
Abstract
Introduction:
Patient satisfaction is a commonly used indicator for measuring the quality of health care. This study assessed patients’ satisfaction with the quality of care at the National Health Insurance Scheme (NHIS) clinic in a tertiary facility.
Methods:
It was a descriptive cross-sectional study in which 379 systematically selected participants completed an interviewer-administered, semi-structured questionnaire. Data were analyzed using Statistical Package for Social Sciences (SPSS) version 23. Bivariate analysis was performed using Pearson χ2 with a P value set at ≤ .05.
Results:
The study found out that about half (193, 50.9%) of the respondents were satisfied with the availability of structure. Patients were not satisfied with waiting time in the medical records, account, laboratory, and pharmacy sections. Overall, 286 (75.5%) of the respondents were satisfied with the outcome of health care provided at the NHIS clinic. A statistically significant association (P = .00) was observed between treatment outcome and patient satisfaction.
Conclusion:
There is a need to address structural deficiencies and time management at the clinic.
Introduction
The increasing health awareness and easy access to health information have enabled patients to play an active role in decisions concerning the quality of care they receive (1). Assessment of patients’ satisfaction is relevant in the field of health management; this is because patients’ satisfaction is one of the main parameters in the assessment of health care quality (2). Patient satisfaction is simply defined as a patient’s judgment on the quality and outcome of care (3). In most developing countries like Nigeria, there is a lack of universal coverage of health care (4). This necessitated the introduction of health insurance for the individual to have access to effective, equitable, and efficient health care (4). The National Health Insurance Scheme (NHIS) is a social health insurance scheme in Nigeria designed to provide universal coverage. It was established under Act 35 of 1999; however, services did not start until 2005, with clients in the formal sector (5). Since commencement coverage has been poor and in some states available to only federal government workers (5). However, there have been complaints from some patients under NHIS over the delays in health services and sometimes lack of services and ordered investigations including imaging (X-ray) (6). A study carried out in Nigeria reported that timeliness of services at the primary health care level impacts positively upon the perception of the quality of services rendered to clients (7). This study was carried out to assess patient satisfaction with the quality of care (structure, the process of care, and overall outcome of care) at the NHIS clinic at the University of Port Harcourt Teaching Hospital (UPTH). The understanding of these factors would help in planning to improve the quality of health care services at the NHIS clinic and to enable it to fulfill the mandate of NHIS which is to improve the health status of Nigerians by the provision of financial protection and guaranteeing patients’ satisfaction (8).
Methodology
This was a descriptive cross-sectional study in which 379 participants completed a 5-point Likert scale interviewer-administered semi-structured questionnaire to rate their satisfaction level with the quality of services provided. Respondents in this study were selected via a systematic sampling technique. From the NHIS clinic records, an average of 30 adult patients are seen daily, 600 adult patients were seen monthly. The respondents were recruited for over 8 weeks. The sample interval was derived by dividing the sampling frame by the estimated sample size, that is, 1200/379, to get 3. The first sample was selected through a simple random technique in which the first 3 adult patients present in the clinic at the commencement of the study handpicked numbers from 1 to 3. The patient who picked the number “1” was the first. Therefore, every third patient that presented to the clinic via the register each day was studied. Hence, 10 patients were recruited daily for the study.
Sample size estimation was determined using the formula for estimating the minimum sample size for descriptive studies when studying proportions with the entire population size >10 000 (9). The estimated minimum sample size using overall satisfaction of 66.8% from a previous study was 341 (10). This minimum sample size was, however, increased to 379 with an assumed 10% nonresponse rate.
Study Area
This study was carried out at the NHIS clinic of UPTH, University of Port Harcourt Teaching Hospital, Rivers State. It is a 500-bed public-owned specialist tertiary health institution. Rivers state is in the South-South geopolitical zone of Nigeria.
