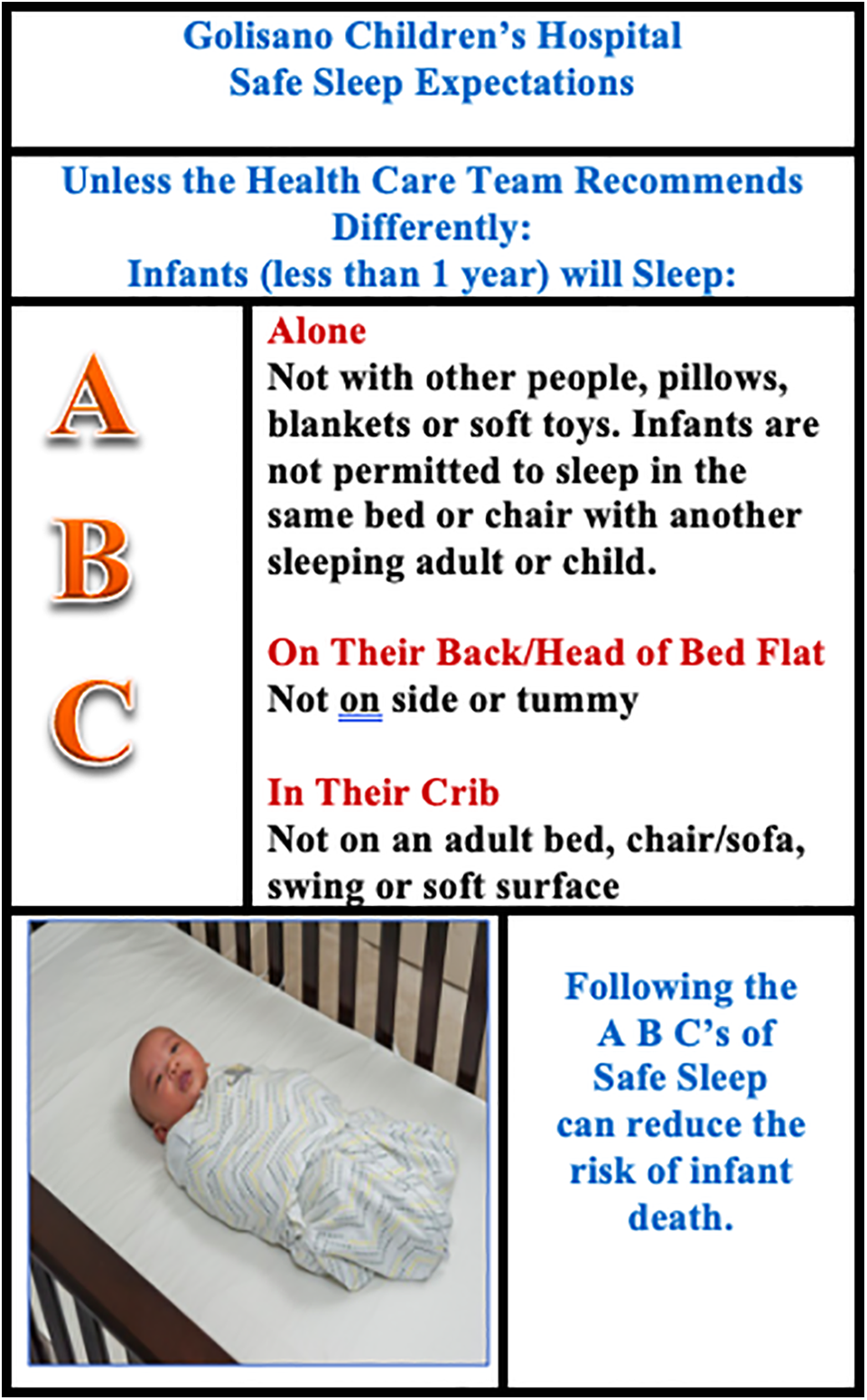
Safe sleep bedside card.
Third, suggested scripts for nurses or care providers who witnessed unsafe sleep were written based on a motivational interviewing model. Motivational interviewing is based in the transtheoretical model of change, a relevant basis for hospital-based interventions where families may be at different stages of change during their stay. There is significant evidence for motivational interviewing for parents to improve the sleep hygiene of school-aged children, but little research about the application of motivational interviewing to improve safe sleep practices for infants (8). The challenge of directly confronting parents is a primary point of hesitation in implementing hospital-based safe sleep guidelines (1). By focusing not only on the information to be shared, but the most effective way to share that information, this intervention sought to increase both the efficacy and the ease of conversations about safer sleep.
