
Abstract
Young people transitioning from out-of-home care (OOHC), often called care leavers, are known to experience mental health challenges. This article presents a scoping review of research studies completed on the mental health care needs and outcomes of care leavers in Australia from 2015 to 2021. Incorporating 17 studies consisting of six peer-reviewed papers and 11 grey literature reports, the review identified several common concerns pertaining to high levels of poor mental health and psychosocial complexity. These concerns were attributed to a number of factors including placement instability, inadequate access to specialist mental health support services, and limited workforce skills and training. Some sub-groups of care leavers such as young parents, those leaving residential care, Aboriginal and Torres Strait Islander care leavers, and an older cohort who had experience of institutional OOHC in earlier decades, were noted to be at particular risk. Nevertheless, some strategies for improving policy and practice were highlighted including more concrete transition planning that established links with support services prior to leaving care, an extension of OOHC till at least 21 years of age, provision of further supports such as trauma-informed approaches targeted towards the specific needs of this vulnerable population and culturally responsive programs for Indigenous youth. A limitation of the review was that most studies included were completed before the introduction of extended OOHC in all Australian jurisdictions, and hence do not reflect the positive influence of extended care on transition pathways including mental health. Future research should specifically examine the impact of extended care models on mental health care needs and outcomes.
Introduction
Young people transitioning from out-of-home care (OOHC), often called care leavers, are recognised globally as a vulnerable group due to their often traumatic experiences prior to entering care, the varied quality and stability of care placements offered and the accelerated transition to independent adulthood that many encounter irrespective of their developmental needs and capacity (OECD, 2022). As a result, they may experience life-long inequalities and disadvantages compared to their non-care peers (Sacker et al., 2021).
One specific challenge for care leavers pertains to advancing their mental health and well-being. In this article, we present a scoping review of research studies completed on the mental health care needs and outcomes of care leavers in Australia from 2015 to 2021. Our analysis examines key impacting factors, the specific experiences of more vulnerable sub-cohorts of care leavers and potential strategies for policy and practice reform.
Formalised OOHC arrangements in foster, kinship and residential care exist for children and young people in Australia who are unable to live with a parent. The Australian Institute of Health and Welfare (AIHW, 2022) reported around 46,200 children (defined as dependents under the age of 18 years) were in OOHC in Australia on 30 June 2021. The vast majority (92%) were either in relative/kinship care or foster care. Approximately 6% lived in residential care group homes supervised by rostered staff. Residential care in Australia is often used to accommodate children whose age (older teens) or challenging behaviour makes it difficult to place them in foster or kinship care. They have often experienced more traumatic early childhoods or greater placement instability than other children in OOHC (Ainsworth & Hansen, 2015; Moore et al., 2017).
Stays in OOHC can be brief, extended or permanent arrangements. However, in 2021, approximately 31,400 young people had been in OOHC for 2 years or more, and most (82%) were in care continuously for the preceding 12 months or longer (AIHW, 2022). Of the overall OOHC population, 19,500 were identified as Aboriginal and Torres Strait Islander (hereafter Indigenous), a rate of 58 per 1,000 Indigenous children in Australia and more than 11 times the rate for non-Indigenous children. This demonstrates an overrepresentation of Indigenous children in OOHC in Australia.
The Transition from Out-of-Home Experience
Australia has a federal child protection system. This results in varied transition from care legislation, policy and services across the eight jurisdictions (Australian Capital Territory (ACT), Northern Territory, Queensland, South Australia, Tasmania, Western Australia (WA), New South Wales (NSW) and Victoria). Approximately, 3,900 young people nationally aged 15–17 years transition from OOHC each year. A total of 1,265, or around 35%, are estimated to be Indigenous (AIHW, 2022). The Commissioner for Children and Young People Victoria suggests the proportion of youth transitioning from residential care constitute about 22% of care leavers (CCYPV, 2020), which is far higher than their overall proportion in OOHC.
In 2021, the national (Commonwealth) Government released an updated National Framework for Protecting Australia’s Children, which recommended nationally consistent leaving care policies and practices, including an expectation that all young people in care will have an operational leaving care plan at the age of 15 years, and that care leavers be supported till at least 21 years of age. However, in practice, the Commonwealth has neither imposed nor resourced these standards, and no minimum benchmarks have been established across the states and territories (Mendes, 2022).
Consequently, the targeted age and level of support available to care leavers within Australia varies considerably. Until recently, all the jurisdictions shared a common position of offering only discretionary (and mostly poorly resourced and inadequate) assistance rather than mandatory unit cost funding once the young person turned 18 years. This meant all care leavers were expected to abruptly transition from reliance on state care to so-called independent adulthood at no later than their 18th birthday, irrespective of their diverse skills, preparedness and capacity (Baidawi, 2016).
