
Abstract
Proning awake patients with COVID-19 is associated with lower mortality and intubation rates. However, these studies also demonstrate low participation rates and tolerance of awake proning. In this study, we attempt to understand barriers to proning. Medical and dental students surveyed nonintubated patients to understand factors affecting adherence to a proning protocol. Only patients who discussed proning with their medical team attempted the practice. Eight of nine patients who were informed about benefits of proning attempted the maneuver. Discomfort was the primary reason patients stopped proning. Addressing discomfort and implementing systematic patient education may increase adherence to proning.
Introduction
Patients infected with the novel coronavirus 2019 (COVID-19) are at risk of developing acute respiratory distress syndrome. Multiple small studies, both retrospective and prospective, have attempted to assess the efficacy of awake proning in COVID-19 (1 –7). One retrospective study of 10 patients found that 1 hour of awake proning led to improved oxygen saturation and a decreased respiratory rate (3). Caputo et al found that 5 minutes of awake proning in 50 patients who visited the emergency department improved median SpO2 from 84% to 94% (8). Another study found that awake proning improved oxygenation as measured by PaO2/FIO2 (5). These studies either do not assess barriers to proning or note poor tolerance of awake proning in a significant proportion of the population. One such study states that only 40 of 105 patients tolerated awake proning, while another found that only 11 out of 48 patients tolerated regular proning (1,9). In this mixed-methods quality improvement study, we aim to evaluate the patient experience of awake proning and understand the reasoning behind poor tolerance through phone interviews conducted by medical and dental school students. By understanding patient perspectives on proning and implementation of proning protocols, we hope to facilitate future research and implementation efforts related to improving the patient experience of prone positioning in nonintubated patients.
Methods
This study was performed at Massachusetts General Hospital from April 27, 2020, to May 20, 2020. Interviews were conducted over the phone. Inclusion criteria were age >18 years, tested positive for COVID-19 (reverse transcription polymerase chain reaction), and diagnosis of viral pneumonia defined by oxygen requirement and/or chest imaging with bilateral pulmonary opacities. Patients were excluded based on need for intensive care unit (ICU) admission, hospitalization >14 days, delirium or dementia indicated by clinical notes in the medical record, or if they were deemed inappropriate for interview by bedside nursing staff.
Patient demographics were collected by electronic medical record review. Physiological measurements were recorded at time closest to the interview. Medical interpreter services were used for patients with limited English proficiency. This study was deemed exempt from full review by the Partners Healthcare Institutional Review Board. All participating subjects provided verbal consent to participate.
Results
Two hundred and thirty-eight patients were screened for enrollment, and of those, 105 (36%) were eligible and were called. Of those called, 26 (25%) answered the call and 16 of those (59%) completed the survey and qualitative interview (Figure 1). The reasons patients declined included fatigue/malaise (n = 3), confusion (n = 3), inconvenient timing (n = 3), hearing difficulties (n = 1), and lack of interest (n = 1; Table 1).

Workflow of study protocol.
Patient Demographics and Characteristics on Day of Phone Call.
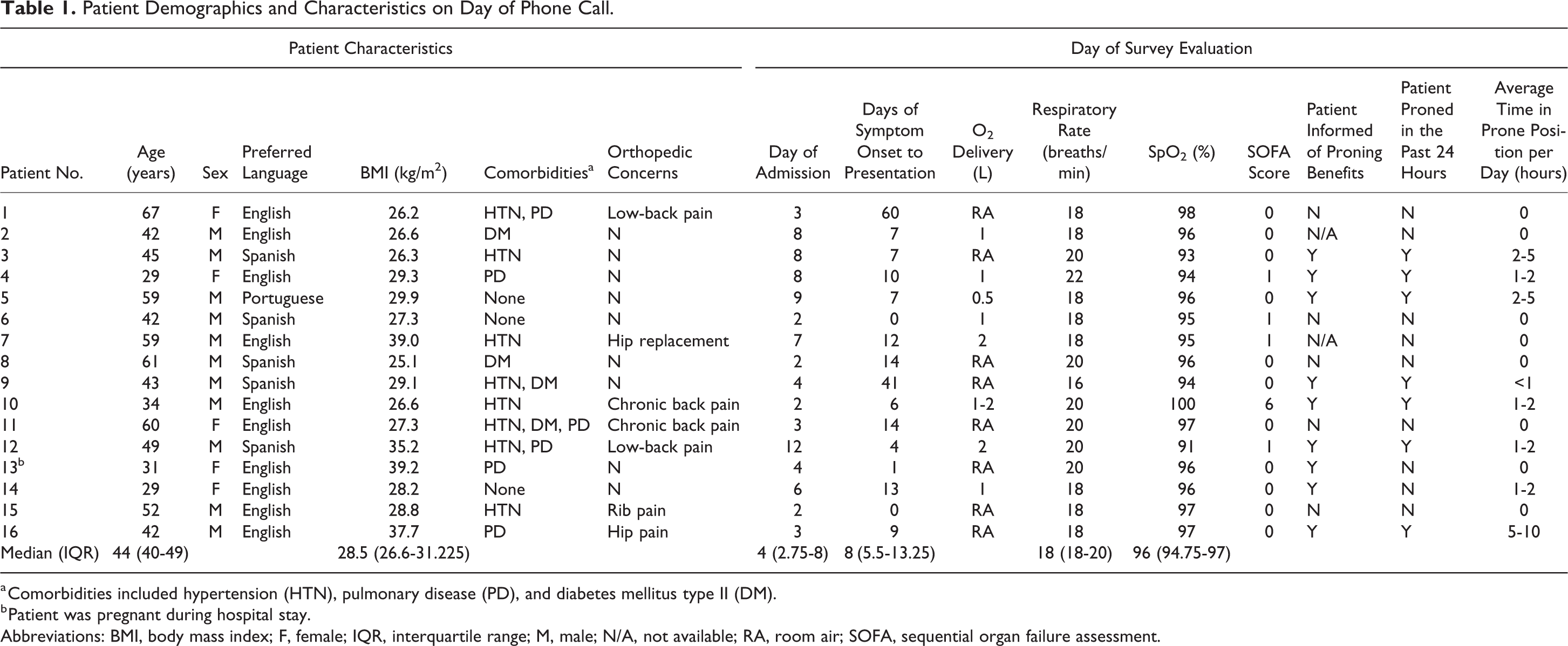
a Comorbidities included hypertension (HTN), pulmonary disease (PD), and diabetes mellitus type II (DM).