Fourth, a traditional safe sleep audit was replaced by Kamishibai Cards or K-cards (Figure 3). K-cards can assist in root cause analysis, especially important in situations such as bed-sharing that rely on behavioral analysis (9). The use of K-cards for children’s hospital quality improvement is based on a multisite study by Solutions for Patient Safety, a coalition of over 100 children’s hospitals; they been shown to improve quality improvement measures with respect to hospital acquired infections (10). K-cards are unique in involving the bedside nurse, in contrast to administrative management leadership of traditional audits. These real-time audits reinforce safe sleep parameters, build rapport for immediate change, and can help educate both families and nursing staff. This is the first noted use of K-cards for sleep safety audits.

Safe sleep K-cards.
Fifth, a smart phrase was implemented on in-house medical record software (Figure 4). Smart phrases provide an automatic drop-down menu for providers to better document behaviors not in adherence with safe sleep guidelines. By specifically and consistently identifying concerning behaviors, caregiver education can be more targeted toward those behaviors. Importantly, using smart phrases also mitigates documentation burden on providers.

Safe sleep smart phrase.
Results
A sample of 100 charts from Golisano Children’s Hospital at University of Rochester Medical Center were reviewed. Inclusion criteria included patients with an admission to the Pediatric Hospital Medicine service in the most recent 12 months who were younger than 12 months of age at discharge. The electronic medical record (EMR) search function was used to locate nursing and provider notes about safe sleep. Of the notes that mentioned safe sleep notes in the EMR search, 51% (n = 36) mentioned safe sleep briefly, 30% (n = 21) mentioned specific safe sleep guidelines, 38% (n = 27) mentioned specific concerns about safe sleep behaviors, and 35% (n = 25) mentioned specific plans for follow-up or continued monitoring. There was significant variety in the verbiage used to describe safe sleep behaviors. It should be noted that this review did not include the patient education record where free-text nursing documentation of routine safe sleep education was previously located, as this chart area is not routinely reviewed by interdisciplinary teams. The smart phrase intends to centralize and standardize this documentation.
A short survey was also conducted in order to assess how this safe sleep toolkit has been useful to care providers in the Children’s Hospital. This survey used a convenience sample of 8 participants in a quality improvement course who work at the Children’s Hospital. Participants included 5 physicians, a registered nurse, a nurse practitioner, and a health care professional student. These participants rated their average concern for caregivers not following safe sleep practices during inpatient stays as a 3/5, where 5 was concern about most caregivers and 1 was concerns only about the rare caregiver. Participants were also asked to rank the helpfulness of the 4 tools, where 1 was not helpful at all and 5 was extremely helpful. The safe sleep web page received an average score of 3.8/5, the safe sleep K-card averaged 4.6/5, the safe sleep script averaged 4.6/5, and the safe sleep smartphrase averaged 4.4/5. Participants also noted that the concise smartphrase was especially useful for integration into patient handoffs.
This convenience sample offers a clear insight that additional tools to improve hospital sleep safety are both welcome and necessary. Additional data are needed to determine whether educational materials are improving staff members’ willingness to have difficult conversations and improving sleep safety in inpatient units.
Lessons Learned
Clinical implications of this quality improvement project include (1) greater buy-in from providers, clinical staff, and families can be fostered by collaborative input and contributions in project design; (2) motivational interviewing can be used as a tool to reflect a cultural shift toward family-centered care; (3) motivational interviewing can ease and simplify communication around safe sleep; (4) simple access to information about safe sleep recommendations are well received by patients and providers, and their impact on safe sleep behaviors should be evaluated; (5) increased ease of safe sleep audits may increase provider adherence; (6) electronic health record templates can improve safe sleep oversight and adherence by standardizing verbiage; (7) documentation of the advice given to caregivers about safe sleep practices is an important part of managing legal risks of inpatient bed-sharing.
With the initial pilot implementation of the K-cards, staff reported increased ease of audits. Adherence to recommended safer sleep measures was a major barrier in previous attempts to improve institutional sleep safety (1). By making adherence easier, providers may be more likely to both participate in quality improvement tracking measures and follow-up with families directly.
Conclusions
The tools established in this project were designed and implemented with careful attention to practicality, impact, and replicability. The scripting, whiteboard, and K-cards were designed with input and contributions from unit safe sleep champions, pediatric leadership, and the interdisciplinary steering team. By using multiple sources of input to design an intervention that was truly desired, there was greater buy-in from clinical staff and families.
Motivational interviewing is used here as a tool to both reflect a cultural shift toward family-centered care and ease conversations for medical providers. These interviewing scripts, along with the website, K-cards, and whiteboards, provide clear and consistent messaging for families. The continued utilization of these tools reflects the importance of both consistent messaging around safe sleep and respecting families during challenging conversations.
Footnotes
Authors’ Note
Ethical approval is not applicable for this article. This article does not contain any studies with human or animal subjects. There are no human subjects in this article and informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.