In response to the effective Anglicare Victoria Home Stretch advocacy campaign to extend care across Australia, all jurisdictions recently committed to introducing various forms of extended care to 21 years for some or all care leavers. Victoria and WA are currently the only jurisdictions to have introduced universal extended care available to those leaving residential as well as foster and kinship care (Mendes et al., 2022). The potential positive impact of these extended care programs on care leaver outcomes including mental health have been widely recognised internationally (OECD, 2022). However, the studies reviewed in this article were completed prior to these programs being introduced in Australia.
The use of the binary terms ‘dependent’ and ‘independent’ are increasingly viewed as problematic in leaving care literature. This article rejects any notion that youth leaving care at 18 years or earlier, with varied developmental skills and needs, will suddenly mature from dependent children to independent adults who no longer require support from OOHC carers, workers and services. Rather, we favour the term ‘interdependence’ to signify a notion of shared care and responsibility, recognising care leavers and other young people in the community will continue to draw on relational connections with family members, friends, support workers and the broader community well into their twenties (Atwool, 2020; Storo, 2018).
Risk Factors for Mental Health, Childhood Adversity and Experiences Prior To Care
Adverse childhood experiences such as exposure to abuse or neglect from a parent or care giver, exposure to family violence, familial substance use and/or mental illness, parental separation/divorce and parental incarceration have been identified as risk factors for future mental illness (World Health Organization, 2018). These factors can lead to placement in OOHC, where children and youth may be exposed to placement instability, varied quality of supports and experiences of further abuse by carers or other adults. Conversely, research has identified factors that can be protective against future mental ill-health, such as family, community and social support (Rapee et al., 2019), yet these are resources the OOHC population often have limited access to. In the general population, of those who develop a mental disorder in their lifetime, around 50% do so by mid-teens and around 75% by their mid-20s (Kessler et al., 2007). Given current OOHC age-based policy, those with experience of OOHC may either be leaving or have only recently left care when symptoms of mental illness first begin to appear.
The Missing Middle in Mental Health
Across Australia there are a variety of free and fee-for-service programs for treatment and support of mental health conditions, such as local community health centres or the federal youth service, Orygen. Orygen operate headspace centres which act as a one-stop shop for young people who need help with mental health, physical health (including sexual health), alcohol and other drugs or work and study support. However, some people (generally referred to as ‘the missing middle’) experience symptoms and psychosocial complexity that are not effectively managed through established care pathways, yet they cannot access or are ineligible for more intensive services (Commonwealth of Australia, 2021). Orygen note that ‘forty per cent of headspace clients do not improve in clinical symptoms’ (n.d. p. 2). Such limited changes in symptomology may indicate these clients would benefit from more targeted services.
The barriers to appropriate service linkage are complex. For example, the ACT Department of Health cite affordability and waiting lists alongside ‘a range of intersecting system constraints and challenges related to workforce, funding arrangements, service transitions and coordinated support’ (2022, p. 30). There are differences in eligibility criteria and service offering between child and adult services, meaning those aged 16 years and above who transition from publicly funded youth programs may not be able to access equivalent adult services. For those in OOHC, there are specific barriers such as authorisation and consent processes, knowing past or family medical history, accessing timely appointments and paying for services (McLean et al., 2022). Yet there are limited funded programs that specifically target the most vulnerable groups, such as those in the child protection system (Department of Health Australia, 2021).
COVID
The National Study of Mental Health and Wellbeing 2020–21 collected data during the early stages of the COVID-19 pandemic. It found that almost two in five (39.6%) Australians aged 16–24 years had experienced a psychological disorder and continued to demonstrate symptoms in the 12 months prior to the survey (Australian Bureau of Statistics, 2022). Additionally, one in five (20%) of people aged 16–34 years were experiencing high or very high levels of psychological distress.
Evidence from a number of countries indicated that COVID-19 accentuated the risk of care leavers becoming homeless, unable to afford food, losing access to education or employment, or experiencing deterioration in mental health. In particular, social distancing regulations exacerbated exposure to social isolation and loneliness (Collins and Augsberger, 2020; Kelly et al., 2021; Munro et al., 2022). While research is still emerging, the OOHC cohort are likely to have additional stressors and risk factors, alongside fewer protective factors, which could make any impacts more acute and even increase their vulnerability to distress and psychological disorders (Devaney et al., 2023).
Aim
This project employed a scoping study to map existing research and examine the mental health care needs and outcomes for Australian youth transitioning from OOHC, whether from foster, kinship or residential care. The review sought to identify recommendations for best practice policies and programs, and any specific impacts for vulnerable subsets of the OOHC population such as early parenting care leavers, care leavers involved with alcohol and drug (AoD) services or youth justice, those who transitioned from residential care, and the large Indigenous cohort.
The research was guided by the question ‘What can scholarly and grey literature tell us about the mental health needs and outcomes of young people transitioning from OOHC in Australia?’
