
Abstract
Organizational learning theory has long recognized the advantages of sequential repetition, since successive events allow organizations multiple opportunities to iteratively refine their approaches. In many situations, though, events unfold so quickly that they can overlap, becoming more clustered or concurrent rather than sequential and successive. This raises a tension; this might impede learning by reducing the time available to examine outcomes and update routines after each round, or it may instead motivate organizations to learn and get better out of necessity since less room exists for error. This study responds by distinguishing between the effects of concurrent experiences on different sets of routines. The study predicts that learning in the focal area will suffer, but that learning on supportive and ancillary routines will be enhanced as organizations experiment and explore for broader ways to build resilience under these challenging circumstances. Tests on nursing homes’ responses to clustered outbreaks during the COVID-19 pandemic provide strong support for the prediction about focal outcomes and partial support for the prediction about supportive outcomes. The study contributes to learning theory by advancing work on timing and demonstrating how organizations can learn to build resilience even if they cannot always learn to get better.
Keywords
Introduction
Organizational learning can occur as organizations engage in repetitive tasks or activities, where organizational members repeatedly observe outcomes and develop or adjust their understandings of the approaches that led to those particular outcomes (Argote & Miron-Spektor, 2011; Egelman et al., 2017; Levitt & March, 1988). Using this knowledge, organizations can update or refine their routines and procedures before engaging in the next round of activity, leading to an iterative and extremely well-studied process of learning through experience with repeated activities within organizations (Argote et al., 2021; Bingham & Davis, 2012; Levitt & March, 1988; Rerup & Feldman, 2011).
In many situations, though, experience does not arrive in iterative sequences that allow for adequate learning and reflection in between trials (Bingham & Davis, 2012; Eggers, 2012; March et al., 1991). The COVID-19 pandemic brought this possibility into stark relief, as individuals, communities, and organizations attempted to learn, adapt, and perform under new and often previously unfathomable strain. Many of these problems were felt acutely within the elderly care system; in the United States alone, almost half of all tracked nursing home residents had or likely had been infected by the end of 2020 (Hochman, 2020), and over 200,000 residents and staff had died from the disease or its complications by the end of 2021—representing nearly one out of every four deaths in the country (Chidambaram, 2022). Within this and other settings, COVID-19 infections often arrived in waves, with many cases occurring concurrently or at the same time. Retrospective accounts from nursing home staff, residents, and family members recall numerous, distressing situations where a high volume of simultaneous infections overwhelmed facilities and led to dramatic deteriorations in resident care and infection control (Hochman, 2020). Although organizations are well known to learn through their experiences (Levitt & March, 1988), these events highlight the importance of timing and pace in that organizational learning process. Organizations that gain similar volumes of experience are likely to learn very different things, depending on how those experiences arrive over time.
Although several learning theories have implicitly acknowledged or accounted for the timing or sequence of various events or experiences (Cyert & March, 1963; Levitt & March, 1988; March & Olsen, 1976; March et al., 1991), recent research has focused much more directly on timing and its central role in the learning process (e.g., Bingham & Davis, 2012; Castellaneta et al., 2022; Musaji et al., 2020; Rerup & Zbaracki, 2021). Much of this work considers the difficulties of learning through extremely rare events, which tend to require deliberate and sustained attention to yield useful knowledge (Lampel et al., 2009; March et al., 1991; Maslach et al., 2018; Rerup, 2009; Rerup & Zbaracki, 2021). At the other end of the spectrum, less work examines extremely frequent events, but this nascent literature suggests two competing views about how organizations might learn under these circumstances. On one hand, some research supports the notion that more frequent experiences lead to better performance, presumably because a faster pace provides more opportunities for learning through repetition while also reinforcing the need to learn out of necessity because less room or time exists for error (Desai & Madsen, 2022; Eggers, 2012; Musaji et al., 2020). On the other hand, though, faster pacing can increase cognitive load and provide decision-makers with less time in between rounds to articulate lessons, codify knowledge, and update routines; as a result, some research finds that more frequent experiences can actually impede learning and performance (Castellaneta et al., 2022; Castellaneta & Zollo, 2015; Hayward, 2002). Navigating between these perspectives is theoretically important given that the learning process may look quite different when experiences arrive so frequently that trial and error or other forms of experiential learning become difficult (Aguinis & Bakker, 2021; Castellaneta & Zollo, 2015; Levitt & March, 1988).
This study contributes to this line of research by examining learning through experiences that can occur so frequently that they may actually overlap or become “concurrent” (Eggers, 2012; Rockart & Wilson, 2019), and the study considers mixed findings about how frequency affects learning and performance by stepping back and asking how increasingly concurrent experiences might affect different routines within the organization in distinct ways. First, the study examines routines directly related to focal experiences, and the study’s framework suggests that learning and performance on these directly related routines will suffer when experience with a focal activity or event becomes more concurrent. This is predicted to occur because associated experiences are greatly compressed over time, with fewer opportunities for iteration or trial-and-error as these events unfold; thus, these situations simply provide fewer chances to develop accurate cause-and-effect understandings and iteratively adjust focal routines in response to new information (Argote, 2013; Levitt & March, 1988). However, the study’s framework also proposes that concurrent experience leads to greater exploration and experimentation, out of necessity, as organizations seek broader ways to build resilience and indirectly support their focal activities under such strain (Cyert & March, 1963; March & Olsen, 1975; March, 1991). To make these latter arguments, the study borrows from the theory about the resource-based view (RBV) and also from related arguments about developing organizational capabilities under pressure or strain (Crilly et al., 2012; Kahn et al., 2018; Natividad & Sorenson, 2015). Although overlapping or concurrent experiences will make learning and performing well on focal routines much more difficult, these RBV theories about capabilities and strain suggest that these experiences will also motivate and incentivize organizations to learn and build resilience in other indirectly supportive ways, leading to better performance on tangential or ancillary routines outside of the focal area.
Associated hypotheses are tested on a unique and extensive facility-level, weekly database of COVID-19 case experience and facility inspection outcomes across all reporting nursing homes in the United States, using an approach that directly adjusts for endogeneity in inspection selection. Findings provide strong support for the prediction about the difficulties in learning involving focal routines, as case experience volume leads to lesser improvements in infection control routines and other procedures directly related to COVID-19 mitigation when that case experience becomes more concurrent in timing. The study also finds partial support for the prediction about supportive routines, as case experience volume leads to greater improvements (in some models) in tangential and ancillary areas, such as on routines for hospital partnership or broader facility (non-infection) quality improvements, when that case experience becomes more concurrent in timing. Contributions to learning theory and other related literatures are described following the study’s theoretical framework and empirical tests.
Theory and hypotheses
Learning and the timing of experience
While various approaches to organizational learning have been proposed, a particularly robust and influential body of research has coalesced around learning through experience with recurring tasks, activities, or events (Egelman et al., 2017; Haunschild et al., 2015; Haunschild & Sullivan, 2002; Levitt & March, 1988). According to this perspective, repetition provides opportunities for an organization’s members to observe outcomes, generate causal inferences about the connections between their actions and those outcomes, and explore refinements through trial-and-error, with the aim to improve these outcomes in the future (Argote, 2013; Cyert & March, 1963; Levitt & March, 1988). Organizational learning occurs as these changes become codified and embedded into the organization’s routines, procedures, and knowledge repositories, leading to the familiar and robust “learning curve” pattern where increasing experience leads to better organizational outcomes, albeit at a marginally declining rate (Kim et al., 2009; Kim & Miner, 2007; Lapre & Tsikriktsis, 2006; Madsen, 2009; Musaji et al., 2020).
Research in this tradition increasingly recognizes the distinct importance of experience timing or pace (Luoma et al., 2017; Maslach et al., 2018; Rerup, 2009; Rerup & Zbaracki, 2021; Zollo, 2009). Research on rare events can provide some guidance about this cadence and its importance (Lampel et al., 2009; March et al., 1991; Maslach et al., 2018; Rerup & Zbaracki, 2021). Given their lack of regularity, rare events provide incomplete understandings about the cause-and-effect connections between organizational actions and outcomes (Lampel et al., 2009; Zollo, 2009). To learn under such ambiguity, organizations must depart from standard trial-and-error learning processes, and instead invest considerable time, attention, and energy into sensemaking, deliberate learning, and other active forms of comprehension and codification (March & Olsen, 1976; March et al., 1991; Rerup, 2009).
