
Abstract
The COVID-19 pandemic highlighted critical communication challenges within the public health workforce, emphasizing the urgent need for practical, scalable, and accessible training solutions. In response, an academic health communication center developed a Health Communication Training Series (HCTS) featuring asynchronous, online courses designed to strengthen communication skills among public health professionals. This paper presents an evaluation of three free, online courses delivered through a state-funded partnership aimed at bolstering workforce resiliency. A survey of 780 registered learners resulted in 70 completed responses, with participants representing various sectors including public health, higher education, and healthcare. Learners reported meaningful application of course objectives within their professional roles and shared course materials with peers. Feedback emphasized the uniqueness of the courses, citing format, content relevance, instructor expertise, and an engaging design. Participants valued the self-paced structure, timeliness of topics, and real-world applicability. Findings suggest that asynchronous mini-courses are a feasible strategy to meet the dynamic needs of a strained public health workforce, providing timely and relevant skill development in an accessible format. The results also point to the potential of such courses to facilitate professional reflection and peer dialogue. Despite limitations related to response bias and generalizability, the study supports continued investment in flexible, high-quality online education to support ongoing professional development and workforce sustainability in public health.
Introduction
The immediate impact of COVID-19 on training and education for public health professionals cannot be overstated. The pandemic underscored the value of effectively deploying health communication skills in the public health workforce (Dubé et al., 2022). It also exposed public health challenges on a global scale, including substantial challenges surrounding communication. The COVID-19 pandemic highlighted the general public’s massive misunderstanding of basic science leading to the increased spread of conflicting health information, resulting in an overall distrust in health professionals and scientific experts (Mandelbaum, 2021). Mitigating the spread of emerging health threats while managing the concerns and expectations of the general public regarding health is an essential job function of all public health professionals.
During the response to the COVID-19 pandemic, the communication between multi-level health agencies, as well as communication with the public, revealed large communication training gaps in the existing information flow leading to job dissatisfaction and burnout among the public health workforce (Kenney et al., 2020; Leider et al., 2023; Mandelbaum, 2021). Essential communication functions such as relationship building, dissemination of data analysis, and explaining complicated health information are crucial in community preparedness and pandemic response (Donovan et al., 2017; Kenney et al., 2020). Kenney et al. (2020) explain that while many health recommendations trickle down from the federal level, it is the local health departments who are essential to promote and implement these recommendations.
Public health professionals’ experience in response to the pandemic emphasizes the value of health communication. Furthermore, when health information is communicated effectively, studies demonstrate that the public is more likely to engage in the recommended preventive behaviors (Donovan et al., 2017). Improving communication skills among public health professionals is essential to the mission of their work, as previous studies have also found that communicating simple health behavior messages such as practicing social distancing and wearing face masks during the pandemic helped limit disease spread and ultimately reduce the number of hospitalizations by up to 75% in the U.S. population (Mandelbaum, 2021). Researchers have identified opportunities to implement innovative and engaging pedagogical approaches to health communication training for public health professionals including mini-courses offering micro-credentialing (Kemper Seeley et al., 2025). The urgency to meet public health professionals where they are is especially critical, evident by the mass exodus of public health workers from the field citing work overload and burnout as top reasons (Leider et al., 2023). When it comes to education and training opportunities, modality matters. Flexibility and concise delivery methods and design are crucial to keep an already stretched workforce engaged even with content that is relevant and timely.
Encouragingly, the World Federation of Public Health Associations convened a working group to address the concerns of low-quality training and education for public health professionals (Kemper Seeley et al., 2025). Acknowledging the lack of high-quality training opportunities for public health professionals strengthens the call for an interdisciplinary approach to teaching health communication. There is significant value in bringing together communication scholars as well as experienced working professionals to improve communication competence by presenting content that is both theoretically grounded, yet also evidence-based (Donovan et al., 2021). The unique perspectives of frontline public health professionals present a case-based approach that allows working professionals along with up-and-coming scholars in the field to learn from the experiences of seasoned public health professionals (Henderson & Sendall, 2022; Kemper Seeley et al., 2025). Additionally, due to geographic limitations, much of the global workforce remains without access to critical training and education calling for the need of innovative training modalities aimed at overcoming physical barriers such as asynchronous online courses (Kemper Seeley et al., 2025).
