
Abstract
This study addresses the scarcity of research on health developments in the heterogeneous group of self-employed workers. It aims at understanding typical health progressions in this group and associations with demographic factors, work characteristics, and self-employment decisions. We investigate health profiles based on mental health problems, self-rated health, and work satisfaction, as well as transitions between them in relation to work effort, reward, overcommitment, demographic characteristics, and entrance and exit into self-employment. Using latent transition analysis, we analyzed data from the Swedish Longitudinal Occupational Survey of Health (SLOSH), including data from 593 participants. We identified four distinct, stable health profiles, revealing associations with work effort, reward, overcommitment, and self-employment decisions. No meaningful relations existed for demographic characteristics. Overall, the findings offer a comprehensive perspective on the health dynamics of self-employed individuals, their associations with work characteristics and decisions to enter and exit self-employment.
Despite being a smaller segment of the workforce (Ekonomifakta, 2023), self-employed workers make significant contributions to our society in terms of economic productivity, job opportunities, and innovation (Van Praag & Versloot, 2007). However, many workers who enter self-employment leave again, and this may have detrimental effects for the individual (Nikolova et al., 2021). Thus, a crucial area of research in the field of self-employment revolves around understanding the factors that influence individuals entering and exiting self-employment.
An important aspect of keeping a business running is the health of the self-employed worker, as research indicates that this is related to the success and survival of their businesses (Koch et al., 2021). It is well documented that—on average—self-employed workers experience better health compared to employed workers (Stephan, 2018). However, self-employed workers comprise a highly diverse group when it comes to who they are, how they work, and their health (Bernhard-Oettel et al., 2024). Furthermore, health is a complex construct, and depending on how health is assessed, results may vary (Stephan et al., 2023). Therefore, studying self-employed workers as one, homogeneous group and relying on averages from single aspects of health is insufficient to provide researchers, policymakers, and organizations with a comprehensive understanding of health development in this specific group of workers in relation to their demographic and work characteristics, and entrance and exit into self-employment.
Although there is existing research of entrance and exit of self-employment, few studies take a longitudinal approach with scientific rigor, following individuals in and out of self-employment, and even fewer examine the effects on various aspects of health (Gish, Lerner, et al., 2022). In this study, we aim to shed light on the development of health in relation to self-employment, demographic and work characteristics, and decisions to enter or exist self-employment. In doing so, we make several important contributions to the literature. First, since health may differ in the heterogeneous group of workers that enter, exit, or remain in self-employment over a period of 4 years, we will identify subgroups based on health profiles and study how workers change between these profiles over time. Furthermore, we aim to increase understanding for the link between health developments and decisions to enter, stay in, or exit self-employment, and therefore, we investigate how entrance into and exit out of self-employment affect health. In addition to this, we will also investigate how these developments associate with demographic and work characteristics. We study work characteristics through the lens of the effort reward imbalance (ERI) model (Siegrist et al., 1986), which explain the relationship between work and health by the efforts a worker put into work and the rewards received. If there is a balance, this is beneficial for worker’s health, whereas imbalances in work efforts and rewards constitute threats to health. This adds to both the theoretical understanding of the diversity in self-employment concerning health developments and decisions to start or remain in this employment form. The analysis of individual and work characteristics also provides insights of practical significance because it may help to identify vulnerable groups for which interventions may be needed to improve possibilities to set up and run businesses successfully.
Self-employment
Self-employed workers engage in an activity for their own account and are able to recruit their own employees (European Union Foundation, 2009). Over time, workers may change between employment forms—self-employment and organizational employment—or work in both, referred to as being a combiner (Bergman et al., 2021) or hybrid entrepreneur (Folta et al., 2010). Thus, it is important not to study only workers that are stably self-employed but also those who enter and exit self-employment. While self-employed workers are often referred to as entrepreneurs, it is a term that more accurately describes individuals who become self-employed due to having an idea or innovation but excludes those who enter self-employment out of necessity. Thus, for this study, we will use the term self-employed workers.
Self-employment grants freedom to organize work according to own preferences, affecting various aspects of work, including task selection, time scheduling, and skill development (Obschonka & Silbereisen, 2015). However, alongside the freedom that comes with self-employment, challenges such as potential income restrictions, blurred boundaries between work and personal life, lack of peer support, and responsibility for employees may arise (Stephan, 2018). One of the few studies focusing on various aspects of health in self-employed workers, indicate that self-employed workers experience both happiness and negative feelings, and more health problems than employed workers (Bencsik & Chuluun, 2021). Thus, the idea that self-employment has an entirely positive relationship with health does not seem to hold true, warranting a closer look into mental health of self-employed workers.
Self-employment and illbeing in terms of mental health problems
Mental health of self-employed workers has thus far most prevalently been studied through the absence of mental health problems such as stress, emotional exhaustion, depressive symptoms, and sleep disturbances (Stephan, 2018), which may be defined as illbeing.
Stress is a nonspecific perceived response to demands (Åkerstedt et al., 2015). Extant research shows that workers feel stressed when they experience work situations with an imbalance between perceived efforts put into work and rewards received (Siegrist et al., 1986). If this exposure is repeated, without allowing the worker recovery between stressful periods, stress can become a chronic experience. Consequently, the individual may suffer from health problems such as emotional exhaustion (Åkerstedt et al., 2016).
Emotional exhaustion is a state characterized by of profound fatigue and depletion, and a sense of being burned out (Melamed et al., 1992; Shirom, 1989; Shirom & Melamed, 2006). Emotional exhaustion is a serious and common problem in the work force. Studies suggest that self-employed workers may be particularly vulnerable to it, due to their unique work circumstances (McDowell et al., 2019). Furthermore, emotional exhaustion may drive intention to exit self-employment (Sardeshmukh et al., 2021).
Depressive symptoms are another common mental health problem in the working force. These encompass a broad range of emotional, cognitive, and physical symptoms, including feelings of sadness, low energy levels, lack of interest, and excessive worrying (Magnusson Hanson et al., 2014). It is important to note that emotional exhaustion and depressive symptoms can co-occur. Self-employed workers may be sensitive to depressive symptoms because they often lack the social support that organisationally employed workers benefit from and may have a tendency to internalize emotions due to stigma and fear of failure (Cubbon et al., 2021).
Stress, emotional exhaustion, and depressive symptoms are all connected to sleep disturbances, a common problem among workers, who often attribute poor sleep to factors at work (Linton et al., 2015). Stress arousal, worrying, and emotional depletion may all make sleep difficult. Sleep disturbances include difficulties falling asleep, restless sleep, and premature awakening (Nordin et al., 2013). Poor sleep has a negative, reciprocal relationship with mental health problems (Freeman et al., 2020). Sleep is one of the major means of recovering from stressors (Åkerstedt et al., 2016).
In sum, illbeing in terms of these mental health problems may have negative effects, both for the individual worker in terms of suffering, but also for society, since workers’ sick leave and income loss amounts to substantial economic costs and losses.
A more comprehensive view of health of workers engaging in self-employment
While health of self-employed workers has been studied with a focus on illbeing in terms of mental health problems (Stephan, 2018), a more comprehensive view on health also encompasses aspects of well-being (World Health Organization, 1958, 1984), and ratings of overall health, often called self-rated health (SRH; Jylhä, 2009).
Well-being may be defined as experiences of pleasure and happiness, and a striving for optimal psychological functioning and self-realization. Wiklund et al. (2019) highlight the central role of well-being in comprehending the health of self-employed individuals and show that self-employment is intricately linked to personal growth, performance, and fulfillment. In addition, experiences of well-being are beneficial for health and longevity, for example, when it comes to the cardiovascular, immune, and endocrine systems (Diener et al., 2018). Individuals experiencing well-being tend to live a healthier life and have better social relationships, have higher work performance, and contribute more to society in general (Diener et al., 2018).