Related research is also beginning to examine learning through extremely frequent experiences, such as those that are clustered closely together over time, and this work also suggests that the learning process can look quite different under these circumstances as well (Castellaneta et al., 2022; Desai & Madsen, 2022; Eggers, 2012; Rockart & Wilson, 2019). Two views on this learning process have emerged. First, some research suggests that greater frequency can increase the motivation to learn, since the faster pace forces organizations to improve their processes and performance more rapidly and leaves less room for errors or inefficiencies (e.g., Desai & Madsen, 2022; Musaji et al., 2020). However, alternative research suggests that an increased frequency can actually suppress the motivation or ability to learn, since this situation “reduces the time organizations have to process, evaluate, and reflect on gathered information . . . pace also increases information load . . . [and] increases the cognitive burden on actors” (Musaji et al., 2020, p. 211). And, as Castellaneta and Zollo (2015, p. 144) note, “short time intervals between past experiences might lead firms to incorrectly specify the connections between actions and outcomes, which may in turn increase the risk of forming vicious routines through superstitious learning processes” (Levitt & March, 1988; Zollo, 2009).
As a result of these conflicting perspectives, researchers are perhaps justified to lament that “we simply do not know how change in attributes [of experience], like their number and pace . . . shape the strategic experience-performance relationship” (Musaji et al., 2020, pp. 209–210). In the following section, I consider concurrent experiences (i.e., those that become more frequent or clustered together to the point that they can even overlap), and I develop a theory about how increases in concurrence can affect learning.
Concurrence and learning on focal versus supportive routines
When experiences increasingly occur in very tight clusters or even concurrently, organizations face competing pressures. On one hand, learning through experiences with the focal activity can naturally become more difficult since fewer opportunities and less time exists to articulate and codify knowledge; but, on the other hand, these circumstances can induce strain and reinforce the need to learn and improve much more rapidly to keep better pace with events as they quickly unfold. I reconcile these competing pressures by drawing from research on the RBV, and from related arguments on developing dynamic capabilities under organizational strain (Eisenhardt & Martin, 2000; Kahn et al., 2018; Milosevic et al., 2018; Wernerfelt, 1984; Winter, 2003). Using these perspectives, I distinguish between focal and supportive routines, and I develop a theory regarding how concurrence affects learning on both sets of routines.
The distinctions between focal and supportive routines
Research on the RBV and dynamic capabilities recognizes that organizations, when faced with internal or external pressures, can respond by developing additional capabilities, routines, and processes in key areas such as product development, quality and reliability, and strategic decision-making (Barreto, 2010; Wernerfelt, 1984). In addition, related research on capability development under pressure recognizes that adverse events and unexpected situations do not affect the whole organization equally but instead affect “that part of the organization in which it is most directly located . . . the primary actor is not the organization-as-a-whole but its parts—groups, teams, functions, departments, and hierarchical levels [emphasis in original]” (Kahn et al., 2018, pp. 509–510). Thus, this research supports the notion that the routines and activities that are directly affected by adversity or strain can be conceptually separated from other routines and activities throughout the organization (Raetze et al., 2021).
Related theory also suggests complex connections among these elements; adversity in one activity or area within the organization can motivate or lead other areas, units, or the overall organization to consider providing (or, in some cases, withholding) resources and support to the focal area (Kahn et al., 2018). This support may take several forms; for instance, better relationships can be established between the focal unit or activity and other parts of the organization to draw in support from these other areas, or similar linkages could be created with suppliers, alliance partners, and other external resource providers to support the organization as a whole (Kahn et al., 2018; Tyler & Caner, 2016). More indirectly but equally important, managers and employees can work to correct problems elsewhere in the organization, resolve “low hanging” or easily addressable concerns on other activities, or otherwise improve performance on other tasks to free up time, attention, and operational capacity or slack for handling issues in the focal area more effectively (Haunschild et al., 2015; Ramanujam & Goodman, 2003; Roberts, 1990; Vogus & Rerup, 2018). Simply stated, a clear theoretical boundary exists between these constructs; although they may both contribute to performance in a focal area, focal routines primarily govern activities and iterations in that specific area, and supportive routines govern activities that either span multiple areas or exist in distinct areas with a much more indirect (though still relevant) connection with performance in the focal area.
More specifically, research on organizational routines and rule systems from a network perspective tends to view organizational routines and processes as existing in groups or clusters, with interconnections between various routines and activities performed by an organization’s members (Argote & Guo, 2016; Bucher & Langley, 2016; Donmez et al., 2016; Pentland & Rueter, 1994; Schulz, 1998; Schulz & Zhu, 2022). For instance, Schulz and Zhu (2022) determined that various clinical guidelines and practices in a Canadian regional health care organization were interconnected, with some existing closer to a particular activity domain (such as clinical care) than other more distant practices with fewer connections or references to that activity. Broadly speaking, studies in this literature as well as other literatures on core and peripheral organizational activities have echoed that certain routines or organizational behaviors can be closer, more centrally connected to, or more impactful on specific activities than other routines and behaviors (Anand et al., 2012; Argote & Guo, 2016; Hudson, 2008; Hudson & Okhuysen, 2009; Kahn et al., 2018; Sonenshein, 2014). A key finding in this research is that focal routines, centrally connected with a specific activity domain, tend to have more references toward or impact on that area than they do on other areas, while supportive routines tend to have an impact that is more widely distributed across a broader range of peripheral organizational activities as well as the focal activity domain (Schulz & Zhu, 2022; Sullivan, 2010).
Thus, in the current framework, a clear distinction between focal and supportive routines involves understanding the distribution of their impact. For instance, in a manufacturing context, routines for quality control, production timing, and packaging all centrally focus on the manufacturing process or product chain itself, while routines for payroll processing, hiring, and workforce training could be applied to workers within the manufacturing chain as well as employees across a wide range of the organization’s other non-manufacturing or support activities. Thus, the latter routines tend to have a more distributed impact, and as a result, they are supportive rather than focal to the manufacturing process.
Routines are often referred to as the basic building blocks of the organizational learning process, since knowledge from organizational experiences can be embedded into these procedures in order to shape or guide future approaches (Argote & Guo, 2016; Becker, 2004; Levitt & March, 1988). Despite this centrality, little work in the learning literature has distinguished between focal and supportive routines and how they may each be shaped by the learning that occurs through concurrent experiences. This is despite the recognition, in other literatures, that organizations may build resilience during times of strain (such as when multiple events occur concurrently) by refining both their central as well as peripheral or supportive approaches (Kahn et al., 2018). To dive deeper into how learning affects these processes, the next sections forward theory about how concurrent experience shapes learning and performance on focal routines, and how this differs from its effect on supportive routines.
Concurrent experience and learning on focal routines
Experiences that cluster together or overlap in time can interfere with learning in the focal area. With increasing concurrence, more experience unfolds before cause-and-effect understandings in that specific area can be formed, and before this knowledge can be codified into routines, since more actions and events in the focal area begin to transpire before the outcomes and feedback from prior events are known or processed (Argote & Guo, 2016; Fang, 2012; Konlechner & Ambrosini, 2019). This situation gives rise to causal ambiguity regarding action-outcome linkages, which is well known to impede the learning process and create room for superstitious learning, ineffective or incomplete actions, or even outright inertia (Lampel et al., 2009; March & Olsen, 1975; Rahmandad & Gary, 2023; Zollo, 2009). Concurrence also interferes with learning by simply providing fewer opportunities to iterate and adjust routines for a given volume of experience (Argote, 2013). For instance, for a hypothetical organization that produces multiple units of a product, producing these one at a time allows several chances to examine output and revise routines between each trial; these sequential opportunities are reduced (or eliminated) if the same number of units are produced simultaneously. As a result, organizational learning in the focal area should be weakened or suppressed when experience arrives in an increasingly concurrent pattern.
It is important to discuss a boundary condition associated with these arguments. The study’s theory presumes that production lines or productive capacity are relatively fixed, at least in the short run, and that increases in concurrence will occur relative to those fixed constraints (Vanacker et al., 2017). In settings where that is not the case, organizations may more naturally be able to expand their processes and collective attention to simultaneously evaluate multiple events as they occur, in parallel, and these organizations may find it easier to interpret those experiences and to generate less ambiguous understandings as a result (Eggers, 2012; Rockart & Wilson, 2019). However, significant challenges may nonetheless continue to impede the codification part of the learning process, since this situation still provides fewer sequential opportunities to integrate those understandings and adjust collective routines between rounds (Argote et al., 2021; Argote & Guo, 2016). Thus, relaxing this boundary condition may still lead to a similar, albeit slightly weaker, prediction. In addition, although organizations may establish relationships or update procedures to begin drawing in additional resources (a possibility that is expanded on in the next section), these operational resources take time to actually mobilize, transfer, and apply effectively into the focal area, suggesting that it is reasonable to consider productive or operational capacity as relatively fixed in the short run (Lecuona & Reitzig, 2014; Vanacker et al., 2017).