Subsidiary questions were:
Are there differences in mental health needs and outcomes for youth transitioning from OOHC according to placement type, such as residential care as opposed to foster or kinship care?
and
What are the strengths and limitations of support services (child welfare, leaving care or youth or adult mental health specific) in relation to meeting the needs of this vulnerable population?
Methods
Structured search terms were used to identify Australian grey and scholarly publications that focussed on the mental health needs of care leavers from 2015 to 2021. Data sources were accessed in mid-2022 and included ProQuest, informit, SpingerLink and Taylor & Francis Online. The search used 11 terms for different types of OOHC, combined with phrases related to mental health. They were: mental health care leavers; mental health leaving care; psychiatric care leavers out of home care; mental health needs of care leavers; mental health leaving foster care; mental health leaving kinship care; mental health leaving residential care; mental health leaving state care; mental illness care leavers; mental illness leaving care and mental illness leaving state care.
Not all papers included were peer reviewed, but all presented a clear research design and methodology. Papers citing both primary and secondary data were included. Key components were collated, such as methodology, population or sample, location of study and key findings. Initial analysis of the content of each paper was completed by one researcher, then reviewed by a second researcher to extract key findings, outcomes and any recommendations assessed as highly relevant to care leaver mental health.
Types of Publications and Locations
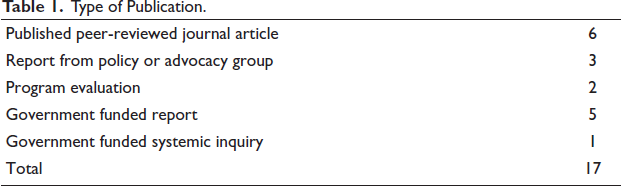
In total, 17 articles met the research criteria, this included six papers published in peer-reviewed journals and 11 forms of grey literature. Three grey literature publications were reports by policy or advocacy groups, two were program evaluations and six were government-funded reports (this included one systemic inquiry). See Table 1 for summary.
Type of Publication.
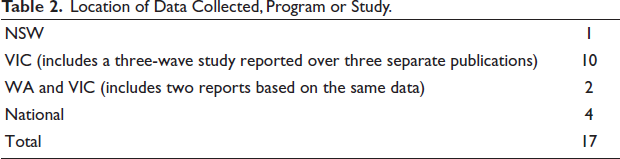
Four publications examined national samples or collected data Australia wide, one in NSW only and 10 studies were localised to Victoria. Two papers used the same data set collected from WA and Victoria, but given each appeared to examine different aspects of the data both were included. Three of the reports from Victoria were part of a longer research study reported in three waves, which used a population of existing respondents and new recruits over the term of the study, revising the questions in each stage. Each appeared to examine different aspects of the data thus were included in the sample. See Table 2 for summary.
Location of Data Collected, Program or Study.
Methodology
The sample used qualitative and quantitative models, and some involved mixed methods or a randomised control trial. Data collection methods included surveys, focus groups and interviews with people who had experienced OOHC, service providers, workers from the OOHC sector, researchers, lived experience experts, other stakeholders and consultations with paid and unpaid carers.
Populations
Despite the Indigenous population being overrepresented in OOHC overall, most studies did not appear to have recruited a representative Indigenous sample. People often had multiple episodes of care across different placements, and some articles did not identify care type, whilst others documented the most recent type prior to leaving care, or multiple types of care for each participant. Some studies included mental health prevalence data gathered from evidence-based assessments and questionaries, from self-report, or they identified formal diagnosis of mental illness or psychiatric disability through data matching.
Results
Prevalence of Mental Health Difficulties
The CCYPV (2020) examined linked administrative data for a cohort of 4,942 children who exited OOHC in Victoria across 2006–2014. They found 51.6% of young people in the cohort were registered in the state-wide acute mental health database and 32.4% in the state-wide AoD database. The majority who exited from either residential care (71%) or foster care (59%) were found to have been registered with acute mental health services (CCYPV, 2020). This indicated that large portions of the OOHC population sought support for mental health or AoD through state-funded services such as hospitals. Similarly, Martin et al. (2021) reviewed records of 1,848 individuals who left care in Victoria in 2013 or 2014 between the ages of 15 and 18 years. They found 18% presented at emergency departments for self-harm and a further 20% presented due to mental health concerns.