With regard to work, well-being is often studied through work satisfaction. Work satisfaction is just one aspect of well-being, but it plays a crucial role in an individual’s overall well-being and quality of life (Cranny et al., 1992; Locke, 1969). A satisfying work experience is characterized by positive affect (Warr & Inceoglu, 2012). Generally, work satisfaction represents a relatively stable evaluation of one’s work, combining both cognitive appraisal and affective reactions derived from that appraisal.
In addition to feeling satisfied with one’s work, feeling healthy or satisfied with one’s health has also been conceptualized as an important domain of well-being by Diener et al. (1999). In other words, well-being relates to a person’s overall contentment, satisfaction, and a positive feeling about life in general or specific domains (Danna & Griffin, 1999).
In general, the relationship between well-being and health problems, social life, and work performance seem reciprocal. For example, well-being helps prevent health problems, but absence of health problems also generates well-being (Diener et al., 2018). However, an individual’s comprehensive health experience might not equal a simple equation in which positive and negative aspects of health problems or well-being can merely be added and subtracted. While the presence of both physical and mental illbeing has a negative relationship with the experience of well-being, individuals make overall subjective judgments concerning their health based on their own situation and its development over time. Thus, one cannot assume that individuals experiencing illbeing necessarily experience impaired well-being and health (Bujacz et al., 2020; Wikman et al., 2005). Hence, in addition to assessing illbeing and well-being, a more comprehensive understanding of an individual’s health experience can be derived by also assessing the individuals SRH.
In earlier research, health of self-employed workers has been operationalised as anything from pure mortality rates (Toivanen et al., 2016) to happiness (Bujacz et al., 2017), or self ratings of health (Bernhard-Oettel et al., 2024). Although these studies cover important health problems, aspects of well-being, or overall individual judgments concerning health, they do not take a comprehensive approach. This yields a lack of understanding of how illbeing, well-being, and SRH together contribute to an individual’s health. Thus, in our study, we will study health of self-employed workers through illbeing in terms of mental health problems, well-being in terms of work satisfaction, and more overall health in terms of SRH of self-employed workers.
Health of self-employed workers has often been studied in comparison to employed workers (Bergman et al., 2021; Gonçalves & Martins, 2018). In general, these studies find that, on average, self-employed workers are somewhat healthier and experience higher levels of well-being than their organisationally employed counterparts. However, it is also established by research that self-employed workers experience higher levels of work stress than employees (Stephan, 2018). Yet, many of these comparative studies have used cross-sectional designs, so that the development of health over time, both in those who are consistently self-employed, and those who switch between self-employment and organizational employment, is poorly understood. Furthermore, the paradox of high stress and high well-being highlights the complexity of health as a concept, and there is a need of a more comprehensive, long-term view of health in research of self-employed workers, taking their heterogeneity into regard.
Understanding the relationship between health and work
Work constitutes a significant aspect of individuals’ lives and can have profound effects on their health. Illbeing, particularly stress, often has roots in the workplace. The relationship between health and work can be understood through work-stress models such as the Job demands-resources model (JD-R; Bakker et al., 2004) or Effort-reward imbalance model (ERI; Siegrist et al., 1986). The JD-R model has dominated studies of self-employment, although it has been noted that JD-R may be too narrow to fully capture the experiences of work outside of the traditional organizational framework (Bernhard-Oettel et al., 2019; Bujacz et al., 2018; Stephan, 2018). Thus, ERI might be a more fruitful model when trying to understand the relationship between self-employed work and health.
ERI shifts the focus from resources and demands provided by organizations to the efforts individuals invest in their work, the rewards they receive in return, their tendencies to overcommit, and its impact on health (Siegrist, 1996; Siegrist et al., 1986; Siegrist et al., 2004). ERI postulates that employees invest effort in their work with the expectation of receiving rewards in return (Siegrist, 1996; Siegrist et al., 2004). Effort refers to the strain perceived by employees due to various job demands and responsibilities, such as interruptions, overtime, and obligations, while reward encompasses the opportunities provided by the job, including salary, esteem, job security, and career advancement. In ERI, a third component interacts with these two factors: overcommitment. Overcommitment refers to the tendency to respond to imbalance between effort and reward by excessively engaging in work and desiring control. Taking this together, the model rests upon the assumptions that an imbalance between high effort and low reward increases the risk of impaired health and that overcommitted employees are at greater risk of health deterioration (Siegrist, 1996; Siegrist et al., 2004). With these assumptions, the ERI model predicts workers’ health as a function of work circumstances and personal dispositions.
As we have argued, self-employed workers are not a homogeneous group, as previously assumed in many studies, and this heterogeneity extends to their work circumstances. The businesses of self-employed individuals vary greatly, ranging from solo entrepreneurs to owners of companies with hundreds of employees. They may face challenges or thrive, and their work hours can vary significantly. Consequently, the levels of effort and reward experienced by these workers vary greatly, and personal characteristics, such as overcommitment, further influence how these circumstances relate to their health (Siegrist & Li, 2016). In summary, ERI underscores the multifaceted nature of self-employment and its impact on health, highlighting the importance of a nuanced examination of entrepreneurial health profiles.
A person-centered approach to longitudinal developments of comprehensive health
In recent years, there has been a growing interest among researchers in examining the long-term health of self-employed workers. However, a key limitation of these studies is that they often treat workers engaging in self-employment as a homogeneous group, assuming they are the same (Arshi et al., 2021; Hessels et al., 2020; Sawang et al., 2020), or predefined subpopulations based on their demographics (Caliendo et al., 2023; Litsardopoulos et al., 2021), or career pattern (Koch et al., 2021). This means that the diversity in terms of health has not been studied in much detail longitudinally.
One approach to examining health diversity among self-employed workers is through person-centered methods, such as latent profile (LPA) and latent transition analysis (LTA). These methodologies have recently gained attention in research within the fields of work and organizational sciences. They enable the creation of parsimonious groupings of respondents that are both conceptually meaningful and methodologically valuable. While these methods are exploratory in nature, they should be guided by theory (Spurk et al., 2020).
Based on a couple of noteworthy studies focusing on well-being of self-employed workers, we argue that a person-centered approach may be fruitful to identify existing subgroups, each characterized by their distinct health profiles in the heterogeneous population of workers who enter, remain in or exit self-employment. Gish, Guedes, et al. (2022) studied self-employed and employed workers in two different samples. They based their profiles on well-being and personality, finding four profiles of varying well-being. In another study, Bujacz et al. (2020), studied only self-employed workers, and identified six distinct profiles based on well-being. These ranged from flourishing to unhappy. Both studies highlight the heterogeneity of well-being in self-employed workers. These studies show that profile analysis is a beneficial approach to assessing health in self-employed workers to understand differences in their health. However, they did not assess illbeing, nor development of well-being or health over time. Thus, insights of these aspects of health in self-employed workers are still lacking. While it is difficult to suggest the exact number and shape of subgroup profiles beforehand, based on earlier research, we expect at least one profile with good health on all or most aspects of health, one profile with mostly poor health, and one or more with different combinations of good and poor health. Furthermore, we expect that the profiles will be relatively stable over time (the same profiles occurring over time and a majority of workers staying in the same health profile over time) while change may occur for smaller groups. Our first research question therefore is:
RQ1. Which health profiles can be distinguished among workers who engage in self-employment, how prevalent are those profiles, and how do the workers transition between these profiles?
Health profiles over time in relation to work effort, reward, and overcommitment
ERI can provide a structured approach to understand the complex relationship between self-employed work and health and can thus be used to validate profiles of health. ERI’s unique perspective of extrinsic (effort and reward) and intrinsic (overcommitment) factors may provide an understanding of the interaction of work and health in ways that other work-stress models have yet failed to explain. Overcommitment might be particularly relevant when studying self-employed workers. They are at a higher risk of working excessively (Balducci et al., 2021) and often experience difficulties in detaching from work (Taris et al., 2008). Thus, ERI may be uniquely fit to study work stress in self-employed workers.