Collectively, these arguments suggest that organizations learn less effectively in the focal area when their experience in that area becomes more concurrent. Learning theory predicts that an increase in the volume of experience will be associated with a decline in the subsequent rate of problems when performing routines in the focal area of activity (Argote et al., 2021; Darr et al., 1995; Haunschild & Sullivan, 2002; Levitt & March, 1988; Musaji et al., 2020). The theory developed earlier suggests that this learning relationship will become less steeply negative (i.e., problems will be suppressed less well) when that experience is increasingly concurrent in its timing. This leads to two predictions: first, about the direct negative influence of experience volume on problems with focal routines based on existing learning theory; and, second, about the moderating impact of concurrent experience on this direct relationship.
Hypothesis 1. Experience volume leads to a negative effect on problems with focal routines.
Hypothesis 2. Experience volume leads to a less steeply negative effect on problems with focal routines when that experience arrives more concurrently.
Concurrent experience and learning on supportive routines
Although focal and supportive routines may both be associated with a specific area of organizational activity (with the latter exerting a more indirect influence, as previously discussed), there is an important theoretical difference between the two sets of routines, and this distinction leads to differences in how learning through concurrent experience affects each of these groups of routines. Focal routines depend centrally, directly, and fundamentally on knowledge gained through focused experiences with tasks and events in that specific area of activity (Argote & Miron-Spektor, 2011; Darr et al., 1995; Levitt & March, 1988). Thus, accurate cause-and-effect understandings in the focal area are necessary to improve these routines (Levitt & March, 1988), and concurrent experience tends to challenge these understandings and impede associated learning, as described in the previous section (Argote & Guo, 2016; Castellaneta & Zollo, 2015). In contrast, supportive routines benefit from knowledge and experiences gained in tangential, related, or overlapping areas of activity (Argote & Guo, 2016; Becker, 2004; Bucher & Langley, 2016; Schulz & Zhu, 2022). For instance, Schulz and Zhu (2022) discuss rules, although similar arguments can apply to other knowledge repositories such as routines. They provide the example of a health care rule about wound care, which they suggest is “highly relevant only to other guidelines involving wounds; it is moderately relevant to other guidelines on lifting and transporting patients” (Schulz & Zhu, 2022, p. 7). In this example, rules and routines that focus centrally on wound care tend to benefit the most from prior experiences involving this specific form of care, and although routines for transporting patients may also contribute to better wound care outcomes, those latter routines certainly also benefit and reflect experiences gained in a wide variety of tangential areas outside of wound care.
Thus, in contrast with its effect on focal routines, concurrent experience in a focal area may not challenge causal understandings or create as much ambiguity about supportive routines, since the knowledge required to refine these broader sets of routines can draw from a larger base of related and unrelated experiences throughout the organization (Argote & Guo, 2016; Milosevic et al., 2018; Schulz & Zhu, 2022). As a result, it is less likely that concurrent experience in a focal area will suppress learning in these supportive areas. Instead, concurrent experience in a focal area may actually contribute to learning and yield indirect enhancements to these supportive routines through another, related yet distinct set of learning mechanisms.
Specifically, since concurrent experience yields less time and provides less precise or reliable knowledge for learning in the focal area, organizations in this situation undoubtedly face greater challenges with managing and maintaining their performance in that area of activity. This pressure is compounded when the volume of experience or events in the focal area increases (relative to a fixed capacity constraint), as this means that an organization faces a greater activity load (from the increasing volume of experience) with shorter (or no) time to refine focal routines in between each iteration given the increasing concurrence of that experience (Castellaneta & Zollo, 2015). While this situation impedes learning through exploitation and refinement in the focal area, as previously discussed, it can also contribute to learning through exploration and experimentation in ways that lead to enhancements on supportive routines (March, 1991; Posen & Levinthal, 2012).
In these situations, the difficulties and strain with learning and managing performance in the focal area are likely interpreted as problems, which can motivate broader searches for solutions that can increasingly involve other routines, locations, and activities within as well as outside the organization (Cyert & March, 1963; March, 1991). This expanded search may quickly and naturally grow to encompass supportive routines (Gavetti et al., 2012; Gavetti & Levinthal, 2000; Posen & Levinthal, 2012). For instance, organizations may work to overcome these problems by developing external relationships to draw in additional resources or by identifying efficiencies and improvements in other tangential areas of organizational activity to free up more time and attention to devote toward focal activities. In addition, these situations can also motivate organizations to experiment with a much larger variety of routines, procedures, tasks, and activities to identify corrections and improvements somewhere—anywhere—within the broader organizational system (Castellaneta et al., 2022; Fang, 2012; Rahmandad et al., 2021; Rahmandad & Gary, 2023).
Collectively, the theory here suggests that concurrent experience in a focal area will motivate increased exploration and experimentation outside of that focal area, leading to better learning in tangential and supportive areas, which is ultimately observed through greater refinements or improved performance on supportive routines. Thus, concurrent experience in a focal area should moderate the direct learning relationship between experience volume in that focal area and the organization’s performance on supportive or tangential routines. There is little direct guidance in the learning literature regarding that main learning relationship between focal experience and supportive or tangential routines; however, enough theory exists to suggest a beneficial impact similar to the effect of experiential learning on focal routines. For instance, greater experience is well known to result in marginally diminishing returns on focal routines, as most of the available refinements to these routines will have already been identified and implemented as experience continues to increase (Argote et al., 2021; Darr et al., 1995; Levitt & March, 1988). In these situations, it is reasonable to presume that organizations with greater experience in the focal area will have also identified more improvements to associated, ancillary, or tangential routines, especially as additional refinements to focal routines become increasingly out of reach (Argote & Guo, 2016; Bingham & Davis, 2012; Schilling et al., 2003; Staats & Gino, 2012). Thus, a greater volume of experience in the focal area should lead to better performance (fewer problems) on supportive routines; that is, a negative relationship should exist between focal experience and problems involving these supportive routines. The theory here about concurrence suggests that this direct learning relationship will become more steeply negative (i.e., problems will be suppressed more effectively) when that experience is increasingly concurrent in its timing. These arguments lead to the following hypotheses.
Hypothesis 3. Experience volume leads to a negative effect on problems with supportive routines.
Hypothesis 4. Experience volume leads to a more steeply negative effect on problems with supportive routines when that experience arrives more concurrently.
Methods
Setting and data
Analyses are conducted on a longitudinal panel of Medicare-/Medicaid-Certified Long Term Care facilities (i.e., nursing homes) across the United States, tracked at the facility level on a weekly basis. Data were reported by nursing homes to the Centers for Disease Control and Prevention (CDC) National Health care Safety Network system and made available by the Centers for Medicare & Medicaid Services (CMS) Division of Nursing Homes/Quality, Safety, and Oversight Group/Center for Clinical Standards and Quality. These data were merged with information about nursing home inspections conducted by state inspection teams following CMS guidelines, as reported through data provided separately by CMS.
The first reported COVID-19 outbreak in a U.S. nursing home occurred in February 2020, and weekly tracking of facility information by the CDC began near the end of May 2020 (Ouslander & Grabowski, 2020; Quigley et al., 2020). However, this study’s analysis begins much later—in March 2021—for several reasons. First and foremost, the study’s outcomes involve inspection results, and although some inspections with an extremely narrow focus were conducted during the pandemic’s early stages, regular inspections and routine oversight were sharply curtailed in frequency and scope until late 2020 or early 2021 in most states and jurisdictions (Jones et al., 2021; Ouslander & Grabowski, 2020; Rubano et al., 2022). Therefore, more reliable outcome measures were available from early 2021 onwards. Second, external knowledge and guidance regarding severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and COVID-19 evolved rapidly during 2020, with considerable ambiguity and drastic differences in understanding and compliance across facilities during this time. For instance, White et al. (2021, p. 201) noted much anecdotal discussion among nursing home administrators regarding the challenges, early in the pandemic, of navigating frequent changes in regulations and guidance from multiple local, state, and federal agencies, which at times was “not only confusing but contradictory” (see also the study by Jones et al., 2021; Spear et al., 2021). This early ambiguity introduces an exogenous source of variation in pandemic responses across facilities; this variation is difficult to control, but it can be limited by selecting a later start period for the study’s analyses. Third, detailed reporting of several data elements that are essential controls in this study’s analysis began in March 2021. Thus, the study’s analysis starts at this point. Nonetheless, the study’s main predictor variables, which track accumulated experience with COVID-19 cases, take advantage of lagged data from prior weeks (with some models using information from nearly all earlier periods since the CDC began reporting data). As a result, although outcomes are observed beginning in March 2021, the study’s analysis accounts for learning that occurred well before this initial observation period, with minimal data loss.