Study Population
All adult patients aged 18 to 70 years who have accessed care in the hospital at not less than 2 different occasions at the NHIS Clinic of UPTH at the time of the study were approached for study participation. National Health Insurance Scheme patients registered with the clinic were a total beneficiary count of 13 318 made up of 5255 principal clients, 8 059 dependents, and an extra dependent of 4.
Study Instrument
The patient satisfaction questionnaire was adapted from a previous study done in Nigeria (10). It consists of 7 sections comprising of 4 to 10 items per section with a total of 37 items. Respondents in this study were asked questions on each statement and asked to assess on a 5-point Likert scale (1 = “Poor,” 2 = “Fair,” 3 = “Good,” 4 = “Very Good,” and 5 = “Excellent”). The average scores on the scales were reported. Also, the sum of the responses to the instrument’s 37 items was converted into a percentage, a score of less than and equals to 50% was regarded as not satisfied, while a score above 50% was regarded as satisfied. In this study, the reliability of the tool as determined by the level of satisfaction of care provided at the NHIS clinic questionnaire, Cronbach α coefficient was 0.95. For the scales “satisfaction on the adequacy of structures in NHIS clinic,” Cronbach α coefficient was 0.86; for “satisfaction with the medical records in the NHIS clinic,” it was 0.88; for “satisfaction with the nurses in the NHIS clinic,” we had 0.91; for “satisfaction with the doctors in the NHIS clinic,” it was 0.90; for “satisfaction with the laboratory section in the NHIS clinic,” it was 0.91; and for “satisfaction with the pharmacy in the NHIS clinic,” it was 0.91. This indicates high reliability of the study instrument. Pretesting of the questionnaire was done using 38 participants in the state-owned Braithwaite Memorial Specialist Hospital, which is an NHIS accredited center in Port Harcourt metropolis.
Data Collection and Analysis
Data collection was carried out in the waiting area of the clinic after patients received their drugs from the pharmacy, for 8 weeks from the last 2 weeks in April to the first 2 weeks in June 2018. Two research assistants (1 male, 1 female) were recruited and trained by the researcher to administer the questionnaire. To prevent double-counting, card numbers of the respondents were written against the filled questionnaire, they were asked also if they had previously filled the questionnaire.
The data were analyzed using Statistical Package for Social Sciences (SPSS) version 23. Bivariate analysis was performed using Pearson χ2. A P value of ≤ .05 was considered statistically significant.
Ethical Approval
Ethical clearance was sought and gotten from the ethics committee of the hospital. Access to the NHIS clinic and its enrollees was gotten from the NHIS project manager. Written informed consent was obtained from the respondents.
Results
A total of 379 questionnaires were administered, consistently, and completely filled, giving a response rate of 100%. Table 1 shows the sociodemographic characteristics among the respondents at the NHIS clinic, more than one-third (98, 38.3%) of them were between the ages of 41 and 50, the mean age was 45.11 ± 10.51 years. More than half (210, 55.4%) were females, while most (317, 83.6%) were married.
Socio-Demographic Characteristics of Respondents.

Table 2 shows items assessing the level of satisfaction with the availability of structure. More than half (209, 55.2%) rated the cleanliness of the NHIS clinic as being good with a mean score of 3.25 ± 0.78, 171 (45.1%) rated the completeness of equipment to deliver care as good.
Level of Satisfaction With Availability of Structures at the NHIS Clinic.

Abbreviation: NHIS, National Health Insurance Scheme.
The item with the highest level of satisfaction score (3.25 ± 0.78) was satisfaction with the cleanliness of the NHIS clinic, while the functionality of equipment and availability of drugs had the lowest satisfaction scores of 2.37 ± 0.95 and 2.08 ± 0.91, respectively.
Table 3 shows items assessing the level of satisfaction with the process of care provided at the medical record, laboratory, pharmacy, accounting, nursing, and physician sections.
Level of Satisfaction With the Process of Care at the Medical Record, Laboratory, Pharmacy, Account, Nursing, and Physician Sections by Respondents.