Indeed, many studies have confirmed the relationship between ERI and mental health problems in the general workforce (Håkansson et al., 2020; Harvey et al., 2017; Hinsch et al., 2019; Leineweber et al., 2020). Further research also indicates a relationship between ERI and work/life satisfaction (Braunheim et al., 2023; Ge et al., 2021; Kinman, 2016). Earlier research using ERI to understand work stress of self-employed workers is scarce. One exception is the study by Wolfe and Patel (2019), who used ERI to explain the positive relationship between stress and autonomy with imbalance in effort and reward, and especially overcommitment, leading to excessive work. In this study, we will use effort, reward, and overcommitment as separate factors to portray work-related factors, since the self-employed are known to be agentic and pro-active and invest a lot of effort into their business operations. To what extent they may compensate ERI through overcommitment is not well-known, but relevant if we seek to understand health developments yet better. However, the work-related factors should vary with health according to theory and thus validate the profiles. Thus, our second research question is:
RQ2. How is membership in health profiles at each time point related to effort, reward, and overcommitment?
Relationships of health and demographic characteristics of the worker
Many longitudinal studies include demographic characteristics as controls, and in these, results are contradictive. For example, Nguyen and Sawang (2016) found no meaningful relationship between health (in terms of mental health and work and life satisfaction), and gender, age, and educational level, but Dawson (2017) found that highly educated self-employed workers reported lower levels of work satisfaction than their less-educated counterparts. Finally, with a meta-analytic approach Solomon et al. (2022) found that higher education in self-employed workers leads to trade-offs, resulting in increased job stress and decreased job satisfaction.
With regard to gender, when analyzing the data for women and men separately, Litsardopoulos et al. (2021), found that women might face greater challenges when initially transitioning to self-employment, but over time, their health benefited from being self-employed more than was the case for men. Stephan, Li and Qu (2020) further add to this by showing that men experience health improvements when becoming self-employed, but women do not. These examples illustrate that the relationship between health of self-employed workers and demographic characteristics is complex and seems to vary depending on how health is assessed, which demographic characteristics are focused upon, and whether studies take longer time frames into account.
The varying results of previous studies highlight the need for longitudinal studies of these factors together and to study not only the prevalence of certain demographics in different profiles of health, but also if, and how, they predict changes between these profiles. This allows validation of the profiles as meaningful descriptions of qualitatively different groups, that cannot just be reduced to demographic differences.
RQ3a. Are demographic characteristics related to health profile membership?
RQ3b. Does demographic characteristics predict transitions between health profiles?
Health, entrance, and exit into self-employment
There is a growing body of research focused on the topic of entering into and exiting out of self-employment. However, the majority of these studies are cross-sectional in nature, primarily examining individuals’ intentions to enter or exit self-employment, without studying actual transitions. The cross-sectional research examining health, find for example that good health is related to intention to enter self-employment (Sweida & Sherman, 2020), whereas poor health has been linked to the intention to exit self-employment (Lindblom et al., 2020; Sardeshmukh et al., 2021).
Few longitudinal studies research the relationship of health and entrance and exit. With regard to entrance, in a study utilizing a quasi-experimental design, B. Nikolaev et al. (2020) found that health in terms of positive and negative affect, is related to entering self-employment. Their findings indicate that individuals who are organisationally employed and experience higher levels of negative affect are more inclined to transition into self-employment. Nikolova (2019) conducted a study tracking workers’ health before and after entering self-employment. The findings indicate that mental health improved for individuals after entering self-employment, while improvements in physical health were only observed among those who entered self-employment due to opportunity (in comparison to those who became self-employed out of necessity), even after controlling for changes in income, psychosocial factors, personality, and local unemployment conditions. Stephan, Li and Qu (2020) also studied mental and physical health, and found that those with poorer mental health self-selected into self-employment, and experienced a short-term improvement in mental health. In a similar study, focusing on well-being, Georgellis and Yusuf (2016) found that work satisfaction increased immediately after transitioning into self-employment but declined in subsequent years, potentially due to unmet expectations and the fading novelty of the new venture.
In terms of longitudinal studies of exiting self-employment, Nikolova et al. (2021) found that transitioning from self-employment to organizational employment was associated with modest improvements in health. Examining self-employment stability, Koch et al. (2021) discovered a positive relationship between stability in self-employment and better health. Furthermore, Bernhard-Oettel et al. (2019) investigated emotional exhaustion and psychosocial factors, revealing that individuals who transitioned from permanent organizational work to self-employment experienced reduced exhaustion and more favorable psychosocial factors. However, exiting self-employment and returning to permanent organizational work showed little to no change in these factors. These studies empathize the importance of considering the specific circumstances surrounding the transition and the need to study health more comprehensively.
RQ4. Does entrance or exit into self-employment predict transitions between health profiles beyond the previous profile membership?
Method
Participants
Since 2006, Statistics Sweden (SCB), on behalf of the Stress Research Institute, collects data for the Swedish Longitudinal Occupational Survey of Health (SLOSH), a national representative cohort study (Magnusson Hanson et al., 2018). SLOSH is a follow-up of the participants of the Swedish Work Environment Surveys (SWES) and comprises today all SWES participants 2003–2019 (n = 51,412). As SLOSH is based on the SWES, it can be regarded as approximately representative of the Swedish working labor market. All labor market sectors and occupations are represented, and the number of men and women is approximately equal. SLOSH was conducted every second year (since 2022 every year) by means of a pen-and-paper questionnaire in two versions; one for respondents who work at least 30% (which in Sweden generally is 12 h per week) and one for those who have left the working force, either permanently or temporarily.
This study is based on to the fifth to seventh data collection (hence forth called waves 1, 2, and 3) of SLOSH conducted in 2014, 2016, and 2018 (for information of attrition, see Magnusson Hanson et al., 2018). We selected those who were self-employed at least during one of the three waves (N = 2,327). This selection criteria were based on the fact that our study aimed at investigating self-employment entrance and exit and associations to health profiles, as well as profile change. As some of the respondents had not responded to all waves, we selected those who had answered at least one item in each of the six health constructs in two of the three waves, one of them having to be wave 2 (2,016; N = 593 participants). For information of missing on item level, see supplementary materials. This selection criteria were employed to achieve a valid health profile classification, which the entire study rests upon. The final sample size of 593 participants that was used in this study is well above the required sample size of 500 participants needed for the employed analytic techniques (Nylund-Gibson & Choi, 2018).
Assessment tools
We assessed health in terms of mental health problems, well-being, and general health, all responses given on Likert-type-scales. We assessed mental health problems in terms of stress, emotional exhaustion, depressive symptoms, and sleep disturbances. We assessed stress with three items, asking how the participants felt during the three preceding months (Åkerstedt et al., 2015). We used the revised 6-item subscale for emotional exhaustion and fatigue from the Shirom Melamed Burnout Questionnaire (SMBQ) to assess emotional exhaustion. The scale is deemed sufficient for describing emotional exhaustion in the general population (Shirom, 1989; Shirom & Melamed, 2006). We assessed depressive symptoms with the symptom checklist-core depression (SCL-CD6) including six items. SCL-CD6 uses a small number of depression core characteristics necessary for diagnosis so that the scores sum up to a meaningful severity assessment (Magnusson Hanson et al., 2014). Finally, we assessed sleep disturbances using a subscale of sleep disturbances from Karolinska Sleep Questionnaire (KSQ). KSQ was developed to describe subjective sleep and sleepiness in a general population (Åkerstedt et al., 2016; Kecklund & Åkerstedt, 1992). SCL-CD6, SMBQ, and KSQ have been tested and deemed fit to assess these constructs in self-employed workers (Bergman et al., 2021).
We assessed well-being, in terms of work satisfaction, with the item Roughly, how satisfied are you with your work?, and SRH general health with the item How would you rate your general state of health?
Demographic characteristics included information of gender (female = 0, male = 1), living conditions (married/cohabited = 0, living alone = 1; no children under 18 living at home = 0, children under 18 living at home = 1), education (up to university = 0, university = 1), age (55 or younger = 0, 56 or older = 1). The cut-off of age was based on the median age, as when dichotomisation is needed, this should be done as close to the median as possible, to avoid type I error (Chen et al., 2007). We coded entrance and exit to self-employment for each of the two transitions (from wave 1 to 2, and from 2 to 3), so that two variables were created: Entering self-employment (all other = 0, entering = 1), and exiting employment (all other = 0, exiting = 1).