The data were accessed in January 2022 and include 41 weekly reporting periods from the week ending 21 March 2021, through the week ending 26 December 2021. There are approximately 15,600 nursing homes within the United States, with roughly 15,300 of these facilities reporting data through the CDC system. After accounting for missing data and occasional non-responders, this study’s data include an average of 14,219 facilities per week (with some entries and exits), yielding an overall panel dataset with 583,004 facility-week observations. Crucially, though, the study’s outcomes are observed during only those weeks in which a nursing home was inspected by regulatory agents; thus, the actual estimation dataset is much smaller (slight variation exists across models, but this estimation dataset includes 21,225 inspected facility-weeks, spread across an average of 518 inspected facilities during each of the 41 weeks). Heckman selection models account for endogeneity in the inspection selection process, as described further below. These selection models include a first-stage estimation of inspection likelihood using the overall facility panel, and a second-stage estimation of inspection outcomes using the smaller inspected facility panel.
Measures
Problems with focal and supportive routines (deficiencies in infection control routines and deficiencies in supplemental routines)
A substantial amount of research in the health care literature consistently highlights the central, focal role of infection control routines in governing nursing homes’ responses to COVID-19 infections during the pandemic (Li et al., 2020; Ouslander & Grabowski, 2020; Quigley et al., 2020; Rubano et al., 2022). Once the nature and transmission pathways of SARS-CoV-2 were increasingly recognized, nursing homes began learning about, testing, and implementing new initiatives, as well as refinements to existing routines designed to manage and prevent COVID-19 infections and associated outbreaks (Quigley et al., 2020; Rutten et al., 2020). These changes took a variety of forms. For instance, many facilities became aware of the need to minimize contact among residents and with staff and to isolate infected residents where possible (Ouslander & Grabowski, 2020). Some homes even created cohorts or pods, grouping residents together to stop any outbreaks from spreading more widely across the entire facility (Rubano et al., 2022). Nursing homes could also develop or update formal infection control plans, including contingency planning for staff illnesses or other workforce issues, and facilities were encouraged to designate a central contact or qualified staff member to oversee these planning efforts (McGarry et al., 2020; Ouslander & Grabowski, 2020). In addition, a wide variety of other changes were also directly germane to infection control in this setting, such as performing COVID-19 testing on residents and staff as required, conducting contact tracing when possible, reporting infection data to residents and families, and limiting visitation and facility access as needed (Quigley et al., 2020).
To examine these and other efforts, state inspection teams conducted periodic site visits at each facility in accordance with CMS guidelines. These inspections covered infection control routines, and by the start of this study’s analysis window, inspections covering other supplemental or ancillary aspects of facility quality (which were temporarily suspended during the pandemic’s early stages) were also reintroduced. This study uses two different dependent variables, each derived from the results of these inspections. In each case, the variables are based on inspection teams’ assessments of problems (i.e., deficiencies) with relevant routines. These assessments were derived through detailed examination during unannounced site visits, which typically included direct observations of facility routines and procedures by inspection teams as well as medical record reviews, interviews with facility staff and residents (and family members, in some cases), and the additional involvement of various medical experts such as pharmacists and internists on inspection teams where relevant. When procedural deviations from federal requirements or other standards of care were identified, they resulted in deficiencies levied against the facility.
The first dependent variable (infection control deficiencies), a measure of problems with focal routines, tracks the number of problems or deficiencies with infection control routines, as identified during these inspections. Consistent with the study’s theory, which distinguishes between focal routines (with a direct impact on a certain area of activity) and supportive routines (with a widespread impact across areas of activity), this variable tracks issues with routines that are directly and centrally connected with controlling the spread or transmission of viruses and other pathogens such as SARS-CoV-2, the virus which causes COVID-19. These deficiencies could include, for instance, failures to implement or conduct appropriate infection control and infection-prevention protocols and procedures, failures to provide adequate oversight for infection control efforts, failures to develop and follow appropriate vaccination and testing policies, and failures to collect and report COVID-19 data to residents and families, among other lapses.
Also keeping with the study’s theoretical distinction between focal and supportive routines, the study’s second dependent variable (supplemental deficiencies) tracks issues with routines that exert a broader or more distributed impact across multiple domains of organizational activity within these facilities. These routines may indirectly support or enhance the facility’s ability to prevent or mitigate COVID-19 outbreaks, either by helping the facility to draw in resources from elsewhere (e.g., deficiencies could involve failures to establish or maintain relevant contractual arrangements with hospitals and other service providers) or through freeing resources and attention by alleviating quality problems in other areas (e.g., deficiencies could involve failures to meet safety or livability standards, prevent medication errors, provide appropriate care for therapeutic and behavioral needs, or offer adequate meals and nutrition, for example). However, in each case, the involved routines also influence or impact the nursing home’s quality of care in other domains outside of infection control. For instance, failures in contractual arrangements with hospitals could translate into problems with providing or obtaining effective or timely care for residents with a wide variety of medical issues or complications, as could other deficiencies in safety standards, medication administration, behavioral care, or nutrition management. Thus, in each case, these routines have a more distributed impact than focal routines that centrally involve infection control or COVID responsiveness, and the associated measure of supplemental deficiencies tracks the number of problems or deficiencies that involve these broader routines associated with facility quality across multiple domains.
The first dependent variable is used to test the study’s predictions regarding focal routines. The second dependent variable is used to test the predictions regarding supportive routines. Since these variables are only measured during the weeks that any given facility is inspected, and since these inspections are potentially non-random, the analyses incorporate a correction for this endogenous selection process, as described further below.
COVID-19 experience volume
Experience volume is measured through a cumulative index of prior COVID-19 infections among facility residents. The study focuses on COVID-19 case volume given that these infections presented unique learning opportunities for caregivers within the nursing home setting. From an early point in the pandemic, it was widely recognized that COVID-19 has a “nonspecific and atypical presentation . . . within the nursing home population” (Ouslander & Grabowski, 2020, p. 2156), that nursing home residents may not have typical symptoms of the disease, and that the disease “acts differently in older adults compared to younger adults” (Rutten et al., 2020, p. 1791). Given these distinctions, localized experience with infected residents within nursing homes was known to directly shape how facility staff learned about the disease and about the routines used to manage and control infections and outbreaks within these unique settings. For instance, with greater case experience, facilities increasingly recognized the need for a “high index of suspicion and low threshold for isolation of residents with almost any acute change of condition” (Ouslander & Grabowski, 2020, p. 2156), as well as the need to screen asymptomatic residents with heightened vigilance, to quarantine or cohort patients transferred into the facility from hospitals or other care settings, and to pay attention for unusual symptoms such as delirium and falls within this unique population (Rutten et al., 2020).
In addition, greater case experience gave nursing homes more opportunities to identify, understand, and test their infection control routines and to continuously tweak and adapt their approaches to suit each facility’s specific characteristics and constraints. Research points to substantial learning opportunities in this setting, as a lack of knowledge about infection control routines presented a significant barrier to their adoption and efficacy (Spear et al., 2021). As some have noted, misunderstandings about “key infection control concepts such as cohorting, isolation, bacterial colonization versus clinical infection, and proper PPE use have been documented among nursing home staff,” with much associated learning occurring through greater hands-on experience involving infected residents and outbreak management (Rubano et al., 2022, p. 54). Collectively, increasing COVID-19 case experience motivated facilities to seek knowledge about changes and refinements to infection control routines and procedures and afforded greater opportunities to learn by trial and error as these protocols were iteratively adapted to suit the specifics of a nursing home’s unique resident population, facility layout, and other constraints (Rubano et al., 2022; Spear et al., 2021; White et al., 2021). For these reasons, the study uses resident COVID-19 infections to construct its experience measures.