The current paper focuses on the evaluation of an online, scalable, asynchronous health communication training program. The goal of this paper is to evaluate the effectiveness of an online/asynchronous delivery method and relevance of content for three courses: “Pandemic Preparedness Communication,” “Dealing with Conflicting Health Information,” and “Strategies to Support Team Well-Being.” Each course educates learners on a relevant topic, and collectively, these courses equip learners to become a more prepared and resilient workforce. The online training series evaluated in the current paper is part of a larger Health Communication Training Series designed for a variety of learners, from students to practitioners, bridging health communication theory and practice (Mackert et al., 2024). The content is intended to be accessible by implementing pedagogical strategies that present core communication principles in an easily digestible and visually appealing format (Donovan et al., 2021).
Methods
A university-based health communication center developed the Health Communication Training Series (HCTS) in 2020 with the intent to design content tailored to public health practitioners and clinicians (Mackert et al., 2024). The Health Communication Training Series became a solution for a gap in health communication training identified by public health professionals who attended an annual 3-day Health Communication Leadership Institute, who asked for additional ways to continue their learning (Mackert et al., 2024). The program has evolved to include collaboration between external partnerships and the Center for Health Communication resulting in 15 online courses with more than 4,600 course enrollments and over 3,700 unique users. One specific collaboration has led to the development of a bundle series of courses intended to support communication efforts by sharing best practices and practical tools to improve the capabilities of public health professionals that are part of the workforce resiliency program in a Southwestern state.
The course development begins with the collaboration with the external partner to identify specific course topics. The course topics are also informed by responses to post-course surveys from learners who completed other HCTS online courses. After identifying desired topics from post-course surveys and a discussion between the external partners and the team, an instructor is recruited based on expertise and availability. Previous instructors include researchers, academic faculty, and clinicians. Course objectives and content are outlined and reviewed through multiple rounds of collaborative efforts between course instructor, Center for Health Communication online education program staff, and the external partner. Once course content is finalized, filming takes place on campus in the production studio and progresses to post-production, where the course is finalized and published on the Canvas online learning platform.
The current research evaluates a bundle of online courses developed through a partnership between the Center for Health Communication and a state-funded organization created to help strengthen outbreak readiness and promote the response infrastructure of local health departments in a Southwestern state.
An online course evaluation survey ran between November 25 – December 10, 2024. The University’s policies for program development and evaluation designate this study as exempt from requiring IRB approval. The survey comprised five total sections: initial items collected information on how participants heard about HCTS, items to understand the importance of continued education (CE) credits, and learn about what training topics were difficult to find (6 items), Strategies to Support Team Well-Being course-specific items (13 items), Dealing with Conflicting Health Information course-specific items (10 items), Pandemic Preparedness Communication course-specific items (10 items). The final survey section collected additional demographic data such as age, gender, race/ethnicity, education, residence, location where they serve in their work, language, industry, etc. (19 items). All participants were asked demographic questions, then the course-specific survey sections were assigned to each participant based on which course(s) they each completed. Finally, participants were asked closing demographic questions and were informed of compensation details. There were seven items within each course-specific survey section that were consistent across all course survey sections assessing their attitudes toward the course content and actions participants took to discuss or share the course content with others. Survey logic design was employed to display the course-specific items in the following prioritized order: Strategies to Support Team Well-Being, Dealing with Conflicting Health Information, and Pandemic Preparedness Communication. The average time to complete the survey was approximately 7 min.
The survey was distributed directly to 780 participants who have previously registered for at least one of the three courses (Pandemic Preparedness Communication (n = 516), Dealing with Conflicting Health Information (n = 157), Strategies to Support Team Well-Being (n = 67) via Mailchimp. The first 50 eligible participants were given a $20 Amazon e-gift card incentive. The remaining participants were then entered into a drawing for a $20 Amazon e-gift card.
Findings
After the survey data were exported from Qualtrics and cleaned, removing partially completed submissions, there were 70 total participants who completed at least 97% of the survey (response rate: 8.9%). The participants predominantly self-identified as women (72.9%) followed by men (22.9%) and the majority of the participants were between 30 and 39 years of age (28.6%) followed by 18 to 29 years (22.9%) and 40 to 49 years (18.6%). Participants mainly came from a public health background (42.9%) followed by higher education (20%) and healthcare (18.6%). Most of the respondents completed the Pandemic Preparedness Communication course (n = 49), followed by Dealing with Conflicting Health Information (n = 39), and Strategies to Support Team Well-Being (n = 22). According to course metrics, the average time between participant course completion and the course evaluation survey completion was 12.8 months (SD = 6.93) for the Pandemic Preparedness Communication course, 5.17 months (SD = 2.08) for the Dealing with Conflicting Health Information course, and 3 months (SD = 1.41) for the Strategies to Support Team Well-Being course.