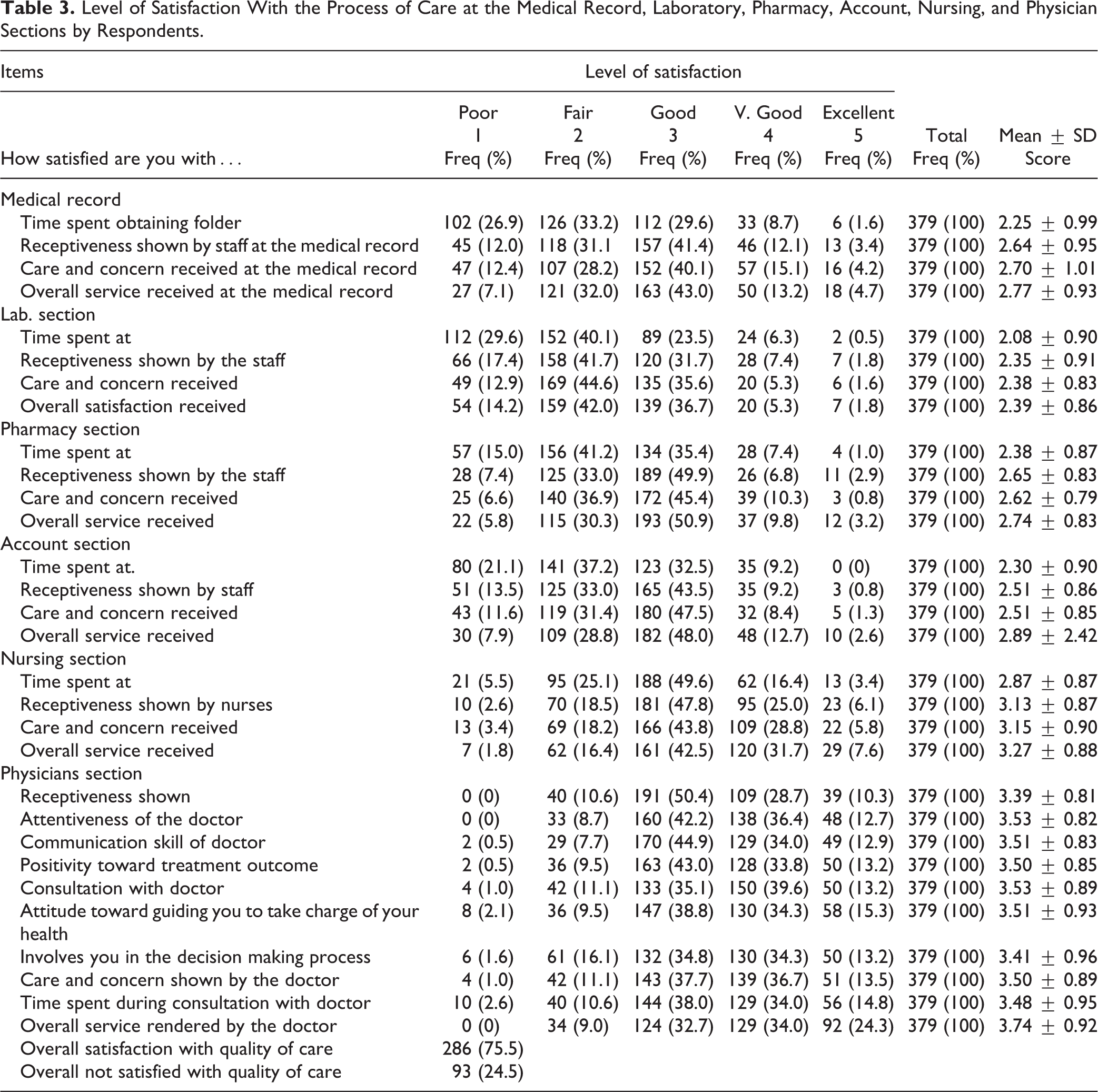
At the records unit, the item with the highest level of satisfaction score (2.70 ± 1.01) was satisfaction with the “care and concern,” and respondents 102 (26.9) were least satisfied with the time spent (2.25 ± 0.99) at the unit. At the laboratory, the highest level of satisfaction score was with the “care and concern,” received, and this was below the mean score (2.38 ± 0.83). The respondents 112 (29.6) were least satisfied with the time spent (2.08 ± 0.90) at the unit.