Experience volume, using these infections, was constructed in a manner that is directly consistent with other empirical research on learning (Darr et al., 1995; Haunschild & Sullivan, 2002; Musaji et al., 2020). This literature recognizes that the effects of past experience accumulate over time, but also that more distant experience may depreciate or become forgotten (Darr et al., 1995; Thompson, 2007). The general salience of the COVID-19 pandemic (and the study’s weekly observations, given that little knowledge may be lost from one week to the next) suggests a relatively long accumulation window. Accordingly, experience was accumulated and tested over a range of 15 weeks (a short but still reasonably lengthy window) to 35 weeks (a longer window that uses nearly all available historical data prior to the first observation period).
Tests were also conducted to compare experience measures depreciated linearly by age (since older events may exert weaker influence) against experience measures without this age-based weighting (Haunschild & Sullivan, 2002). Research in this domain suggests using model fitness to determine which of these experience measures are most explanatory (Darr et al., 1995; Haunschild & Sullivan, 2002; Srinivasan et al., 2007; Wiersma, 2007). In these tests, age-weighted measures were consistently more explanatory than unweighted experience, which is reasonable to expect since recent COVID-19 cases are likely more salient and influential than much older cases. Thus, final models use age-weighted experience measures. These tests also revealed that experience accumulated over a relatively long lag (35 weeks) was more explanatory in models estimating the study’s first outcome (infection control deficiencies). This longer window makes sense given the potentially enduring impact of nursing home outbreaks on infection control routines, and when combined with the age weighting, this approach accounts for a long history of experience but also realistically allows older events within this window to exert a weaker influence. Nonetheless, final models are presented for each tested version of the experience window (15, 25, and 35 weeks), and results are interpreted conservatively across all these models for each outcome.
COVID-19 experience concurrence
According to the study’s theory, increasing concurrence reflects a tighter clustering or overlapping of experience (in this case, resident COVID-19 infections) within particular segments of a broader timeline, as compared to a smoother or more even distribution of these events across that entire period. Thus, an ideal measure would take higher values when more cases occurred during the same week(s), and lower values when these experiences were instead spread more evenly across the entire multi-week window used to accumulate experience volume. This notion of concurrence is supported in the study’s setting, as some nursing homes experienced tightly clustered cases or significant outbreaks within a short period of time, while other nursing homes found that infections tended to emerge in a less-compressed fashion as the pandemic unfolded (Hochman, 2020; Maxouris, 2021).
This study uses a Herfindahl index to track these differences, since this index has the desirable property of taking higher values when items (i.e., infections) exhibit greater overlap or simultaneity within a smaller subset of categories (i.e., weeks) and lower values when these items are more evenly distributed across all available categories (Harrison & Klein, 2007; Haunschild & Sullivan, 2002). The index was constructed by first calculating the proportion of overall cases that occurred within each specific week during the trailing experience period, squaring each of these weekly proportions, and then summing these proportions across all weeks in the trailing window. The index used in each model is comparable to the respective experience volume measure, in that it is also constructed over the same timeframe (15, 25, or 35 weeks), and each weekly proportion is also depreciated linearly by age prior to the summation. The index is set to zero when no COVID-19 cases occurred over the trailing window (i.e., when the experience volume measure is also zero), and its maximum possible value is one. Thus, to summarize, COVID-19 Experience Concurrence reflects the distribution of experience over time, and the measure takes higher values when more infections are clustered within fewer (or the same) weeks.
Control variables
Several controls are required to account for unique influences in this setting. First, the facility’s occupancy ratio (its ratio of residents to total beds) is used to control for capacity limitations. Analyses also include the mortality rate from causes outside of COVID-19, to address general differences in resident health across facilities. The number of staff with COVID-19 infections during the reporting week is also included, since these infections can impact staffing levels and care quality. The analyses also control for resident and staff influenza cases, as well as for the number of residents and staff with other (non-COVID, non-influenza) respiratory illnesses, since each of these could motivate or influence infection control efforts outside of the study’s theorized mechanisms.
Although facilities are not required to report specific staffing levels on a weekly basis, they are required to indicate whether they are experiencing a shortage in any particular staffing category. These shortages can directly affect infection control and supplemental efforts. Thus, a dichotomous control was included to track shortages in nursing staff, and another dichotomous control tracks shortages in clinical staff (shortages in other staffing areas, such as with nursing aides, were highly correlated with the included controls). An indicator is included to track whether the facility reports a shortage of respirators or face masks, key physical components required for infection control. Dichotomous controls are also included to reflect whether the facility requests assistance (from state or local government agencies) for staffing or personal protective equipment (PPE) shortages. These variables are not highly correlated with the direct controls for actual staffing or equipment shortages since facilities do not always request assistance (e.g., when shortages are temporary or self-limited), and also since facilities may request assistance for upcoming or anticipated shortages. Thus, these controls address a related but distinct set of constraints that could independently impact the facility’s infection control and supplemental efforts.
The analyses also control for the reporting period (i.e., week) to account for changes affecting all facilities over time. Finally, a control is also included for major changes in external guidance. Although several agencies regulate various aspects of nursing home operations and care, the CMS exerts especially significant influence since compliance with this agency’s guidance is often a condition of reimbursement (for services provided to residents insured through Medicare and Medicaid, two federal insurance programs overseen by this agency). CMS publicized several prospective or upcoming rules during the study window, but fewer rules were actually implemented during this timeframe due to delays, comment periods, and court injunctions. However, two notable CMS rule changes involving nursing homes were implemented during the study period. The first, implemented around 10 September 2021, broadened how facilities were allowed to conduct some of their testing around resident and staff COVID-19 outbreaks. The second, implemented on 12 November 2021, removed most restrictions on visitation and access to nursing homes. Thus, a categorical control was included to reflect these changes; the control is set to one when just the first policy was in effect (weeks ended 12 September 2021 through 7 November 2021), and it is set to two when both policies were simultaneously in effect (week ended 14 November 2021 through the end of the study period). All controls and predictor variables were lagged by 1 week to reduce the possibility of reverse causality.
Analysis
Both of the study’s outcome variables (deficiencies with infection control and supplemental routines) are measured through inspection results, with these inspections occurring sporadically throughout the study period. A nursing home may have zero deficiencies during a particular week because an inspection occurred and no problems were found, or because it was not inspected during that week. Most nursing homes were inspected between one and three times over the 41-week study period, although some facilities were inspected up to 14 times, and other facilities were not inspected at all during this period. Concerningly, these inspection-selection decisions are potentially non-random; for instance, regulators may inspect or more frequently reinspect facilities with prior deficiencies or higher case counts, or they may be selectively drawn to larger facilities or facilities with greater capacity. Thus, the potential exists for unobserved endogeneity involving the inspection-selection process and its association with facility capacity, available resources, or other organizational characteristics, and these possibilities can introduce systematic bias into the study’s findings if they are left unaddressed.
Therefore, the study’s models are estimated using Poisson regression with a Heckman correction for endogenous sample selection (using the heckpoisson command in Stata/SE 15.1). Unlike with standard Poisson models, this estimation approach does not require equidispersion (equal mean and variance in the outcome); thus, this approach is suitable for both of the study’s count outcome measures (Heckman, 1979; Wooldridge, 2002). In each model’s first stage, predictors and controls are included along with an instrument to estimate a nursing home’s likelihood of being inspected (these first stages include all available facility-week combinations over the 41-week study period, since each home is always at risk of inspection). These models use facility size (number of beds, scaled by hundreds) as an instrument, for several reasons. First, larger facilities are inspected more frequently, due in part to their increased visibility as well as their higher resident volumes. Second, facility size does not necessarily affect care quality or lead to (or prevent) deficiencies in routines. Larger facilities may hire more staff to meet their increased capacity, or they may fail to maintain adequate levels and encounter staffing shortages as a result (White et al., 2021; Xu et al., 2020). While staffing shortages are well known to affect care outcomes, staffing ratios can be adjusted independently of facility size, and larger facilities do not necessarily perform better or worse on their own (Maxouris, 2021; McGarry et al., 2020, 2021). Thus, facility size meets the relevance and exogeneity conditions for a valid instrument (Wooldridge, 2002). A breakdown of the number of facilities within various bed count categories is included here, to provide additional information about the distribution of facility sizes in this setting.