To assess effort, reward, and overcommitment we used the scales developed by Siegrist et al. (1986). We revised the scale, excluding items that were not applicable for self-employed workers, keeping three items from each subscale.
All tables and figures noted with S can be found in Supplementary materials. Study items and factor loadings are presented in Tables S3 and S5, results from confirmatory factor analysis (CFA) in Tables S2 and S4, correlations Table S6, and reliability assessments in Tables S7 and S8.
Analysis strategy
We analyzed the data using LPA and LTA. These are person-centered analyses, aiming to identify subgroups of participants who share a similar profile of scores on the variables of interests (Morin et al., 2020). Thus, we were able to identify groups with distinct health profiles. First, we saved factor scores from measurement models of the health indicators and covariates to use in the analyses. These measurement models (tested with CFA) provided validity evidence of the scales assessing one, defined construct each. Second, to establish which profiles of health are present among self-employed workers, we ran LPAs for each wave; thus, following the analysis strategy described by Morin et al. (2020). Third, we tested profile similarity, which is equivalent to conducting analyses of longitudinal measurement invariance. This step also provided validity evidence for the profiles’ longitudinal similarity. Fourth, we followed with LTA, testing transitions between profiles over time. Fifth, utilizing a stepwise approach, so that the new variables would not affect the profile membership, we added demographic characteristics, entrance into and exiting out of self-employment as predictors of transitions above and beyond previous profile membership, and effort, reward, and overcommitment as covariates. Health in covariation with effort, reward, and overcommitment provided validity evidence for the hypothesized covariance in accordance with the ERI model. We conducted all these analyses in Mplus 8.6 (Muthén & Muthen, 2017). In addition, we used chi-square tests to test whether certain demographic characteristics were more prevalent in any of the health profiles. We conducted these analyses in R (R Core Team, 2019). More details about the process are presented in the supplementary materials.
Results
RQ1. Which health profiles can be distinguished among workers who engage in self-employment, how prevalent are those profiles, and how do the workers transition between these profiles?
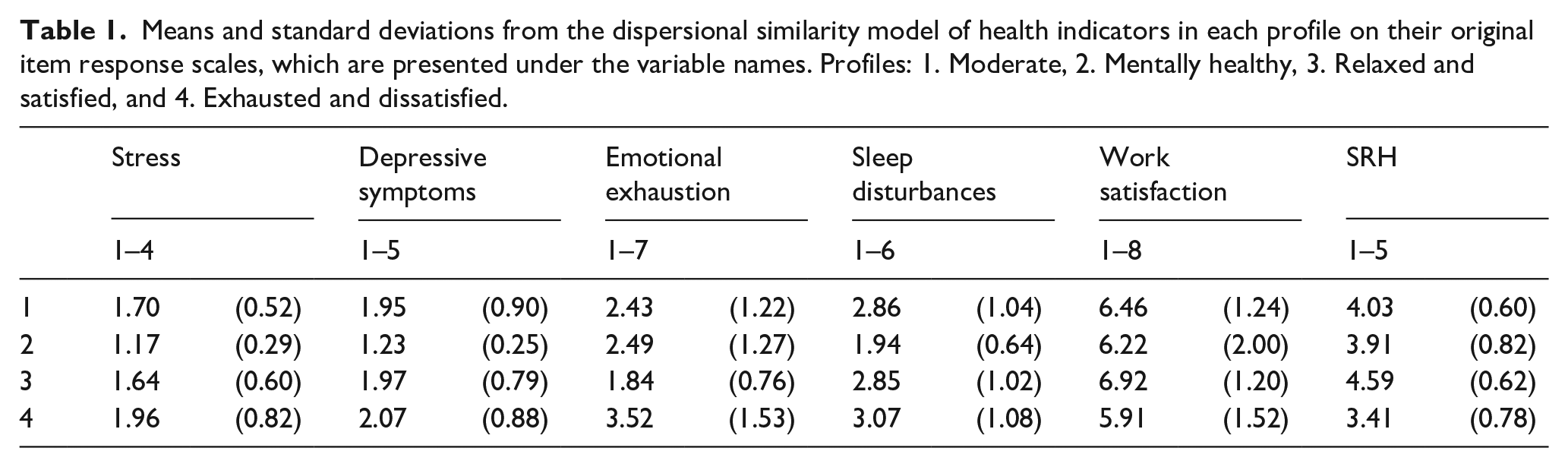
The analysis of measurement models revealed that the models fitted well in all three waves (Table S2–S5). Thus, the six indicators of health were used to form profiles at each wave. We chose the four-profile solution in all three waves, because it was supported both theoretically and empirically, as the found profiles were alike at each wave (Table S9). We named the profiles (1) Moderate profile (average on all health assessments), (2) Mentally healthy profile (few problems with mental health, sleep disturbances and stress, but below average general health and work satisfaction), (3) Relaxed and satisfied profile (very low experiences of exhaustion, and high general health and work satisfaction), and (4) Exhausted and dissatisfied (high exhaustion and low general health and work satisfaction; Figure 1 and Table 1).
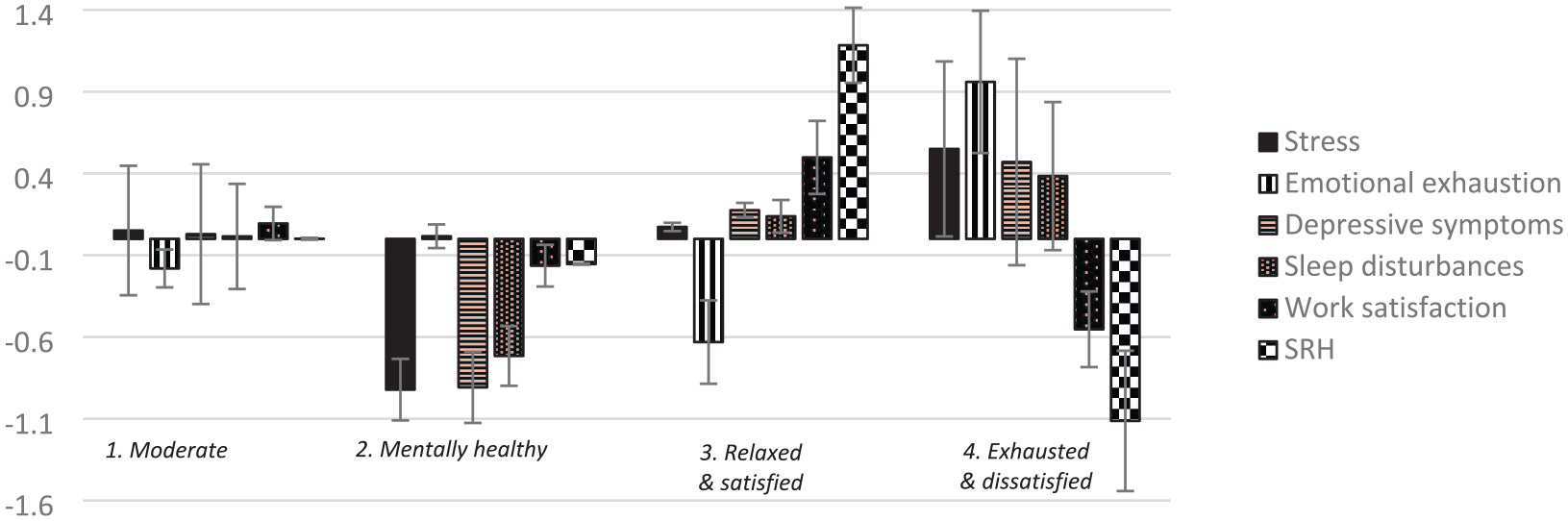
Final four-profile solution identified in the self-employed workers. Profile indicators are factor scores with mean of 0 and a standard deviation of 1 with 95% confidence intervals. Low scores on stress and exhaustion indicate good health, and high scores bad health. Low scores on all other constructs indicate bad health and low satisfaction, and high scores good health and high satisfaction. Estimates from the dispersional similarity model.