The item with the highest level of satisfaction score (2.65 ± 0.83) was satisfaction with the “receptiveness,” received at the pharmacy section. The respondents 57 (15.0) were least satisfied with the time spent (2.38 ± 0.87) at the unit.
The items with the highest level of satisfaction score (2.51 ± 0.85) at the account section were satisfaction with the “care and concern” and “receptiveness” shown by the staff at the account section (2.51 ± 0.86). The respondents 80 (21.1) were least satisfied with the time spent (2.30 ± 0.90) in the unit.
In the nursing section, items with the highest level of satisfaction score (3.15 ± 0.90) was satisfaction with the “care and concern’’ followed by “receptiveness” (3.13 ± 0.87). Less than half 166 (43.8) rated this as good. The respondents 21 (5.5) were least satisfied with the time spent (2.87 ± 0.87) in the unit.
The respondents were very satisfied with the level of “receptiveness (3.39 ± 0.81) then communication (3.51 ± 0.83) and attentiveness (3.53 ± 0.82)” shown by the physicians as well as time spent during a consultation (3.48 ± 0.95) and the consultation process itself (3.53 ± 0.89). The overall service rendered by the doctor had a mean score of 3.74 ± 0.92, and 129 (34.0%) rated the overall service rendered by the doctor as being very good.
Table 4 shows no statistically significant association observed between age, sex marital status, and religion with patient satisfaction with the quality of care provided at the NHIS clinic.
Relationship Between Sociodemographic, Nonmedical-Related Factors and Overall Satisfaction With Outcome of Quality of Care Provided at the NHIS Clinic.

Abbreviation: NHIS, National Health Insurance Scheme.
a Yates continuity correction.
b Fisher exact test.
c Statistically significant.
There was a statistically significant association observed between treatment outcome and patient satisfaction, as those who had positive treatment, outcomes had a significantly higher proportion 281 (98.3%) of being satisfied with the care provided at the NHIS clinic than those with negative treatment outcome 5 (1.7%).
A statistically significant association was also observed between willingness to recommend to others and patient satisfaction, as those who are willing to recommend to others had a significantly higher proportion 275 (96.2%) of being satisfied with the care provided at the NHIS clinic than those who are not willing to recommend to others 11 (3.8%).
Discussion
This study has looked at the patient satisfaction with care received using 3 domains of care namely structure, process, and outcome. This present study found the overall satisfaction score with quality of structure to be slightly above average. Responses for the item on the cleanliness of the NHIS clinic had the highest mean score under structure indicating that the respondents were satisfied with the level of cleanliness of the clinic. This is similar to a study where most patients rated the environment as clean, comfortable, and (11) suitable for them during their consultation (12). This observation in index study may be attributed to the efficient cleaning staff. However, the availability of drugs and the functionality of equipment were rated below average. This may be associated with poor maintenance of equipment culture, the protocols involved in the procurement of drugs, and other material resources by hospital management as well as delays in the release of funds as well as poor funding.
This study also assessed satisfaction at various levels of the process of care; the satisfaction with the doctor consultation had the highest level of patient satisfaction, while the lowest level of patient satisfaction was found in the laboratory section. The high satisfaction with a consultation with the doctor was attributed to being an advantage to the patient. The patients preferred to spend more time with the doctors for a closer relationship and perceived feeling of special care from the doctors, while the process of sample collection in the lab which involves a needle prick may influence the patient’s satisfaction with care. There was a general complaint about the waiting time in most of the sections, showing clearly a need for the staff to improve on the time spent on the process of care. The report in this study is in agreement with a study done in south western Nigeria which identified waiting time, how patients were treated by the health care service providers as key determinants of satisfaction (13).