Each model’s second stage adjusts for inspection selection using information from the first stage, and these second stages estimate the number of deficiencies (in either infection control or supplemental routines, depending on the outcome) for facility-weeks where inspections occurred. Fixed effects are unavailable with Poisson models using Heckman corrections; however, since the analyses pool multiple observations for the same facilities over time, robust standard errors are used to account for autocorrelation in the error term (Wooldridge, 2002). Finally, note that these models correct for selection in their second stage using a full information maximum likelihood (FIML) estimator; this approach does not require or allow the inclusion of a separate inverse Mills ratio variable to make this selection adjustment (see the articles by StataCorp, 2017; Terza, 1998).
Results
Table 1 reports descriptive statistics and correlations among the study’s variables. Correlations among each of the experience volume measures are naturally high since these variables use overlapping historical information, and correlations among each of the concurrence measures are also high for the same reasons. These respective constructions are never entered simultaneously within the same model. None of the other correlations raise any particular concerns regarding collinearity. Variance inflation factors were examined, and all were well below acceptable thresholds.
Descriptive statistics and correlations.

Note: n = 21,183.
As previously described, the study’s findings are estimated using two-stage models. Table 2 presents a sample of first-stage estimates of inspection likelihood, and Tables 3 and 4 present all second-stage estimates of inspection results (Table 3 presents estimates of infection control deficiencies, and Table 4 presents estimates of supplemental deficiencies). Beginning with Table 2, the first model corresponds with the control model from Table 3 (Model 1), and the second model corresponds with the control model from Table 4 (Model 1). Here in Table 2, positive coefficient estimates indicate an increased likelihood of inspection, and negative coefficient estimates indicate a reduced likelihood. The results of these first-stage estimates are not specifically interpreted, except to note that the coefficient of the instrument (facility beds) is uniformly positive and highly significant. This conforms to the expectation that larger facilities have a higher chance of being inspected, and the coefficient’s statistical significance is important to establishing the instrument’s relevance. To conserve space, Table 2 does not display the first stages from other models in Tables 3 and 4; however, all first stages were examined, and the instrument’s coefficient estimate is always positive and significant (always p < .05, often p < .001).
Poisson regression with endogenous selection and robust standard errors: First-stage (selection) models of inspection occurrence.

Note: n = 583,004 (21,225 selected, 561,779 non-selected). Std. errors in parentheses. External Policy Change = 0 (prior to test freq. & access changes) used as baseline category.
p < .10; *p < .05; **p < .01; ***p < .001.
Poisson regression with endogenous selection and robust standard errors: Second-stage models of infection control deficiencies.
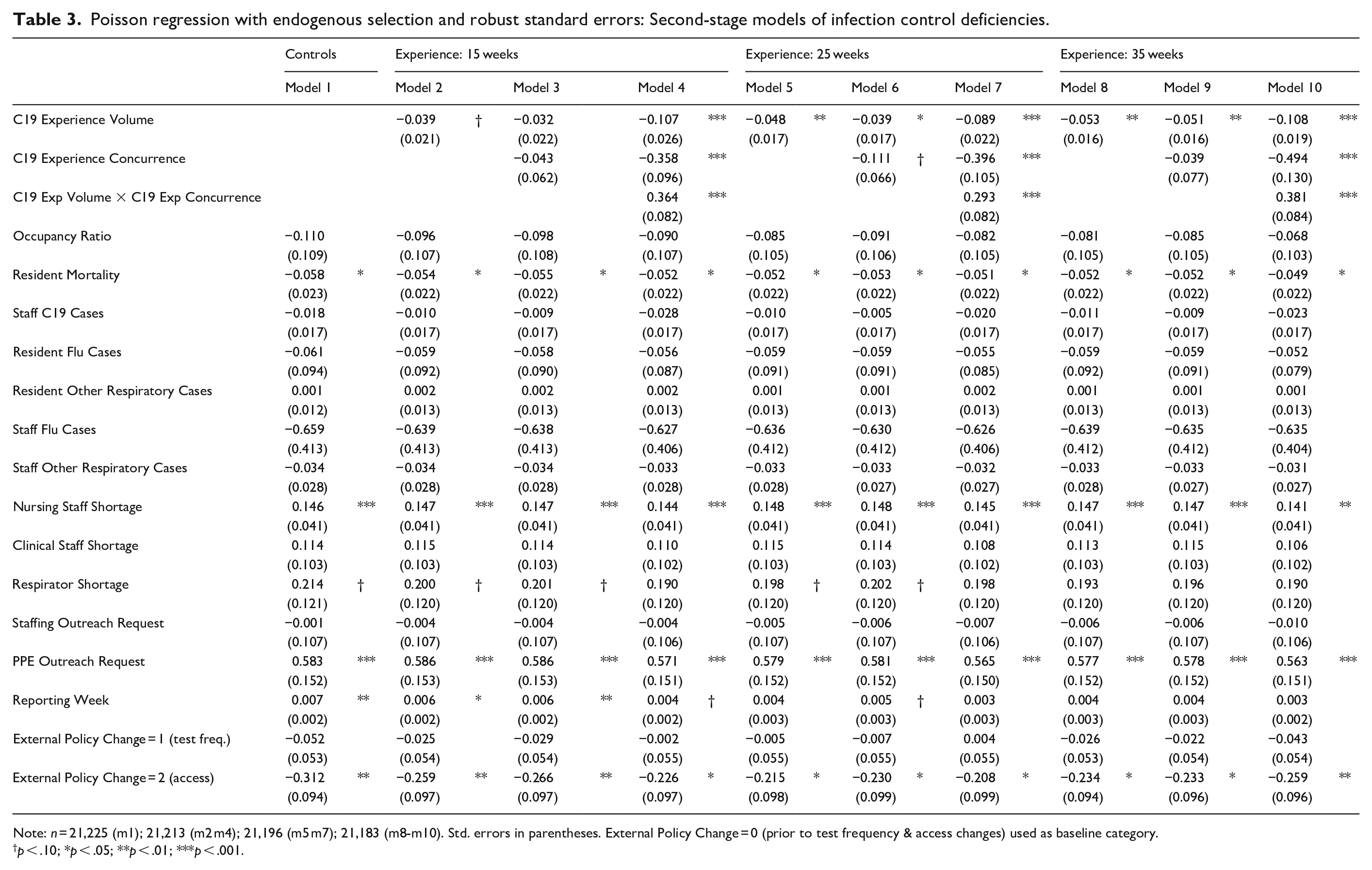
Note: n = 21,225 (m1); 21,213 (m2 m4); 21,196 (m5 m7); 21,183 (m8-m10). Std. errors in parentheses. External Policy Change = 0 (prior to test frequency & access changes) used as baseline category.
p < .10; *p < .05; **p < .01; ***p < .001.
Poisson regression with endogenous selection and robust standard errors: Second-stage models of supplemental deficiencies.

Note: n = 21,225 (m1); 21,213 (m2 m4); 21,196 (m5 m7); 21,183 (m8-m10). Std. errors in parentheses. External Policy Change = 0 (prior to test frequency & access changes) used as baseline category.
p < .10; *p < .05; **p < .01; ***p < .001.
Table 3 presents second-stage estimates of infection control deficiencies, used to test Hypotheses 1 and 2 about problems with focal routines. Model 1 includes only controls. Models 2 through 4 present results using experience (volume and concurrence) over the prior 15 weeks. The coefficient of experience volume is negative but non-significant when it is introduced in Model 2, as well as when concurrence is added in Model 3. This pattern could reflect unobserved heterogeneity in the effects of volume, where volume may lead to equivocal results until its interaction with concurrence is also considered. Indeed, this coefficient becomes significant in Model 4, when that interaction is included. This provides support for Hypothesis 1; the negative coefficient suggests that volume (at low levels of concurrence) will lead to a reduction in infection control deficiencies, consistent with the notion that nursing homes learn from their experiences in ways that benefit these routines. Furthermore, the interaction term’s coefficient is positive and significant in this model, suggesting that the direct relationship with experience volume will become less steeply negative when that experience arrives in an increasingly concurrent pattern. This provides support for Hypothesis 2.
Models 5 through 7 replicate this analysis with experience accumulated over 25 weeks, and models 8 through 10 use experience accumulated over 35 weeks. Results are identical, except that the coefficient of experience volume remains significantly negative in all models once these longer histories are considered, which provides continued support for Hypothesis 1. Again, the interaction term’s coefficients are significantly positive (in models 7 and 10). Collectively, this pattern of findings provides strong support for Hypothesis 2. In this setting, greater experience appears associated with fewer problems on focal routines, but the relationship weakens (becomes less negative) when that experience arrives in an increasingly concurrent fashion.
