
Abstract
Primary sarcoma of the lung and/or pleural cavity is a rare finding accounting for <0.5% of all thoracic malignancies. Histologically, mesothelioma predominates in this subcategory of neoplasms; its relationship to asbestos exposure and cigarette smoking is well documented. Other tumor types include fibrosarcoma, malignant fibrous histiocytoma, angiosarcoma, leiomyosarcoma, synovial sarcoma, and Ewing sarcoma. Standard evaluation with bronchoscopy and radiographically guided biopsy are frequently nondiagnostic and require open biopsy to provide an adequate tissue sample.
Keywords
Case Study
A 39-year-old man employed as a housepainter presented with fevers, weight loss, and a nonproductive cough. He reported having a positive tuberculin skin test and received Bacillus Calmette-Guérin vaccine as a youth. Current sputum cultures and cytology were negative for malignancy. Computed tomography of the chest showed a large right pleural effusion and 3 pleural-based nodules (Figure 1). Bronchoscopy demonstrated no endobronchial lesions and a negative aspirate cytology. Thoracentesis and pleural biopsy yielded only pleural fibrosis.

Computed tomography of the chest illustrating a large, irregular, pleural-based mass.
Thoracoscopic exploration of the chest revealed a longitudinally spreading, thick, friable tumor mass along the parietal pleural surface of the lung. Light microscopy showed a high-grade spindle cell neoplasm (Figure 2; hematoxylin and eosin stain at ×40). Further investigation demonstrated a tumor that was vimentin (+), cytokeratin (−), and epithelial membrane antigen (−), thus suggestive of a sarcoma, but with calretinin (+). Electron microscopic studies failed to show the long, thin microvilli characteristic of mesothelioma. Chromosomal studies with the reverse transcription-polymerase chain reaction test for the t(X;18) translocation confirmed the diagnosis of a synovial sarcoma. 1 Further workup revealed no evidence of extrathoracic disease. Given the presence of multiple nodules and extensive pleural tumor involvement, no further surgery was planned and the patient treated with adriamycin and ifosfamide. He is alive with disease at 10 months postdiagnosis and has asymptomatic progression of his tumor as seen on computed tomography scan.
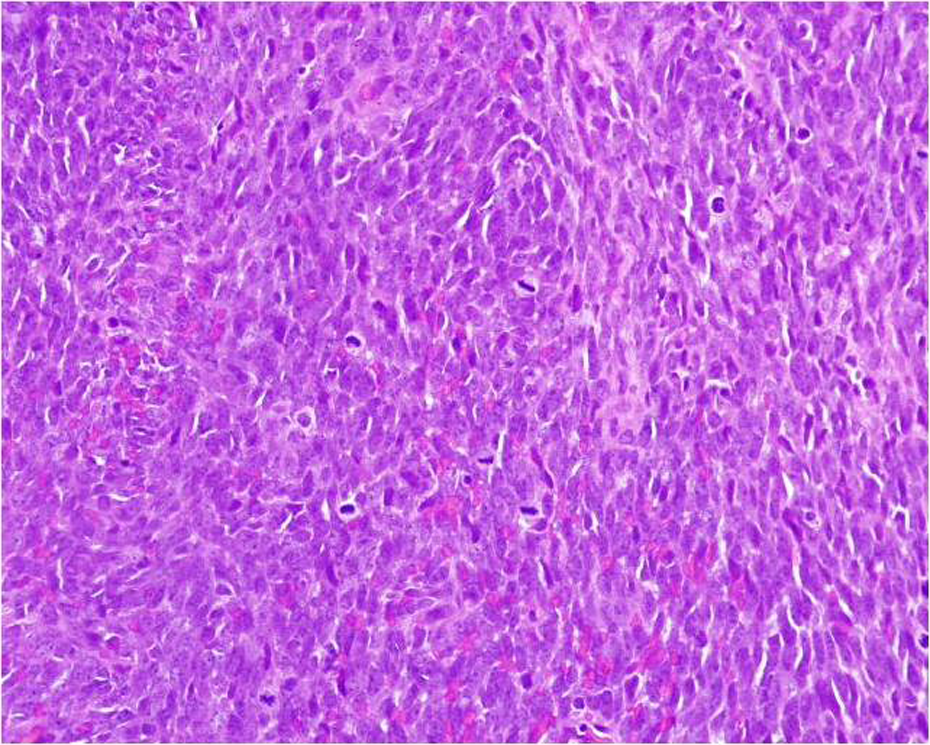
Hematoxylin and eosin stain of the tumor at ×40 magnification demonstrating a spindle cell malignancy.
Discussion
A paucity of literature exists on primary pulmonary synovial sarcoma. Most cases of intrathoracic synovial sarcoma are secondary to metastatic disease with a clinically obvious primary tumor adjacent to the joint capsule in a limb. As noted by Nascimento et al, 2 metastatic disease from these cancers generally results in multiple, rather than isolated, pleural nodules.
In contrast to a series of patients reported by Gaertner et al, 3 this patient’s tumor appeared to be monophasic with a relatively small epithelial contribution to the tumor cell population. All tumors in the series were pleural-based masses that were excised at surgical exploration. The median survival of the 5 study patients was 18 months, with 4 of the 5 patients dead of their disease by 30 months. Histological analysis of recurrent tumors showed a monophasic spindle cell pattern.
In the study of primary intrathoracic sarcomas by Régnard and colleagues, 4 an actuarial survival of 48% at 5 years was noted if the primary tumor could be resected completely, and a 0% survival at 2 years if only incomplete resection was achieved. Further, they found a significant prognostic difference between T2 and T3 tumors, with a lesser contribution of nodal status to overall survival.
The absence of an extrathoracic disease in this case supports the notion by Rys et al 5 that primary synovial sarcomas are derived from immature mesenchymal elements and not from the synovium within the joint capsule. Differential subpopulations’ cell growth probably plays an integral role in determining tumor recurrence and ultimately patient survival.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.