The three-wave ‘Beyond 18’ Victorian study presented similar findings. Wave one surveyed 202 young people (85 were still in care, 107 had left care) aged 16–19 years. They found 45% reported ‘very high difficulties’ with peer relationships and over 25% reported ‘very high degrees of emotional difficulty’ (Muir & Hand, 2018, p. 6). The second wave sample of 126 participants (97 care leavers—including 15 who were young parents—and 29 still in care) indicated poor psychological well-being, and 25% were found to experience levels of psychological distress that indicated a likely depressive or anxiety disorder (Purtell et al., 2019). Compared to community samples, care leavers had high levels of financial stress and psychological distress (Purtell et al., 2019). Young people who felt unprepared to leave OOHC had the highest levels of psychological distress, and a poor sense of life control. The third wave examined 126 care leavers (19 were young parents), and reported that those who were not engaged in activities such as employment or education generally had poorer mental and physical health, higher levels of distress and lower levels of life satisfaction, than those who were engaged in such activities (Muir et al., 2019).
Fernandez et al. (2016) accessed a sample of 669 adults nationally who were in care as children between 1930 and 1989 (hereafter ‘older care leavers’). Current mental illness was reported by 59% of the population, and over 70% disclosed treatment for mental illness in the past. In all, 65% reported experiencing suicidal ideation at some point in their lives and 39% had attempted suicide. These rates are far higher than the general population (Fernandez et al., 2016).
Psychosocial Complexity
Many authors commented on intersectionality and complexity of mental distress, behavioural issues and other concerns such as finances, unemployment, disability, housing, youth justice involvement or AoD use (Martin et al., 2021; Mendes et al., 2020; Muir et al., 2019; Fernandez et al., 2016; Purtell et al., 2016, 2019). McDowall (2020) surveyed 325 care leavers aged 18–25 years nationally, and found 10% reported a psychiatric disability. Similarly, analysis of care records of 166 youth aged 16–18 years in Victoria identified reference to a disability (commonly an intellectual or cognitive impairment) in 36% of cases, despite disability status not being captured as a standard data set (CCYPV, 2020). They also found 17% had a connection with youth justice.
Another review of records of 1,848 young people with experience of OOHC found AoD treatment had been sought by 21% of the sample, and one in five had youth justice community orders (Martin et al., 2021). Conflict and relationship difficulties was a prominent theme, and one suggested to be linked to struggles with mental health or emotional regulation (Muir et al., 2019; Purtell & Mendes, 2020). Other authors noted stress and anxiety were widespread, alongside what are commonly labelled as challenging behaviours such as use of violence and AoD use (Purtell et al., 2016).
Impact of Formal Supports, Child Welfare Services and Informal Supports on Mental Health
Researchers noted positive informal supports and relationships with others play an important role in enhancing mental health for the OOHC population (CCYPV, 2020; McDowall, 2020). Monson et al. (2020) found the quality and stability of placements appeared to correlate with good mental health. Rahamim and Mendes (2016) asserted that mental health was fostered by positive relationships and supportive social networks. Similarly, Muir et al. (2019) noted that life challenges can be mitigated with ongoing and consistent support from carers, family, partners, friends or key workers.
Care leavers reported they wanted home style environments, where their needs were attended to, alongside respectful, meaningful and consistent relationships with care givers (Smales et al., 2020). Participants in a study by Purtell and Mendes (2020) said they valued continuing care workers with specialist knowledge of programs, services and opportunities for young people. They also described how attuned workers could avert mental health crisis even just by being available to speak with. These findings were echoed by Monson et al. (2020) who reported that care leavers valued home-like environments and relationships with carers and workers who have good interpersonal and communication skills. They also welcomed an opportunity to talk about their needs, be involved in decisions about their care and access mental health treatment when it was needed.
Leaving Care
Vulnerability
Findings suggested socioeconomic and mental health vulnerabilities come to the forefront in the leaving care phase, which prior to the recent extended care reforms, began at no later than 18 years. For some, leaving care planning started at 15 years. Authors agreed that leaving care is a time of increased stress, with reduced stability and changes to accommodation and formal relationships (McDowall, 2020; Muir & Hand, 2018; Purtell & Mendes, 2020; Rahamim & Mendes, 2016). Rahamim and Mendes (2016) observed unaddressed mental health concerns had significant impact on the success of transition from care, noting associated stress could exacerbate or trigger mental health conditions. Similarly, Purtell and Mendes (2020, p. 59) noted lack of stability during the leaving care phase can ‘contribute to spiralling issues and compromised mental health’.
Transition Planning
At the time of the transition from OOHC, mental health and AoD concerns were often not addressed, and appropriate service linkages not established. The CCYPV found ‘more than two-thirds of young people with mental health issues (67%) and more than one-third of young people with substance use issues (37%) did not receive the help they needed to address these issues before they left care’ (2020, p. 26). Purtell et al. (2016) stated those with more complex presentations needed ‘very strong advocates’, a scant resource in an underfunded sector. For many care leavers, obtaining ongoing accommodation was particularly challenging. The records of 1,848 Victorian care leavers, who left care in 2013 or 2014 between the ages of 15 and 18 years, were reviewed by Martin et al. (2021). They noted (p. 66), ‘54 per cent of the cohort accessing homelessness services in the four years after exit, and high levels of repeat use of SHS [Specialists Homelessness Services]’.