b Patient was pregnant during hospital stay.
Abbreviations: BMI, body mass index; F, female; IQR, interquartile range; M, male; N/A, not available; RA, room air; SOFA, sequential organ failure assessment.
Seven patients (44%) did not receive information about proning from their medical team, and none of those patients reported proning in the 24 hours before completing the survey. Nine patients (56.3%) received information about proning. Eight of these nine patients (89%) attempted proning. The 1 patient who did not attempt the maneuver was pregnant. Seven (77%) had used the prone positioning in the last 24 hours before the survey. All 8 patients who indicated they spent time in the prone position cited discomfort as the primary reason for being unable to continue. Factors contributing to discomfort included preference for a different position, orthopedic concerns, and obtrusive medical equipment. Orthopedic concerns listed in Table 1 had no effect on the likelihood of a patient to attempt proning (P = 1.0).
Discussion
Previous studies have shown the benefits of awake proning on physiologic measures and clinical outcomes but have provided little information on patient barriers to proning (2,5,6). Our study adds to the literature by evaluating the subjective patient experience. In this mixed-methods study, not being informed about the practice and discomfort were the major barriers to proning. Pregnancy also served as a barrier. While per hospital policy patients with COVID-19 were to be encouraged to use prone positioning as much as they could tolerate by their inpatient medical teams, many stated that they had not been informed of this protocol. As expected, we observed that patients who did not discuss proning with their medical team did not participate in proning. Although the sample size is small, this observation highlights the importance of systematic patient education in promoting the practice. Supplying information on potential proning benefits to patients in their native language before attempting the maneuver is also recommended for future studies.
Among those who attempted proning, discomfort was the primary reason patients limited their time in the prone position. This is a novel observation as previous proning studies either only included critically ill patients on sedating medications or did not solicit patient insights on barriers to awake proning. This finding is supported by the current literature which suggests poor adherence to proning for non-ICU patients (1,9). More information is needed regarding the types of discomfort patients experience in order to design interventions to address these issues. Current proning protocols, in our institutions and others, do not include assessments of pain or discomfort with proning. We recommended that future studies implement initial and repeat assessments of pain accompanied by recommendations on possible pain-relieving measures (eg, positioning, pain medication) to increase proning adherence. The authors believe that by improving educational efforts and addressing comfort-related issues, we will be able to improve proning compliance and therefore patient outcomes.
The strengths of our approach include a generalizable population as exclusion criteria were based solely on ability to participate in an interview. Additionally, our study allowed for open-ended patient responses.
This study also highlights the ability of medical and dental school students to leverage their skills virtually via telephone interviews with patients. The efficacy of these interviews is relatively unknown, but they are useful in employing the effective communication skills of physicians in training which allows for a wider range of contribution from different levels of healthcare providers. These telephone interviews allowed for new ways to conduct qualitative research in a population of quarantined patients and provided a sense of companionship between patient and interviewer. Utilizing the talents of these groups in novel ways can be of great benefit during the pandemic.
Limitations
Weaknesses of this study are the small samples and low completion rate. The low completion rate was largely due to patients not answering the phone in their hospital room when called. This highlights a challenge in conducting phone-based quality improvement studies dealing with hospitalized patients.
Footnotes
Authors’ Note
The study was considered exempt from IRB approval on April 3, 2020. Paul Currier and Rebecca Israel contributed equally to this work.
Acknowledgments
The authors are grateful for the contributions of Dr Joseph J. Locascio to the statistical analysis of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Massachusetts General Hospital Clinical Innovation Grant and the Harvard Catalyst Program which supported the statistical analysis.