Participants were asked to agree or disagree on a seven-point Likert scale (1-strongly disagree[. . .]7-strongly agree) “I have applied the strategies learned in this course in my professional role.” On average respondents reported that they agree that they applied the strategies learned in the courses to their professional role (M = 5.84, SD = 1.35).
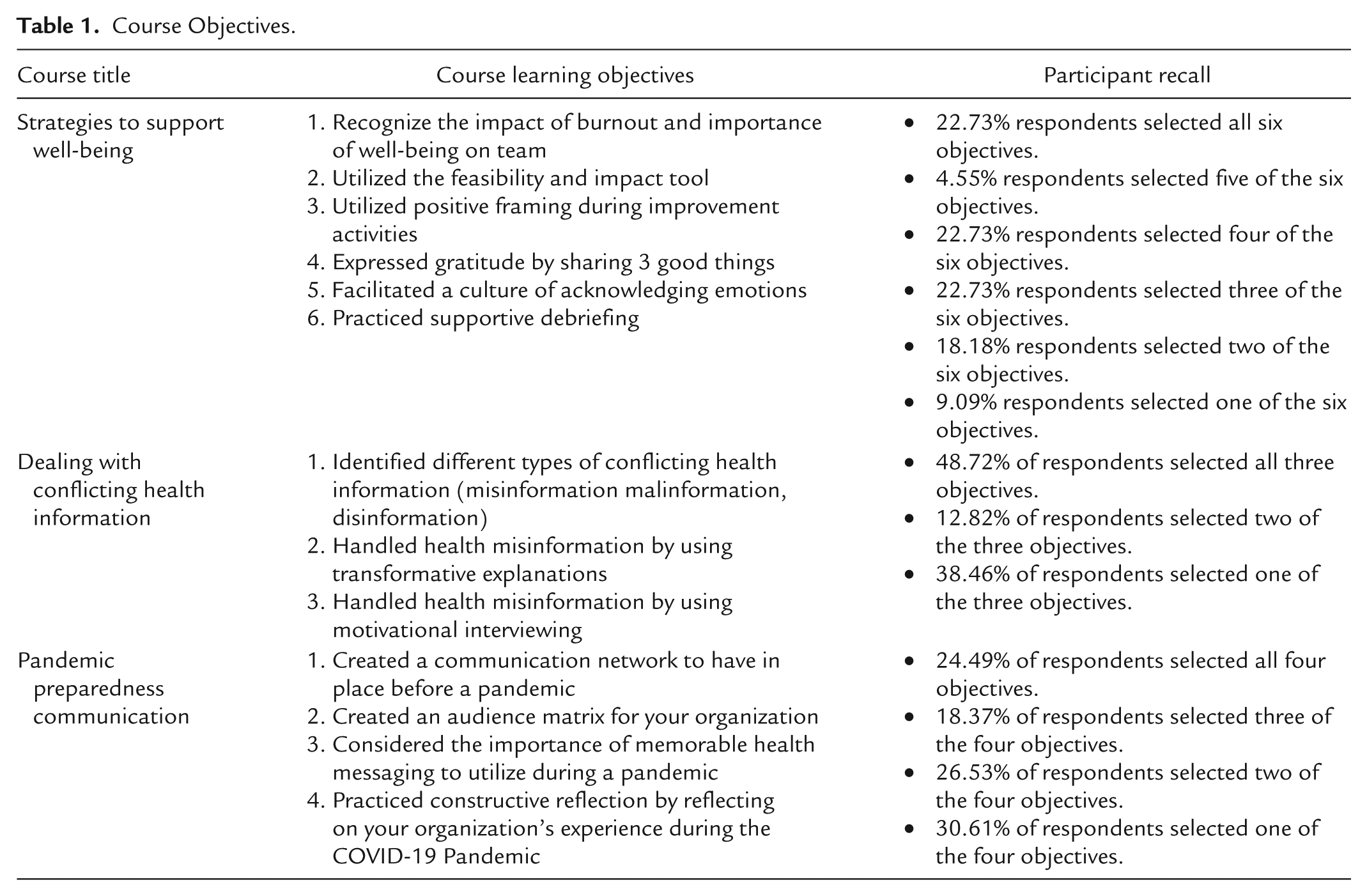
Regarding the course objectives, respondents reported applying many of the intended course objectives in their work. The participants who completed the Dealing with Conflicting Health Information applied the majority of the intended course objectives in their work. The other two courses, Pandemic Preparedness Communication and Strategies to Support Well-Being were closely split. See Table 1.