Muir and Hand (2018) found preparation for transition from care was uneven, often lacking formal planning, or alternatively based on plans that focussed on immediate and basic care needs such as housing, rather than comprehensive care plans that prepare a young person for leaving care and embedding themselves in the broader community. Their study of 200 young people found that over a third indicated they were not able to access the services they needed in care (Muir & Hand, 2018).
Gaps in mental health linkages remained after transitioning out of care. McDowall (2020) asked 325 care leavers aged 18–25 years about their needs, and around 20% indicated they needed mental health support (2020). Similarly, Smales et al. (2020) asked 10 young people aged 18–27 with experience of OOHC what health services they needed, and their responses indicated mental health support remained a high priority.
Options for Mental Health Support are Inadequate
The review found a number of systemic and structural barriers that could impede access to and engagement with mental health and other services. Authors noted there are often complexities related to social and emotional development and mental health symptomatology in the OOHC population, meaning many existing services did not meet their needs (McDowall, 2020; Muir et al., 2019). Researchers found that long-term relational based supports were beneficial to those experiencing behavioural issues or a history of trauma (Muir & Hand, 2018). Yet, consistent methodical or organised health care was hard to maintain due to relocation between different catchment areas or clinics, particularly where there was instability in OOHC placements or accommodation (Muir et al., 2019).
Services in Australia, particularly those that were publicly funded, had restrictive eligibility requirements or lacked capacity to support the complex presentations often seen in the care leaver population (McDowall, 2020; Muir & Hand, 2018; Rahamim & Mendes, 2016). Concerns were raised about differences in eligibility criteria between catchment areas whereby those accessing public youth services in one catchment may no longer be eligible in another, or may transition to an adult service without any equivalent program (Rahamim & Mendes, 2016).
Services in the private sector were observed to be mostly unaffordable for care leavers (McDowall, 2020; Muir & Hand, 2018). Low-cost options such as bulk-billing or free programs potentially required participants to sacrifice the benefits provided by a long-term therapeutic relationship with a familiar counsellor (Purtell & Mendes, 2020). It was noted that low-cost programs may have other limitations related to duration of care or number of sessions, which created other barriers to engagement and disruption to care relationships (Mendes et al., 2020).
For older care leavers, finances were a major barrier to accessing services. Fernandez et al. (2016, p. 14) surveyed 669 individuals who reported key difficulties that included ‘inability to afford the costs involved (69%), lack of information about services (34%), stigma (30%), lack of available services (24%), lack of transport (21%), and work commitments (6%)’. It was clear that individual ability to locate programs and engage with them varied, and there were major gaps in availability of appropriate services across the lifespan.
Proposed Policy and Practice Reforms
Many authors called for extension of supports and development of uniform policies and legislation nationwide. Some suggested increasing the leaving care age to 21 years nationwide (CCYPV, 2020; Martin et al., 2021). Others called for extension of supports to the age of 25 years and for consideration of further priority access to services (Fernandez et al., 2016; McDowall, 2020). Rahamim and Mendes (2016, p. 8) noted a need to match leaving care programs to ‘reflect the maturity and developmental needs of the young person rather than just ending formal supports abruptly at a specific chronological age’. They called for ensuring gradual transition and flexibility so that supports do not all change or end at once. There were calls to address gaps in care, for example where public services were not available, or not suitable due to complexity or specific care needs.
Several researchers discussed the need for mental health services that were tailored, flexible and accessible (Barker et al., 2022; CCYPV, 2020; Purtell et al., 2016; Rahamim & Mendes, 2016). They called for specialised mental health services that were assertive, provided outreach models, were available to address prodromal or emerging illnesses and which sought to treat the trauma experienced prior to, during and after leaving care. Duff et al. (2022) found effectiveness in assertive case management, specifically to help access and maintain stable housing. Purtell et al. (2016) suggested having the option to fund private services in cases of gaps in service delivery, alongside holistic and wraparound supports. Several studies highlighted the benefits of integrated services which would allow more holistic support and intensive treatment to address concerns such as mental health and substance use (Duff et al., 2022; Monson et al., 2020; Muir et al., 2019; Purtell & Mendes, 2020).
Establishing Appropriate Supports
Researchers urged greater focus on establishing mental health treatment whilst in care and before leaving care (CCYPV, 2020; Martin et al., 2021; Monson et al., 2020; Muir & Hand, 2018; Purtell et al., 2016). Mendes et al. (2020) specifically noted a need for greater emphasis on early intervention, to ensure needs are identified and supports established while in care. Duff et al. (2022) found provision of appropriate supports ‘raises the possibility of improving health and wellbeing, employment and education, social participation and inclusion’ (2022, p. 68). Certainly, unmet mental health needs appear to lead to long-standing impacts in mental health for this vulnerable population.