Means and standard deviations from the dispersional similarity model of health indicators in each profile on their original item response scales, which are presented under the variable names. Profiles: 1. Moderate, 2. Mentally healthy, 3. Relaxed and satisfied, and 4. Exhausted and dissatisfied.
The longitudinal design of the study allowed us to estimate the prevalence of profiles at each wave (Tables S10 and S11). The prevalence of all four profiles stayed similar over time. The model that specified transitions between waves 1 and 2, and between 2 and 3 as stationary had the best fit (Table S12), indicating that changes were stable over time. This model was used for the following analyses. The moderate profile was the largest at all time points, followed by the Relaxed and satisfied and the Exhausted and dissatisfied profiles, whereas the Mentally healthy profile was smallest. Transitions between profiles are represented by the percentage of self-employed workers who changed profile between waves (Figure 2, corresponding to Table S15). Most participants stayed in the same profile over time (61.6%–76.3%). Participants who changed profiles mostly moved from the Moderate to the Relaxed and satisfied profile (23.2%–28.7%), and from the Exhausted and dissatisfied to the Moderate profile (18.7%–26.5%). Few participants switched from the Relaxed and satisfied to the Exhausted and dissatisfied profile (1.9%–7.6%).
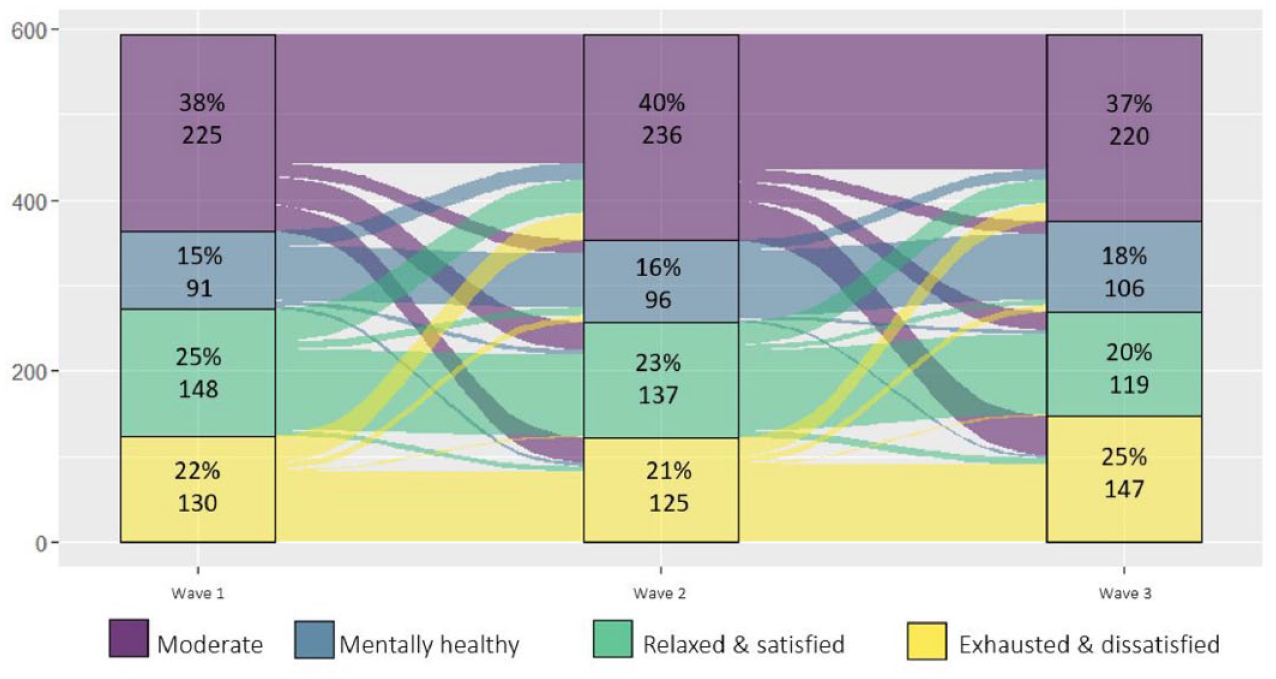
Latent transitions between profiles across waves. Profile membership from the dispersional similarity model.
RQ2. How is membership in health profiles at each time point related to effort, reward, and overcommitment?
The analysis of measurement models revealed that the models for effort, reward, and overcommitment fitted well in all three waves (Tables S4 and S5). The similarity model that restrained relationships to be the same over time had better fit than the free model (Table S17). Participants of the Moderate and Relaxed and satisfied profiles were distinguished by above average effort and reward, but below average overcommitment. For the participants of the Moderate profile, these estimates were around the overall mean, but for the ones in the Relaxed and satisfied profile, the pattern was more distinct. Participants of the Mentally healthy and the Exhausted and dissatisfied profile experienced low effort, low reward and high overcommitment. In the Mentally healthy profile, these experiences were around the sample mean; however, for the participants of the Exhausted and dissatisfied profile they more distinct (Figure 3, corresponding to Table S18).
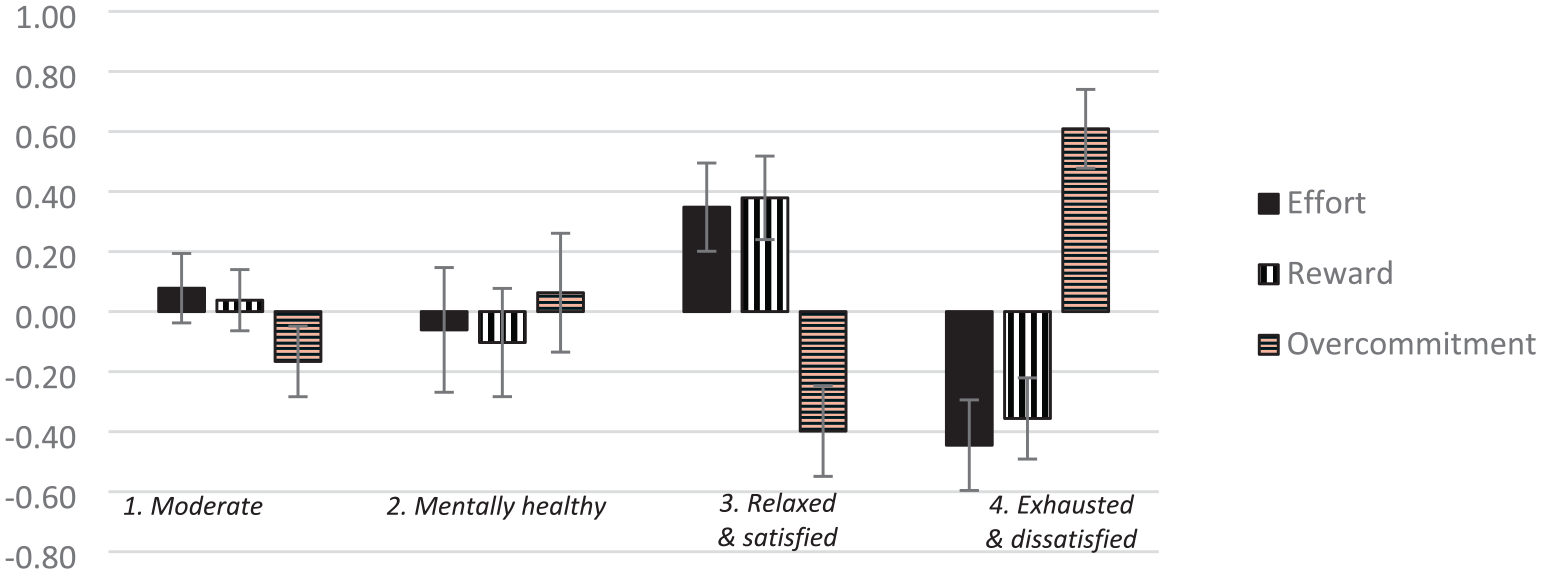
Effort, reward and overcommitment in self-employed workers. Based on factor scores with mean of 0 and a standard deviation of 1% and 95% confidence intervals. Estimates from the model assessing relationships of transitions and the three variables with relationships held similar over time. Low scores indicate low effort, low reward and low overcommitment, high scores indicate high effort, high reward and high overcommitment.