Course Objectives.
Participants were asked to agree or disagree on a seven-point Likert scale (1-strongly disagree. . .7-strongly agree) to the statement, “I talked to people at work about this course.” On average, respondents stated that they agreed that they talked to people at work about the course (M = 5.58, SD = 1.63).
When asked if participants shared the course with others who found it helpful, the majority of respondents stated that they shared the course. For the Pandemic Preparedness Communication course, 43 of the 49 participants (87.8%) stated they shared the course. For the Dealing with Conflicting Information course, 30 of the 39 participants (76.9%) stated they shared the course. For the Strategies to Support Well-Being, 19 of the 22 (86.4%) stated they shared the course. Of those who answered “yes” to sharing the course with others who found it helpful, 88% (81 out of 92 participants) specifically shared the course with a colleague at work.
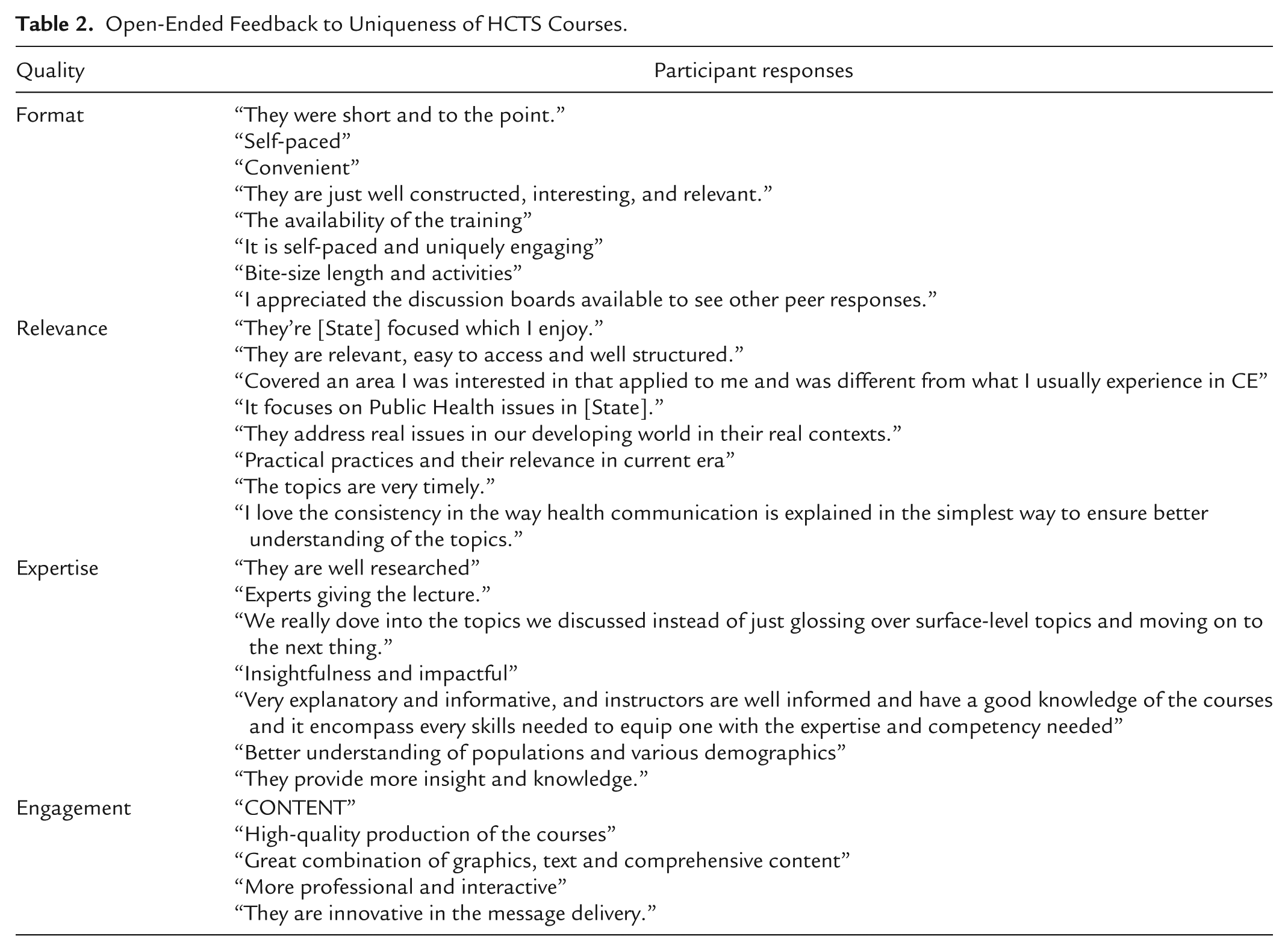
We analyzed responses to the single open-ended question “What made the HCTS courses unique from other CE efforts you have previously taken” using Braun and Clarke’s thematic analysis approach (2006). Two team members independently reviewed all responses to agree on themes and sentiment. The resulting themes were reviewed with the larger research team and sample quotes for each are displayed in Table 2. There was a total of 62 responses from participants which were thematically analyzed resulting in four common themes. Most of the open-ended responses were positive (69.4%) with 27.4% being neutral and only 3.2% categorized as negative. The negative responses expressed the courses were either slower paced or “not necessarily unique” but rather “a good opportunity for free CE credit.”