Table 4 presents second-stage estimates of supplemental deficiencies, used to test Hypotheses 3 and 4 about problems with supportive routines. Models are nested similarly; Model 1 includes only controls, and the subsequent models provide tests using experience over 15, 25, and 35 weeks. The coefficient of experience volume is negative and significant across all models, suggesting that greater experience leads to fewer deficiencies involving supplemental routines. This is consistent with the study’s theory regarding this learning relationship, and the pattern provides support for Hypothesis 3. Examining the interaction with concurrence, the interaction term’s coefficient is negative and highly significant when considering experience accumulated over 15 weeks (Model 4), negative and significant for 25 weeks of experience (Model 7), and negative but not significant for 35 weeks of experience (Model 10). Thus, at least over relatively shorter or moderate histories, experience appears associated with even fewer deficiencies on supplemental routines when it arrives concurrently. However, the effect does not appear to hold when experience is accumulated over a longer timeframe. Although preliminary tests suggested that a shorter experience window (15 weeks) was most explanatory for models estimating this particular outcome, the results here are interpreted collectively and conservatively to indicate partial support for Hypothesis 4. In this setting, greater experience appears associated with fewer problems on supportive routines, and some models suggest that the relationship intensifies (becomes even more negative) when that experience arrives in an increasingly concurrent fashion.
To facilitate interpretation of the study’s moderating hypotheses (Hypotheses 2 and 4), several figures plot the study’s estimates as well as their average marginal effects to test differences in slopes across the moderations. These figures use experience over 35 weeks when estimating infection control deficiencies (Table 3, Model 10), and they use experience over 15 weeks when estimating supplemental deficiencies (Table 4, Model 4), since these were the experience-accumulation windows that maximized model fit in preliminary tests on each respective outcome. Figure 1(a) plots the predicted number of infection control deficiencies at various levels of experience volume and concurrence, using a range of one standard deviation around each variable’s mean except where constrained by zero. As seen in the figure, increases in experience lead to a lower number of infection control deficiencies when that experience is not very concurrent in timing. However, this slope becomes less negative (and even appears to turn slightly positive) when concurrence is high.
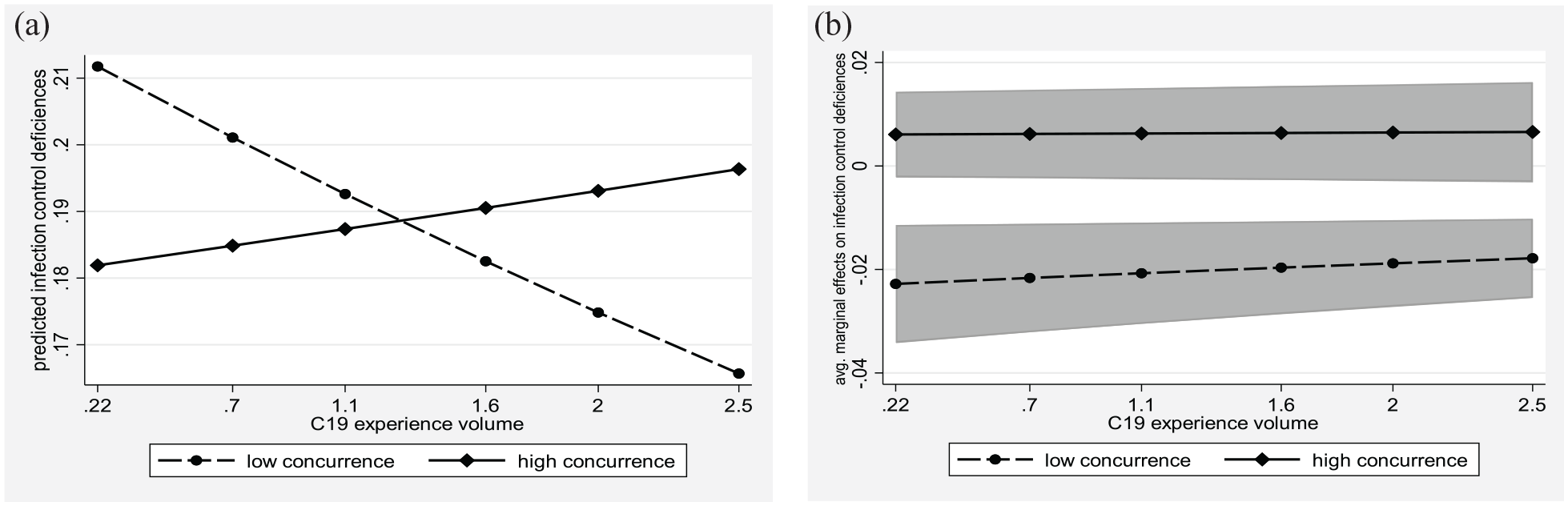
Figure 1(b) plots the average marginal effects (i.e., the slope effects) of these predictions and includes 95% confidence intervals around each plot in order to test slope differences. Negative values reflect a negative slope at a particular experience level (with reference to the slopes of each respective prediction in Figure 1(a)), and overlapping confidence intervals would indicate that changes in concurrence (from one standard deviation below to above its mean) do not lead to a significant change in the slope of experience at that particular volume level. As seen in the figure, the confidence intervals do not overlap, which suggests a significant moderation across the entire plotted range of experience volume. This result is consistent with Hypothesis 2.
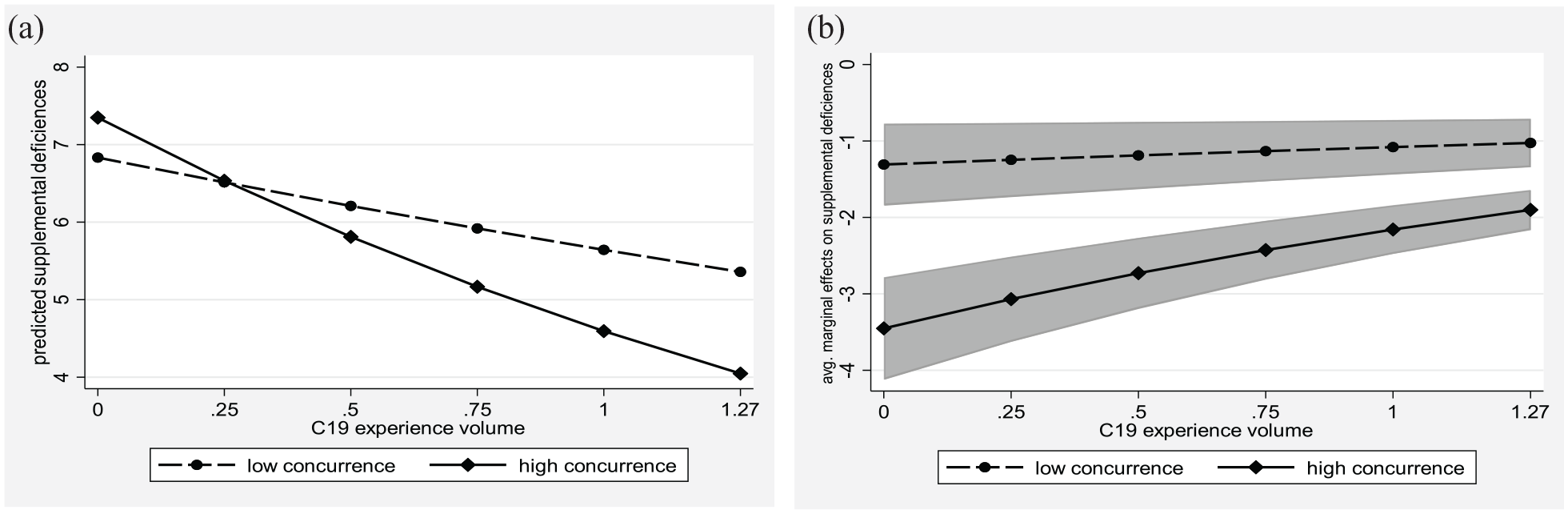
Figures 2(a) and (b) display similar plots for estimations of the study’s other outcome, supplemental deficiencies, from Model 4 in Table 4. As seen in Figure 2(a), increases in concurrence lead to a more negative effect of experience volume on this outcome measure. Figure 2(b) plots the respective marginal effects. Again, here, the confidence intervals around these effects do not overlap, which suggests that increases in concurrence lead to a significantly more negative effect across all levels of experience volume. This result supports Hypothesis 4. However, we recall that this hypothesis was only partially supported across other models from this study’s analysis.