On the contrary to this present study, another study done in northern Nigeria among NHIS enrollees reported that most respondents were satisfied with the services offered by the medical records, pharmacy, laboratory, and accounts units of the clinic. Only a few respondents were dissatisfied or indifferent at all the service units (14). Also, studies have reported a long consultation waiting time due to a shortage of physicians. However, a majority of respondents felt that the consultation time was adequate to discuss their problems and needs (14, 15). In agreement with findings in this study, Iloh et al in a tertiary hospital in south eastern Nigeria reported that the respondents were most satisfied with the patient–provider relationship. Their study reported medical doctors’ relationship was rated highest and medical records staff was rated lowest (10).
This present study found high levels of overall satisfaction with the quality of care provided at the NHIS clinic in UPTH. This high level can be associated with the fact that the NHIS clinic which also serves as the staff clinic is within a tertiary hospital making it easy for clients to assess the tertiary level of care when needed. This value is high compared to some other studies in Nigeria, which reported a lower overall satisfaction score (10,14,16,17). On the contrary, the overall satisfaction level in this present study was lower compared to findings from South Africa and Islamabad where overall higher satisfaction scores were reported (12,18). These differences specifically the findings from the South Africa study can be linked to its collaboration with international partners which resulted in better funding, hence the higher level of overall satisfaction, unlike this present study where most of the funding comes from the national government.
Our study however found that positive treatment outcome; willingness to recommend to others among patients was statistically significant with satisfaction with the quality of care. The duration of enrolment was found not to be statistically significantly associated with patient satisfaction in this study. This is in contrast to findings from studies in southwest Nigeria which reported that respondents who had enrolled for between 1 and 4 years were about less than half as likely to be satisfied than respondents who had enrolled for 5 years (19,20). However, while our study did not demonstrate any relationship between sociodemographic variables (such as age, education, marital status, and religion), and satisfaction with the quality of care, some studies have reported age as the strongest predictor of satisfaction (16), while others have reported no association between patient satisfaction and sociodemographic variables (17,19).
Study Limitations
Satisfaction was based entirely on respondents’ perceived expectations which may not have given the true description of the services provided at the clinic. The information for satisfaction was also collected as a snapshot, happenings around the time of collection of information could affect the respondents’ assessment.
Conclusion
Patients’ satisfaction is an important outcome that reflects the quality of health care provided in a health facility. This study reported the patient’s satisfaction with the different domains of care at the NHIS clinic UPTH and the associated factors. Despite the higher percentage of the overall satisfaction with the outcome of quality of care among patients in this study, most participants were dissatisfied with the laboratory service provided at the NHIS clinic, and they complained about time spent in the laboratory, account section, and obtaining folders at the medical record and at the pharmacy. However, they expressed great satisfaction with the provider–patient relationship with the physicians. There were complaints about the availability of drugs as well as malfunctioning equipment. The study, however, found that positive treatment outcomes, willingness to recommend the clinic to others, were related to patients’ satisfaction with care. It is recommended that the NHIS staff should undergo time management training periodically to achieve the mandate of the program, and there should be a review of the equipment availability and maintenance system as well as the drug list and procurement system.
Footnotes
Authors’ Note
Ethical clearance was sought and gotten from the University of Port Harcourt Research and Ethics Committee. Permission to carry out the study was obtained from the Head of Department of Preventive and Social Medicine, University of Port Harcourt. Access to the NHIS clinic and its enrolees was gotten from the NHIS project manager. A written informed consent was obtained from the respondents.
Acknowledgments
All the respondents and data collectors are appreciated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.