RQ3a. Are demographic characteristics related to health profile membership?
With a couple of exceptions, demographic characteristics were similar in all profiles over the three waves (for overall sample characteristics, see Table S16). There was a statistically significant difference in age between members of the Moderate (m = 55 years, 95% confidence interval [CI] = 54, 57) and Mentally health profiles (m = 51 years, 95% CI = 48, 53) during wave 1. Furthermore, statistically significant differences existed between the frequencies of educational level during wave 2 (χ2 = 8.3, df = 3, p = .04). Post hoc tests indicated that these statistical differences existed between the Moderate (54% went to university) and Exhausted and dissatisfied profiles (41% went to university; χ2 = 4.4, df = 1, p = .04), and the Relaxed and satisfied (59% went to university) and Exhausted and dissatisfied profiles (χ2 = 7.1, df = 1, p = > .01). In comparison, 55% of participants in the overall sample went to university.
RQ3b. Does demographic characteristics predict transitions between health profiles?
For the LTA, both the free and the similarity model that restrained relationships to be the same over time indicated that some demographic characteristics had a small, but statistically significant relationship with profile membership. The similarity model, which indicated better fit than the free model, demonstrated that self-employed workers who had higher education were slightly more likely to transfer to the Exhausted and dissatisfied profile than the others (Moderate profile: odds ratio [OR] = 1.25, 95% CI = 1.03–1.52, p = .02, Mentally healthy profile: OR = 1.28, 95% CI = 1.08–1.53, p = .01, Relaxed and satisfied profile: OR = 1.16, 95% CI = 1.01–1.35, p = .04). However, in the LTA, the null model had better fit than both the free and the similarity model, indicating that the demographic characteristics were not related to profile membership in a meaningful way (Table S13). Thus, we tested self-employment entrance and exit without controlling for these variables.
RQ4. Does entrance or exit into self-employment predict transitions between health profiles beyond the previous profile membership?
For entering and exiting self-employment, the similarity model that restrained relationships to be the same over time had best fit (Table S13), indicating that there were effects of entering and exiting self-employment, and that these were similar across waves. Most workers were continuously self-employed (w1 to w2: n = 231, 49%, w2 to w3: n = 260, 44%), and approximately as many entered (w1 to w2: n = 93, 16%, w2 to w3: n = 71, 12%) and exited self-employment (w1 to w2: n = 77, 13%, w2 to w3: n = 68, 11%).
Entrance into and exit out of self-employment predicted health profile membership in the coming wave above and beyond profile membership in the previous wave. Those that entered self-employment between waves were more likely to be members of the Relaxed and satisfied profile in comparison to the Exhausted and dissatisfied profile (OR = .31, 95% CI = .12–.81, p = .02). In a similar manner, those that exited self-employment were more likely to be members of all other profiles, compared to the Moderate profile (Mentally healthy profile: OR = 4.81, 95% CI = 1.19–19.43, p = .03, Relaxed and satisfied profile: OR = 7.14, 95% CI = 1.91–26.63, p = < .01, Exhausted and dissatisfied profile: OR = 4.84, 95% CI = 1.02–22.93, p = .05). See Figure 4, corresponding to Table S19. In other words, while the self-employed workers were most likely to stay in the same profile over time or change to a similar profile (hence making profile membership of the previous wave the strongest predictor of profile membership in the following wave), entrance into and exit out of self-employment predicted profile membership beyond this, indicating that entrance and exit are meaningful predictors of health in the following wave.
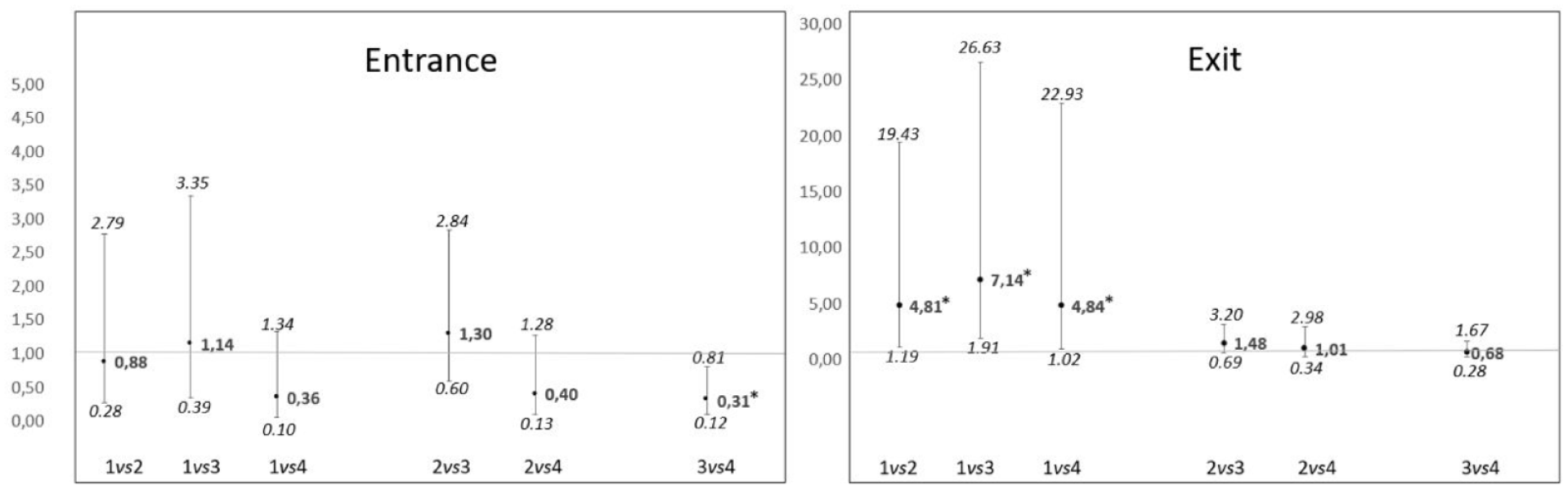
The probability of profile membership, depending on entrance into or exit from self-employment, odds ratio, and 95% confidence intervals. Values above 1 indicate a higher probability of profile membership after entrance/exit, above and beyond the effect of profile membership previous wave. Note that as the distribution of odds ratios is skewed, the CI are asymmetrical. Note that the scales are different for entrance and exit.
Discussion
With this article, we aimed to study the development of health in relation to self-employment, demographic and work characteristics, and decisions to enter or exist this employment form. Among the self-employed, we found four stable profiles of health, named the Moderate profile, Mentally healthy profile, Relaxed and satisfied profile, and Exhausted and dissatisfied profile. Most participants stayed in the same profile over time, and most changes involved transitions from or to the Moderate profile, which was also the largest one (RQ1). The Moderate and Relaxed and satisfied profiles had high effort, high reward, and low overcommitment, while the Mentally healthy and the Exhausted and dissatisfied profiles had low effort, low reward and high overcommitment. However, these results were only distinguished from the overall sample means (in terms of effect size and statistical significance) in the Relaxed and satisfied and Exhausted and dissatisfied profiles, and overcommitment in the Moderate profile (RQ2). The demographic characteristics had little influence on profile membership (RQ3a), or transitions between profiles between waves (RQ3b). However, entering or exiting self-employment had an effect. Entering self-employment made the worker more likely to end up in the Relaxed and satisfied than in the Exhausted and dissatisfied profile in the following wave, and exiting self-employment made workers more likely to end up in all other profiles, but not the Moderate profile (RQ4).