This review identified a trial program called the Ripple Project targeting the mental health of young people aged 12–17 years living in OOHC in Victoria. It sought to reduce expressions of self-harm such as suicide attempts and substance abuse, as well as lowering homelessness, social isolation and contact with the criminal justice system (Herrman et al., 2016). Through a 5-year controlled trial, it delivered a structured model of support for carers in OOHC while encouraging early identification of mental health need and linkage to treatment and support for mental illness and behavioural problems (Herrman et al., 2016). The trial is expected to be completed in 2023.
The review also found two programs trialled in the State of Victoria, which failed to secure ongoing funding. The Berry Street Stand By Me program provided an intensive transition planning phase, with access to flexible brokerage, holistic supports, advocacy, care planning, access to sustainable housing and tailored therapeutic supports (Purtell et al., 2016). The evaluation indicated improvements in complexity, reduced risk of poor outcomes and significant savings to State Governments due to reduction in reliance on state services when exiting care (Purtell et al., 2016).
Additionally, the Salvation Army Westcare Continuing Care Program assisted young people during their transition from OOHC, through a relationship-based model of care, providing support and referrals to relevant services. Contact with Continuing Care workers supported mental health, helped to avert crises such as deteriorating mental health and housing issues and consequently improved engagement in employment and education for young people who may otherwise have disengaged from services (Purtell & Mendes, 2020). These studies highlighted improvements in mental health outcomes for care leavers when skilled and well-resourced workers, who understand the needs of care leavers, engaged with them to build meaningful lasting supports.
Workforce
Studies called for advanced training for OOHC workers on mental health, for mental health workers on OOHC, and for others who are likely to come into contact with this population, such as AoD workers or police (Herrman et al., 2016; Monson et al., 2020). Rahamim and Mendes (2016) suggested specialist mental health training so workers with established relationships can engage better with early identification and intervention for mental health concerns. They also called for investment in meaningful mentorship with social and group programs. Similarly, Fernandez et al. (2016) suggested specialised mandatory trauma informed training for workers in services that older care leavers would access, such as the aged care sector.
It appeared that existing services would benefit from further training to engage with the mental health needs of this client group meaningfully and successfully. It was also suggested that services such as youth justice, AoD, child protection and mental health would otherwise be improved with better cooperation, collaboration and coordination, including handover of information (Duff et al., 2022; Fernandez et al., 2016; Martin et al., 2021; Purtell and Mendes, 2020). Authors noted changes would avoid unnecessary retelling of experiences of trauma, improve early identification of mental health need and timely delivery of services. Fernandez et al. (2016) argued that focus on coordination with communities especially Indigenous communities, could support mental health, including culturally appropriate healing. Mendes et al. (2020) suggested the Indigenous population would also benefit from tailored services, with focus on meaningful cultural connectedness.
Greater Participation of Lived Experience in Policy Development
Many researchers called for improvements in engaging those with lived experience. Several authors suggested services could improve youth participation, and better involve youth in decisions about their care and their futures (CCYPV, 2020; Duff et al., 2022; Monson et al., 2020; Smales et al., 2020). This review identified a randomised trial called the Bounce Project, which recruited a sample of young people with lived experience to contribute to a mental health promotion intervention (Rafeld et al., 2020). This study highlighted a lack of meaningful opportunities for those with lived experience to engage in research, noting there are specific barriers to participation experienced by this population, requiring considered design to promote engagement (Rafeld et al., 2020).
Smales et al. (2020) recommended inclusion for lived experience in all future work related to the sector, including research, programs, training, services and policy development. Martin et al. (2021) suggested better involvement of youth with lived experience into policy design. Researchers noted a need for better data collection, including post-care, by better identifying those with experience of OOHC in health outcome data (Fernandez et al., 2016; Martin et al., 2021; Rahamim and Mendes, 2016).
Outcomes for Specific Populations
Residential Care
Limitations in data made it difficult to distinguish mental health outcomes by care type. However, outcomes from a sample of young people who completed the Strengths and Difficulties Questionnaire measuring psychological well-being found those in residential care had the highest total difficulties scores (Muir & Hand, 2018), indicating high levels of distress and social difficulties. Their emotional and interpersonal challenges were attributed to traumatic life experiences including the ‘physical and emotional disruption’ of life in OOHC (Muir & Hand, 2018). Furthermore, the CCYPV (2020) found those with a history of placement instability and those exiting from residential care had the poorest mental health outcomes. While there are many possible explanations, this could indicate that young people with the highest degrees of complexity are more likely to be relocated, or the experience of multiple types of care or care placements is destabilising.
