
Abstract
Among the spectrum of Developmental Dysplasia of the Hip (DDH), cases involving dislocation (DDH-dislocation) are not frequently examined in global epidemiological research. This ecological study estimates the incidence of late-diagnosed DDH-dislocation among Colombian children aged 3 months to 18 years, from 2010 to 2020. Data were drawn from the Individual Service Provision Records (SISPRO) and vital statistics provided by the National Administrative Department of Statistics (DANE). A total of 68 460 late-diagnosed DDH-dislocation cases were identified, with a female-to-male ratio of 2.2:1. Annual incidence ranged from 4.3 to 8.3 per 1000 live births. Elevated rates were concentrated in central Cundiboyacense, southern Santander, and the Nariñense Andean Massif regions. These findings underscore the need for a nationwide early detection program designed to reduce late diagnoses, especially in areas with higher incidence rates.
Introduction
Estimates of DDH incidence rates vary widely in the specialized literature, mainly due to the use of different screening methods (clinical examination, ultrasonography, radiography), the application of selective or universal screening, and phenotypic and cultural differences among ethnic groups studied in each research, among other factors. 1 The exhaustive review of Loder and Skopelja 2 reports a DDH incidence between 0.06 per 1000 live births (for Africans) to 76 per 1000 live births (for Native Americans). After 1980, with the introduction of Graf’s method, Loder and Skopelja 2 reported an average incidence estimate of about 7.5 to 34.7 per 1000 for hips above Graf IIa for Caucasians at 4 to 6 months of age. The very definition of “late diagnosis” is also a matter of debate in the current literature and is recognized as a major methodological limitation. 3 According to Cheok et al, 4 10 studies defined late-diagnosed DDH as diagnoses made after 3 months of age. For late-diagnosed DDH dislocation, Wenger et al 5 proposed a late-diagnosis threshold for DDH dislocation as early as 2 weeks after birth, while Bjerkreim and Johansen 6 set it at 1 month of age.
Developmental dysplasia of the hip (DDH) risk factors, as described by Loder and Skopelja, 2 include sex, breech delivery, family history, and ethnic origin.7,8 Females comprise 76% of cases. A positive family history is found in 12% to 33% of patients. 2 Regarding ethnicity, the incidence is higher among Native Americans and Caucasians (particularly Scandinavians) and lower among Asians, Africans, and their descendants.1,2 After birth, the practice of swaddling –a common cultural practice in several places around the world,2,7,9 -11 such as in Japan– is a significant risk factor for DDH. Indeed, the city of Kyoto implemented a public initiative to discourage swaddling, obtaining a substantial reduction in the DDH incidence: from 53 per 1000 live births between 1971 and 1973 to about 6 per 1000 live births between 1974 and 1976. 10
Early diagnosis is essential for improving the outcome of DDH treatment approaches.12,13 In 2015, the American Academy of Orthopaedic Surgeons (AAOS) published a Clinical Practice Guideline for the early detection of DDH in patients younger than 6 months of age. 14 Recent works aim to achieve further standardization of early diagnosis practices and even clinical and ultrasound-based screening programs using Graf’s method.12,13 In particular, the international expert meeting held in Csolyospalos (Hungary) in 2018 reached a consensus on several critical aspects of DDH detection and treatment. 12 Key recommendations included the necessity of ultrasound screening to address the limitations of clinical examinations, the implementation of a nationwide universal screening program based on the Graf technique, and the application of such a program to every newborn before 6 weeks of age by adequately trained healthcare professionals. 12 The goal is to obtain an early diagnosis to enable the timely selection of a therapeutic approach12,15 to improve the patient’s prognosis. 15
The potentially high incidence rates of DDH dislocation and the severe sequelae of this disorder in the adult lives of late-diagnosed patients make DDH dislocation a public health problem.1,16 -18 However, to the best of the authors’ knowledge, no nationwide estimation of the incidence of late-diagnosed DDH dislocation has been conducted in Colombia, and only preliminary studies on this research topic have been published in Latin America, despite DDH dislocation being a common condition in pediatric orthopedic consultations. Thus, the main goal of this study is to provide a reliable estimate of the incidence of late-diagnosed DDH dislocation in the Colombian pediatric population between 2010 and 2020, addressing the knowledge gaps about the incidence rate of this disease in Colombia.