Our results in relation to theory and previous research
The health profiles were generally balanced, in the sense that they were either different kinds of healthy (Moderate, Mentally healthy, and Relaxed and satisfied), or unhealthy (Exhausted and dissatisfied). This is in line with research indicating that relationships between mental health problems, well-being, and general health is reciprocal (Diener et al., 2018). However, it is important to note that the three healthy profiles were not similar in their profile shape. Instead, they each were characterized by a distinct profile in health, which is in line with previous research (Bujacz et al., 2020; Gish, Guedes, et al., 2022). The three healthy profiles had meaningful differences in several remarks. Member of the Moderate profile experienced average health on all health assessments. What is important to note is that this group is moderate in comparison to the others, but with regard to their means on the original scale, this group should still be considered healthy, and should thus not be seen as they were in a “neutral” (i.e., in-between good and bad) health status. In studies using only means of all self-employed workers, this group, which is the largest of all four groups, would most likely drive the means, thus making it look like self-employed workers are healthier than organisationally employed workers. Here, our results help to reveal a more complex reality.
Members of the Mentally healthy profile experienced notably lower mental health problems in terms of stress, depressive symptoms and sleep disturbances, but their emotional exhaustion was on an average level. Interestingly, the mentally healthy profile had lower work satisfaction and general health than the other healthy groups. Members of this profile may thus be seen as the classic idea of a healthy person—in that they lack symptoms of mental health problems. However, they also seem to lack positive aspects of health, such as work satisfaction, that is present in the Relaxed and satisfied profile. The latter experienced considerably lower levels of exhaustion than the other groups, and considerably higher work satisfaction and general health.
The Exhausted and dissatisfied stuck out as the only truly unhealthy profile. Workers in this profile had noteworthy differences from member of the other profiles when it came to emotional exhaustion, work satisfaction, and SRH, with none of the 95% CI overlapping with the other profiles. Thus, workers in this group were highly likely to experience practically significant differences in health and its consequences compared to members of the other groups.
In sum, our results highlight the complexity of the concept of health and that it is not as easy as adding and subtracting positive and negative aspects. Our results further extent this earlier research because we show that the findings of cross-sectional studies by Bujacz et al. (2020) and Gish, Guedes, et al. (2022) indicating that there are different combinations of health also hold over time. We could also show that these health profiles are stable over time, and this is another novel and important contribution to the research field. Workers mostly stayed in the same profile over time, and second changed to a similar one. Regarding our first research question concerning the prevalence of typical health profiles and changes in between them over time, the results reveal that most workers who engage in self-employment are healthy—but in different ways. This is in line with previous research indicating that self-employed workers are generally healthy (Stephan, 2018), but we provide important nuance to this observation. Furthermore, their health is generally stable over time, meaning that those who are healthy tend to stay healthy, and those who are unhealthy stay unhealthy.
The health profiles were in coherence with the effort, reward, and overcommitment-model, in that the healthy profiles had either average effort, reward, and overcommitment, or high effort, high reward but low overcommitment, and the unhealthy profile Exhausted and dissatisfied had low reward, low effort, but high overcommitment (Siegrist, 1996; Siegrist et al., 1986; Siegrist et al., 2004). The profiles were also in line with previous research of health and work circumstances, including those using JD-R (Bernhard-Oettel et al., 2019; Bujacz et al., 2018) and ERI (Wolfe & Patel, 2019), as well as studies of excessive work (Balducci et al., 2021; Taris et al., 2008). Interestingly, and adding to these earlier findings, there was no profile with low effort and high reward. This might be due to self-employed workers deciding how much effort they want and can put into their work, and it may be related to their tendency to be engaged in their work (Mabunda Baluku et al., 2020). Furthermore, for self-employed workers, there might be a direct effect of effort on business success, that is not present for employed workers in the same way, meaning that the effort they put into their work more directly affects business survival. Low effort on the other hand was reported by the Exhausted and dissatisfied group and might indicate that the business of the self-employed worker is not going so well. In this group, it would be valuable to be able to trace developments back over longer time frames to better understand whether low effort and reward of presumably less profitable businesses resulted in emotional exhaustion and dissatisfaction. Another line of thinking may be that work situations characterized by high effort and low rewards lead to exhaustion and dissatisfaction, so that workers finally cut back on their efforts to at least in part reduce the existing imbalance.
To answer the second research question of the study about the relationship between health profiles and effort, reward, and overcommitment, health of workers engaging in self-employment is in line with the assumptions of the ERI model. What is more, with the necessary adjustments made in assessment, ERI seems to be a valuable framework to study workers engaging in self-employment and is one of the few theoretical frameworks that can depict the high investment that workers in this employment form often make (in form of effort and/or overcommitment).
Generally, we found few associations between demographic variables and the four identified health profiles as well as transitions between them. Gender and living conditions did not differ, and this may be surprising, since earlier research has identified health differences in self-employed women and men (Litsardopoulos et al., 2021; Stephan, Li & Qu, 2020), and having a partner has often been found to be positive for health and well-being because it may generate a source of social support (Diener et al., 1999). However, all studies, including ours, take on different analytical approaches, and include different assessments of health. Thus, it might be that differences found are dependent on approach. In our case, we found that gender does not influence health profile membership beyond previous profile membership, and thus, gender seems to be less important than previous health status, which was not tested in the other studies.
The two statistically significant differences that were identified were only found in one of the waves, thus, they were not consistent over time. This concerns the findings that members of the Moderate profile were slightly older on average (55 years) than those of the Mentally healthy (and the differences related to education showing that workers with lower education were more often in the Exhausted and dissatisfied 51 years), profile than in the Moderate and Relaxed and satisfied profiles, which might sound paradoxical, but is in line with previous research (Dawson, 2017), and might be explained by the fact that education often raises ambition (Clark & Oswald, 1996). Interestingly, those with higher education were more prone to switch to this unhealthy profile, which is in line with Solomon et al. (2022). This finding perhaps also illustrates the difficulty to find clear-cut demographic differences related to the health profiles, since at any wave, the health profiles contained both individuals whose health remained stable over time as well as some who transitioned to the health profile more temporarily. For example, in the unhealthy profile Exhausted and dissatisfied, there may be more individuals with lower education and thus lower labor market power, and perhaps more necessity-driven self-employment (Stephan, 2018). At the same time, highly educated self-employed workers transitioned into this profile, and thus, educational differences between health profiles were blurred. However, this also illustrates the complex reality of studying health and health developments in self-employment and the difficulties inherent in studies that only can capture momentary assessments.
The differences in demographic characteristics we found did not repeat over waves and had small effect sizes. In addition, the null model with no relationships between demographic characteristics and the profiles had the best fit. A possible interpretation of these results is that the statistically significant relationships between demographic variables and the profiles found at one time point arose by chance, or were too small to have practical significance. This would also be in line with the results of Nguyen and Sawang (2016). Thus, to answer RQ3a and RQ3b, we found no meaningful, stable relationships between profile membership, or transitions between them and demographic characteristics.
We found that workers who entered self-employment between waves were more likely to be in the Relaxed and satisfied profile than the Exhausted and dissatisfied. This is in line with several earlier studies (Bernhard-Oettel et al., 2019). Furthermore, and much in line with studies by Stephan, Li and Qu (2020), and Nikolaev et al. (2020), we found that health indeed seemed to develop in a positive direction, specifically with respect to reduced exhaustion and increased work satisfaction.
Regarding to workers who exit self-employment, we found that those who exited were more likely to transition to any health profile but the Moderate one, indicating that exiting self-employment leads to health that differs from the most common and average health profile of self-employed workers. This, at least party, parallels the study by Nikolova et al. (2021), who found that transitioning from self-employment to organizational employment was associated with modest improvements in health. Our study may also help to explain these earlier seemingly contradictory findings (Dawson, 2017; Nguyen & Sawang, 2016), as it reveals different types of health profiles seem related to different changes, underscoring the merits of a person-centered approach that highlights developments in distinct subgroups and not in the group as one entity. In addition, since this study portrays health in a more comprehensive way, our results can give further insights to better understand that health changes as a pattern, form different shapes, instead of simply changing in absolute levels on single variables as would be the case if values in single measures go up or down.