Indigenous Care Leavers
Findings indicated mental health concerns were widespread in the Indigenous care leaver population. One study of 64 Aboriginal young care leavers found almost one-third had mental health concerns such as depression, self-harm and suicide attempts, while 11 had drug and alcohol issues, and five were managing chronic health conditions (CCYPV, 2020). Purtell et al. (2016) noted that Indigenous concepts of family and community were at odds with the Western individualistic organisation of the child welfare system. Mendes et al. (2020) completed a scoping study specifically examining the Indigenous care leaver population, and found that ‘poor mental health for some Indigenous care leavers was seen as a direct outcome of layered disadvantage; experiencing trauma, abuse or neglect, growing up in OOHC, and being disconnected from their culture and community’ (2020, p. 191). Meaningful cultural connectedness was found to be a key contributing factor in enabling success and happiness later in life for the Indigenous population, and linked to strong mental health and well-being, yet these needs are often not met through generalist mental health programs (Mendes et al., 2020). While a large proportion of the OOHC population is Indigenous, it appears their specific needs are often not addressed by services.
Early Parenting Care Leavers
The CCYPV (2020) examined a cohort of more than 4,942 young people aged 15–18 years who exited care between 2006 and 2012, and found that ‘16% of [the] cohort became parents while still in care or within three years of OOHC exit’ (2020 p. 61). However, only a few articles collected data or presented discrete findings regarding the mental health of young parenting care leavers. Barker et al. (2022) specifically surveyed seven parenting care leavers and found that mental health support was identified as a key need. Another study identified 15 parenting care leavers in their cohort, identifying the usual challenges that would be faced by young parents such as ‘difficulties finding or affording appropriate housing, finding employment or dealing with the complex emotions of becoming a parent’ (Muir et al., 2019, p. 32).
It is likely that young care leaver parents experience aspects of disadvantage related to their mental health that other young parents would not encounter. For example, Barker et al. (2022) noted when symptoms of trauma are untreated, there can be impacts on parenting and individual capacity to cope, and that contact with child-protection services can be a difficult experience, particularly if the child of a parenting care leaver was removed. Muir et al. (2019) noted parenting care leavers were less likely to be engaged in education or employment. They suggested these factors could lead to lower incomes and higher levels of financial stress alongside further vulnerability in the future, which would likely impact longer term mental health and well-being. These layers of disadvantage may also result in intergenerational experiences of the child-welfare system.
Older Care Leavers
One major study explored the experiences and needs of 669 older care leavers, defined as those who spent time in institutions and other forms of OOHC from 1930 to 1989 (Fernandez et al., 2016). Their findings detailed severe suffering, abuse and neglect while in care alongside long-standing psychosocial disadvantage. These included financial hardship, poverty, addictions and limited opportunities for employment or study alongside ‘chronic illness, disability, relationship breakdown, homelessness, social isolation, anxiety and depression’ (p. 237). Nevertheless, they identified internal resilience and survivorship which was demonstrated by all participants in the study, and discussed some of the factors that people reported had helped such as access to confidence building and nurturement through education, stability, employment, interpersonal relationships or recreational groups, or a serendipitous connection with an individual who offered relevant support.
Many from this cohort have expressed major concern about contact with institutions such as inpatient and aged care facilities, fearing ‘a return to the vulnerability, fear and disempowerment they experienced as children’ (p. 236). Fernandez et al. (2016) suggested a need to recognise all care leavers as a special needs group, and to consider priority access to services such as home care packages and mental health treatments.
Discussion, Limitations and Suggestions for Further Research
This article reviewed 17 studies related to the mental health care needs and outcomes for youth transitioning from OOHC in Australia between 2015 and 2021. There were persistent findings of high rates of suicidal ideation, deliberate self-harm and mental illness for those with lived experience of OOHC. These appeared throughout the lifespan, indicating needs are not met sufficiently by existing services.
While trauma, mental health and recovery present a complex web of interconnected contributing factors, findings suggested any socioeconomic or mental health vulnerability was likely to be exposed during the leaving care phase, commonly 15–18 years. There were many suggestions to reshape systems to better support the developmental needs of care leavers and the advancement of positive mental health outcomes, both while in OOHC and for those with care experience in the broader community.
Extension of Care
Authors agreed there was a need for the development of uniform national policies and legislation. Studies called for leaving care ages to be extended, some to reflect individual capacity rather than an arbitrary age, whilst others specifically recommended extending to 21–25 years. This would be more consistent with the opportunities experienced by other young people in the community, replicating community interdependence in the leaving care system (Mendes et al., 2011).
Improving Stability and Connectedness While in Care
There seemed to be a relationship between mental health difficulties and factors such as a lack of stability in care or accommodation, financial difficulties and poor engagement in social, recreational or employment activities. Those exiting from residential care or with a history of placement instability had the poorest mental health outcomes. Studies suggested a possible connection between particular care types and psychosocial difficulties, as has been noted in international literature (Sacker et al., 2021).