Open-Ended Feedback to Uniqueness of HCTS Courses.
Discussion
The experiences during the COVID-19 pandemic highlight the need for continued communication skills development for the public health workforce. This is particularly true as they confront challenges such as skepticism of public health research and expertise and the spread of conflicting information online. The purpose of this paper was to evaluate three scalable, asynchronous health communication courses through an online survey of registered learners who completed the courses.
The findings of this evaluation support previous research demonstrating the need to meet public health professionals where they are, to address some of the drivers that lead to increased burnout - in this case related to communication training and the flow of information during the COVID-19 pandemic (Leider et al., 2023). Learners reported applying at least half of the course learning objectives in one course and nearly even split applications in the other two courses. Participants reported favorable feedback regarding the format, topic relevance, and level of expertise in their open-ended responses speaking to the uniqueness of the courses from other CE efforts. Overall, learners found the material engaging and beneficial as reported in their own words. These key findings point to a successful and innovative approach in presenting critical public health training. The success of these three free online courses is a response to the urgent need to offer critical training to both emerging and seasoned public health professionals through an asynchronous format that is both effective and flexible (Kemper Seeley et al., 2025).
There are many opportunities afforded by well-designed asynchronous online education. The process of designing, developing, and promoting asynchronous online education can be replicated across disciplines while continuing to present high quality content that meets the stringent requirements of CE accreditation. The course modality presented in this study provides a learning space where skills can be newly developed or refined while encouraging adequate time for learners to reflect on its importance. New courses can be quickly developed and disseminated to address emerging trends in a variety of fields. For example, in public health—as with the emergence of AI as a tool in public health research and practice - to provide timely learning opportunities for professionals. A challenge related to developing such courses, however, is ensuring the content is more “evergreen” and can remain useful over time; in the case of a course on the role of AI in public health, for example, that would require education on how such tools work and the ethical application of such tools - and not training focused on a specific tool at a particular moment in time.
Another opportunity in such courses is to embed content and exercises designed to encourage learners to discuss and apply course content with their colleagues and organizations; an example might be a worksheet designed to guide a conversation about key audiences for future pandemic communication planning. Such efforts could help the information in these kinds of courses spread beyond those learners directly enrolled in the classes, but more research would be needed to study the efficacy of these approaches. The workforce remains stretched thin across many industries and regardless of daily responsibilities, there is a need for continued development. Online asynchronous courses such as the ones presented in this paper offer convenience and accessibility for learners with busy schedules with only fragments of time for learning.
This study has limitations, most notably that the sample might include learners who were more likely to have approved of the course content and approach and potentially already be engaging in some of the outlined objectives of each course. Still, study results suggest there is a substantial opportunity for well-designed asynchronous online education to support the ongoing professional development and skills-based training of practicing public health professionals. As such, approaches such as that shared in this report should be considered when thinking about how to ensure the ongoing training and preparation of the public health workforce. Additionally, the survey item asking participants to report the number of learning objectives they have applied to their work did not allow for the selection of “zero objectives” or “none” which should be acknowledged as a limitation in the study design as some participants who reported only applying one objective could include individuals who did not apply any. Despite this limitation, the participants who selected multiple objectives remains a valuable indicator of the applicability of the course content. Finally, the survey used did not collect individual course completion data. Therefore, additional analysis could not be conducted to determine potential differences in evaluation outcomes based on time lapses between course completion and course evaluation. Future course evaluation studies can overcome this limitation by embedding the course evaluation survey in the course platform with an automatic evaluation survey deployment set to a cadence such as 6 and/or 12 months from course completion.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Texas Epidemic Public Health Institute (TEPHI).