In conclusion, and to answer research question four, entrance and exit into self-employment have an effect on health of workers, providing important understanding to the consequences on health of self-employment.
Strengths, limitations, and future research
Like with all research, our study has strengths and limitations. The exploratory approach of LTA is a strength as there is very little previous research focusing more comprehensively on health, and health changes in self-employed workers over time. In addition, the method allowed us to find and indicate interesting interactions that we could not have foreseen. Using an exploratory analysis, in comparison to using a confirmatory analysis, facilitated particularly in mitigating type 1 errors, as it enables uncovering unforeseen interactions and avoid dealing with numerous hypotheses.
Corresponding to guidelines for LPA and LTA, our profiles are based on health indicators that are theoretically related but distinct, and ERI provides a theoretical explanation to the relationship between work and health (Spurk et al., 2020). A strength associated with the method is that we were able to test how previous health profile membership, demographic characteristics, and entrance and exit into self-employment affect following health profile membership. Finally, with regard to the exploratory nature of our study, is that it has weaknesses in the same way as all exploratory approaches have: it is more sensitive to data set discrepancies and results need to be confirmed with future studies. Future studies will have to take a confirmatory and more in-depth approach to the relationships and interactions found.
In contrast to other person-centered studies investigating the health of workers engaging in self-employment, our study is longitudinal. This provides the opportunity to understand changes and relationships over time. Furthermore, the use of LTA analysis works as test of measurement invariance, confirming the profiles are the same at all three waves. A further strength in the use of LTA is the process of using both qualitative and predefined quantitative judgments to decide the number of health profiles, taking background evidence, study design, data quality, and our understanding of underlying mechanisms into consideration (Amrhein et al., 2019; Cohen, 2016; Gelman & Stern, 2006). Finally, the longitudinal nature of the study allows repeated measures that confirm results from one wave to another.
Another strength lies in our rigorous testing of the health constructs stress, emotional exhaustion, and sleep disturbances and collection of validity evidence in accordance with APA standards (American Educational Research, 2014). To increase power, we exported factor scores from the CFAs we used into the LPA and LTA. While factor scores do not explicitly control for errors in assessment as latent variables do, they provide a partial control by giving more weight to reliable items and preserve the underlying assessment structure (Morin et al., 2020). Furthermore, we assessed two of our health assessments, work satisfaction and SRH, using single items. When a construct is sufficiently unidimensional and narrow, it can be assessed using a single item (Fayers & Sprangers, 2002; Wanous & Hudy, 2001). Also, overall health is a well-established concept (Benyamini & Idler, 1999; DeSalvo et al., 2006; Mossey & Shapiro, 1982) and an indicator of morbidity and mortality (Latham & Peek, 2013; Regidor et al., 2010). The validity and reliability of this item has been shown in various studies (Bailis et al., 2003; Benyamini & Idler, 1999).
In our study, we set out to study health comprehensively. We did so by including assessments of mental health problems, work satisfaction, and overall health. Future studies may benefit from focusing even more on the positive aspects of health, such as positive affect and eudaimonic well-being (Ryan & Deci, 2001; Stephan, Tavares, et al., 2020) to further differentiate between the healthy profiles of workers engaging in self-employed work.
We used the framework of ERI to understand the relationship between self-employed work and health, but it might be prolific to study this relationship from other perspectives as well, such as Self-determination theory (SDT; Deci et al., 2017) and coping (Lazarus & Folkman, 1984). SDT with its idea of satisfaction of basic psychological needs may be specifically well suited to study self-employed work, as this is a theory of human behavior and thus not a work environment theory developed for traditionally employed workers. Coping are thoughts and behaviors that the worker uses to manage stressful situations (Lazarus & Folkman, 1984). In a study of well-being, B. N. Nikolaev et al. (2023) suggest that coping strategies can be studied in combination, which aligns well with a person-centric approach and considering multiple health indicators simultaneously, thus providing nuanced interpretation of health profiles. Hence, we recommend studying health of self-employed workers from these perspectives in future research, and both of these frameworks may be added to the study of ERI as well.
In or study, we looked at experiences of business characteristics in terms of effort, reward, and overcommitment, but future studies may research the relationship between objective work characteristics, such as income, branch, and business success. Our focus was not to study why the workers exiting self-employment ended up in different profiles, this might find an explanation in objective work characteristics. For example, one likely reason for ending up healthy or not after having left self-employment might be related to why and how one left self-employment. If the business failed, but the worker did not want to exit self-employment, they may end up Exhausted and dissatisfied, or if the worker left voluntarily, they end up in the Mentally healthy or Relaxed and satisfied profile. Furthermore, we did not know the extent of the businesses of the workers; whether they are solely self-employed or combine self-employment with organizational employment. Future studies focusing on combiners in addition to solely self-employed are highly warranted (Nikolova et al., 2021). Thus, for future research, we suggest researching the relationship between different kinds of health and objective work characteristics, as well as its connection to entrance and exit into self-employment.
Finally, we suggest that future studies cross-validate the health profiles within specific groups of self-employed workers to explore potential shape or qualitative differences in profiles. For instance, researching the population of self-employed women or immigrants may yield profiles of health different from our results, which represent the entire population of self-employed workers across all demographic characteristics.
Conclusion and practical implications
Our study shows that health of workers engaging in self-employment is not as simple as just being healthy or unhealthy, but that illbeing and well-being are interrelated, and that SRH is related to these but not as a direct consequence of them, and such complexity of health has often been overlooked in research on self-employed work. Health of the self-employed workers was generally stable over time, but if workers changed health profiles, they were most likely to change to a similar one. Furthermore, effort, reward, and overcommitment provided understanding of how work and health may interact and validated the health profiles; displaying the merits of using ERI to understand the work situation of the self-employed and its association with health. We found that demographic characteristics had no meaningful relationship with health profiles of the self-employed workers. Furthermore, and maybe most interesting, we showed that entrance and exit into self-employment affect health changes above and beyond previous health profile membership. Those who entered self-employment were more likely to report positive health change, and those who left reported changes in all directions away from the Moderate health profile. Our results further advance understanding of the heterogenous group of self-employed workers and highlight in what way their differences may drive different health developments.
Finally, this study has a number of practical implications. Our results may inform policy makers, organisationally employed workers, and self-employed workers themselves that being self-employed is not exclusively related to good health. In addition, exiting self-employment may come at a price, or the opposite, it may be positive for the workers’ health development. Thus, our results provide these stakeholders with important information of the relationship between health and self-employment to consider when encouraging or taking the leap to because self-employed. Another implication of our findings is that health interventions for self-employed workers may need to target specific and may need to be tailor-made to the health-related problems experienced in these groups. Based on the fact that health and work factors, such as depicted in ERI, are related, targeting health profiles, or targeting work-related factors in interventions for self-employed workers may have beneficial effects to improve both the work situation and health, and may potentially have an impact on entry or exit decisions.
Supplemental Material
sj-docx-1-brq-10.1177_23409444241277831 – Supplemental material for Are you in or are you out? A longitudinal person-centered study of health and entrance and exit into self-employment
Supplemental material, sj-docx-1-brq-10.1177_23409444241277831 for Are you in or are you out? A longitudinal person-centered study of health and entrance and exit into self-employment by Louise E. Bergman, Aleksandra Bujacz, Constanze Leineweber, Susanna Toivanen and Claudia Bernhard-Oettel in BRQ Business Research Quarterly
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded with a grant from the Swedish Research Council for Health, Working Life, and Welfare (FORTE 2017-01063).
Ethical approval
The research project that this study is part of was approved by the Swedish ethical review authority (Nr: 2018/2266-31/5). By answering the survey respondents gave their consent to participate. Data is not analyzed or presented in a way that makes individual identifiable.
Data accessibility
Given restrictions from the ethical review board and considering that sensitive personal data are handled, it is not possible to make the data freely available. Access to the data may be provided to other researchers in line with the Swedish law and after consultation with the Stockholm University legal department. Requests for data, stored at the Stress Research Institute, Department of Psychology, should be sent to
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.