It is possible that individuals with complex presentations are more likely to be in residential care or have multiple placements. However, authors noted these environments have factors that would be further destabilising for mental health, such as lack of consistent care givers and other stressors. Similarly, establishing protective factors such as friendships, emotional supports and services to treat mental health concerns would be challenging under these circumstances. Conversely, stability in placement or accommodation would allow opportunities to establish relationships with others, link with suitable services and engage meaningfully with vocational activities such as work or study.
Young people appreciated placement stability with opportunities to form strong social connections in their local communities. They requested more holistic and stable support, including connections with others. Where stable relationships with workers were established, these could be therapeutic and appeared to allow earlier identification of concerns. Familiar workers who know a person well may be better placed to detect early symptomology or warning signs of mental illness or implement crisis intervention when rapid action is needed. Young people may feel more able to disclose their concerns and seek support. Furthermore, creating lasting and meaningful linkages would likely improve confidence and mental health.
Improving Transition Planning and Establish Supports
Researchers found evidence of poor transition planning. Some did not have established supports, while others had supports that did not meet mental health needs appropriately. While existing mental health challenges, emotional difficulties or psychosocial disability may present challenges to care planning, it was challenging for people to establish themselves within communities and link with professional supports after leaving care. Research demonstrated youth benefitted from perseverance and advocacy to ensure service linkages were established before leaving care.
Improving Accessibility of Supports and Targeted Programs
Layers of disadvantage formed significant barriers for care leavers across the lifespan to access useful supports. This included the adverse impact of traumatic childhood experiences on formation of positive social connections. People experienced difficulties with instability, finances, accommodation, relationships and recreational activities.
While public youth specific services could broach some of these barriers with flexibility and outreach models, adult services are typically more stringent in their eligibility criteria and models of care. Individual abilities to engage with services varied, and so did the availability of appropriate services. Many fell into a ‘missing middle’—eligibility criteria, psychosocial disadvantage, mental health symptoms, transient accommodation and AoD use made it challenging to have these same concerns addressed.
Make Services More Appropriate for Care Leavers
Authors noted a need for workforce training to improve awareness of the OOHC sector in the mental health sector and vice versa. Many authors called for priority access to services and supports after transitioning from care, noting the benefit of targeted programs. An initial step could include recognising care leavers at points of intake, and attempt to identify and address their specific needs.
Some called for changes to information sharing to ensure services were delivered in a timely and coordinated manner, without need for those with care experience to rehash histories of trauma and repeat their stories. This would need to be balanced with respect for individual preferences and confidentiality, and it is possible that trauma informed approaches would help mitigate some of the risks and concerns. There would certainly be benefits in ensuring services are more integrated and working together more effectively.
Overall, services would benefit from improved understanding and careful consideration of care leaver needs. Aged care and mental health facilities share processes and procedures that are highly triggering for those with childhood experience of institutionalisation. There is an urgent need to enact reform throughout the service sector to avoid continued re-traumatisation.
Address Needs of Specific Populations
The review found young care leavers who are young parents encounter layered disadvantage impacting mental health and well-being in the long term, which may result in intergenerational experiences of poverty and the child-welfare system. Authors called for non-punitive and tailored, age-appropriate support across sectors, particularly mental health and child well-being.
Results indicated mental health concerns for Indigenous care leavers were widespread, and services were not meeting their needs. Authors noted a link between meaningful cultural connectedness and strong mental health and well-being, yet noted these needs are often not met through generalist mental health services. They called for more awareness alongside provision of culturally appropriate interventions that recognised the broader family and community connections and obligations of Indigenous youth.
The older care leaver population were found to have experienced serious trauma resulting in lifelong mental health struggles and multiple layers of long-lasting disadvantage. This further compounded mental health symptoms and complicated access to support. Researchers called for services to be more aware, to get better at identifying older care leavers, understanding their needs and ensuring supports are appropriate—and not re-traumatising.
Limitations
Most if not all studies reviewed were conducted before the introduction of extended OOHC care options in all Australian jurisdictions, hence do not reflect the positive impact of extended care on transition experiences including mental health. However, the outcomes of this review support this policy change. Future research will ideally review studies that have directly examined the impact of extended care on mental health needs and outcomes.
Many studies either did not include or did not report members of their samples as Indigenous, or the sample was not representative of the high numbers of that population known to be in OOHC. Future research would ideally recruit samples that are representative of the high proportion of Indigenous youth within care leaver demographics.
Many of the studies examined did not differentiate between care types. Others reported mixed information such as most recent care type or types experienced. Future research would ideally identify total years in care and length of time in each care type in their results.
The COVID-19 and related restrictions are likely to have had adverse mental health impacts for care leavers in the Australian context. Given that the length and degree of lockdowns varied considerably across the eight states and territories, future research might also usefully interrogate the different impact of these restrictions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.