Supplemental analyses
Several robustness checks and supplemental analyses were conducted to examine the stability of this study’s results. Some of these checks, such as the tests using experience across a range of accumulation windows, were previously described and integrated into the study’s main results due to their particular importance. However, a few other tests were also warranted. First, the study’s models are estimated using Poisson regression with a Heckman correction. This estimator relaxes the strict assumptions regarding overdispersion that affect standard Poisson models. Nonetheless, as a robustness check, the study’s models were each replicated using negative binomial regression with random effects, as the latter approach also accommodates overdispersion. Hypothesized results were identical in all cases, with the exception that the interaction between experience volume and concurrence became significant in the expected, negative direction in Table 4, Model 10, lending even greater support to the associated prediction. The stability of these results provides reassurance that the study’s findings are not unduly affected by overdispersion or other considerations in the choice between these estimators.
Next, the study uses a Herfindahl index to measure concurrence. This index ranges from zero to one and reflects the clustering or concurrence of infections within specific weeks (rather than their more even distribution across weeks). Thus, ideally, values of zero always reflect a perfectly smooth distribution of cases, and values of one always reflect perfect clustering of multiple cases. However, here, some zero values arise in situations where nursing homes had zero cases during the trailing period (since the index is set to zero in those situations), and some values of one arise in situations where nursing homes only had one case during the trailing period (since these situations result in a value of one when calculating the index). Two steps were taken to ensure that these special situations do not drive the study’s results. First, the study’s best-fit experience models (Table 3, Model 10, and Table 4, Model 4) were replicated while including a binary control to adjust for this impact; this control was set to one for observations where the focal nursing home had fewer than two infections during the relevant trailing window. Results were identical. Second, these models were also replicated when excluding these observations outright. This is a more conservative approach, but it discards a fair amount of potentially relevant information. Results for focal outcomes (compare with Table 3, Model 10) were identical. Results for supplemental outcomes (compare with Table 4, Model 4) were weaker and no longer statistically significant. Thus, there may be some limited concerns about the latter results when following a much more conservative approach to testing the study’s hypotheses, but the overall pattern across these tests was similar to that in the main analyses.
Discussion
This study proposes and finds differences in how organizations learn through experience, depending on how that experience is received. Specifically, the findings reveal that organizations learn less effectively on focal routines when their experiences are clustered together or overlapping, but partial support is also found for better learning under these conditions on the supplemental or ancillary routines that indirectly support a focal area of activity. These findings raise a number of theoretical and practical implications, as well as several limitations.
Theoretical and practical implications
This study raises several implications for organizational learning theory. First, there is growing recognition in this literature that the timing or pacing of experiences can affect whether and what organizations learn from them (Aguinis & Bakker, 2021; Eggers, 2012; Rahmandad & Gary, 2023). However, even in studies on frequent experiences, a common focus is still on events that unfold sequentially, allowing for at least some time in between iterations to engage in trial-and-error learning (Aguinis & Bakker, 2021; Desai & Madsen, 2022; Hayward, 2002). The present study extends this work by examining experiences that can overlap or become more concurrent, often requiring organizations to respond before the outcomes of prior actions are known (Fang, 2012; Rahmandad & Gary, 2023). These situations can create ambiguity about cause-and-effect relationships. The study develops a new theory about how this sort of ambiguity may influence and shape the learning process, and it uses this theory to articulate and predict how overlapping or concurrent experiences can affect learning outcomes involving different sets of routines.
Relatedly, the study also reconciles conflicting findings in prior research about how frequency can affect learning, since some studies have found that more frequent experiences can motivate learning out of necessity, while other studies have found that learning can instead be challenged by strain and other complications under these conditions (Aguinis & Bakker, 2021; Castellaneta & Zollo, 2015; Eggers, 2012; Musaji et al., 2020). Along these lines, the study draws from the RBV theory, and specifically from arguments about organizational capabilities and strain, and uses this theory to distinguish between focal routines in a specific area and supportive routines that span or involve other areas (Kahn et al., 2018; Raetze et al., 2021). The study uses this distinction to reconcile prior findings by suggesting that extremely frequent or overlapping experiences can challenge learning in a focal area, but that it can have broader benefits by leading to experimentation and better learning in supportive areas. To that end, the study also responds to calls for greater research on how learning could impact different routines in distinct ways (Argote et al., 2021; Argote & Guo, 2016; Becker, 2004).
It is also interesting to note that experience was found to accumulate over a shorter window for supplemental routines than for focal routines in this setting. Although this empirical finding was obtained through a preliminary specification test and was not specifically interpreted, it is intriguing to ponder whether the broader benefits of experience, for supportive routines, might often be more fleeting or transitory when compared with the more direct and enduring impact on focal routines. This seems sensible, and if it is indeed the case, the perspective could contribute to a learning theory by suggesting that time matters more for learning through experiences when those experiences are increasingly non-local or distant from a focal activity or outcome. Non-local effects are already recognized in some learning research, such as on explorative learning and boundary-spanning search (Levinthal & March, 1993; March, 1991), but that research typically does not consider time. The present study’s perspectives suggest new and interesting opportunities for integration across these streams (Bingham & Davis, 2012).
Finally, one of the study’s most important implications is practical in nature. The COVID-19 pandemic has caused unfathomable strain on individuals, communities, and organizations; yet, more generally, strain has always been all too familiar in many organizational settings throughout history (Castellaneta & Zollo, 2015; Roberts, 1990; Vogus & Rerup, 2018). This study suggests that members of organizations facing strain, such as the strain that could arise when many events and experiences begin to unfold concurrently or simultaneously, would do well to identify and review the ancillary routines, activities, and practices that indirectly support or supplement the overloaded area (Kahn et al., 2018). The study’s findings raise the possibility that broader learning can occur, and performance on those ancillary routines can be more readily enhanced, even when focal routines within the specific area are difficult to directly improve. The hope is that, by purposefully identifying ancillary but relevant targets for change, organizations might be able to reduce or recover from strain much more rapidly and effectively. For instance, managers in these and other settings would do well to identify and invest in routines with a broad or distributed impact across multiple areas of organizational activity, such as routines and guidelines for hiring and training, and procedures for securing resources or maintaining the organization’s supply chain or distribution network. These and other supplemental routines are often overlooked during times of crisis; yet, they provide essential support that could potentially facilitate the organization’s response (Ramanujam & Goodman, 2003; Roberts, 1990; Vogus & Rerup, 2018).
Limitations
Several limitations also impact our understanding of these results. First, measurement error could be introduced through contextual ambiguity in the distinction between focal and supportive routines. Great care was taken in this study’s theory to define and distinguish these constructs, and this theory draws heavily from research on organizational capabilities and strain and other topics, where these distinctions are already well established (Kahn et al., 2018; Raetze et al., 2021; Vogus & Rerup, 2018). Yet, even though a clear theoretical boundary exists between these constructs, this boundary may be fuzzier or difficult to discern within some empirical settings. If so, this could introduce error through incorrect coding or inaccurate classifications within those settings, and this might make it more difficult to accurately parse out the respective effects of the theorized predictors on either focal or supportive routines. This possibility is limited here given that infection control routines are explicitly disaggregated and evaluated separately from other routines by regulatory inspectors in this study’s context. Nonetheless, the limitation cannot entirely be excluded since focal and supportive routines could still potentially overlap in unexpected ways, such as if some smaller facilities in this setting interpret or execute these routines jointly or in a more blended fashion. Other settings with a more continuous boundary or more ambiguous distinction between these sets of routines may pose additional challenges, and further research on these constructs and their applications in various empirical settings would be beneficial.
Next, other limitations also exist, and many of these are specific to the study’s setting. Although the study controls for several relevant influences, the COVID-19 pandemic was an unprecedented shock within this and other settings, and organizational learning through experiences associated with the pandemic may differ from learning through other experiences in alternative settings. Indeed, from early in the pandemic, it was well recognized that the magnitude and scale of COVID-19 infections created previously unfathomable strain on most health care facilities, and the effects on nursing homes were particularly unique given their elderly and vulnerable resident populations (Ouslander & Grabowski, 2020; Rubano et al., 2022). Although this presents a novel context to study how organizations learned and coped during clustered, concurrent experiences, the possibility certainly exists that organizational learning will unfold differently in other less-challenging settings. Thus, future research in other settings could help to extend the study’s findings and limit these potentially idiosyncratic influences.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.