Methods
This is a descriptive ecological study following an approach adapted from the method of Sánchez et al 19 about the incidence of skin cancer in Colombia, in a similar fashion to the approach of Den et al 9 for Japan, and Degnan et al 20 for the United States, both in the field of the Epidemiology of DDH. The supporting data were collected from three official Colombian sources:
• The National Demographic and Health Survey, ENDS 2015. 21
• The Individual Service Provision Records (RIPS) database from the Integrated Social Protection Information System (SISPRO) of the Ministry of Health and Social Protection (Ministerio de Salud y Protección Social). 22
• The Colombian national record of births and deaths from the vital statistics of the National Administrative Department of Statistics (DANE). 23
Given this is an ecological study, all the available and relevant records from these comprehensive public datasets were used. The raw data acquired from RIPS records (containing specialist-based diagnoses from pediatricians and orthopedists) were curated and transformed into a unified dataset for patients older than 3 months, as they correspond to late-diagnosed DDH dislocation cases resulting from the application of the Colombian protocol. Then, information on live births during the study period (2010-2020) was obtained from the country’s birth registry. 23 The diagnostic reports for confirmed cases of DDH dislocation were constrained to the same time window. For validation purposes, an estimate of the late-diagnosed DDH dislocation incidence rate was obtained using anonymized data from the 2015 ENDS survey. 21 Under the official DDH diagnostic protocol in Colombia, the diagnoses present in the dataset were supported by X-ray imaging at 4 to 6 months of age, except for a negligible subset of early-diagnosed cases based on clinical screening and ultrasonography.
The International Classification of Diseases, 10th Edition 24 (ICD-10) was used to select the records whose codes correspond to DDH-dislocation, using the same definition employed by Den et al 9 and Thallinger et al, 25 that is, codes under the Q65 classification: Q65.0 (“Congenital dislocation of the hip, unilateral”), Q65.1 (“Congenital dislocation of the hip, bilateral”), and Q65.2 (“Congenital dislocation of the hip, unspecified”). The resulting filtered dataset allowed the application of the inclusion and exclusion criteria for this study:
Inclusion Criteria
• Records of new cases of DDH-dislocation for patients between 3 months and 18 years of age at the time of diagnosis (late diagnosis).
Exclusion Criteria
• Records of cases reporting concurrent comorbidities of the hips and lower limbs causing hip dislocation unrelated to developmental dysplasia of the hip.
• Records of cases with incomplete or missing diagnostic data, such as the patient’s age at the diagnosis.
• Records of cases previously included in the dataset.
Using these inclusion and exclusion criteria, the resulting query to the public repository yielded 68 460 valid records, thus forming the sample for this study. Based on these RIPS data, stratified by sex and year, it is possible to estimate the annual incidence of late-diagnosed DDH-dislocation in Colombia as the ratio of new cases (the number of first consultation records corresponding to patients older than 3 months of age) in the RIPS database containing confirmed diagnoses of DDH-dislocation to the total number of live newborns, within the corresponding time window, and scaled per 1000 live births:

The incidence rate is reported annually with 95% confidence intervals (C.I.) for 3 groups: males, females, and the total population. A Poisson distribution is used to model the discrete nature of the data. However, due to the large dataset size, it is approximated by a normal distribution. The C.I. is calculated as
Ethical Considerations
This study was strictly conducted under the ethical standards of the Declaration of Helsinki. Thus, its supporting protocol was approved by the Ethical Committee of the Hospital Infantil Universitario de San José during its ad-hoc meeting on April 16, 2024. Since all datasets used in this work were extracted from previously anonymized public health databases, informed consent was not applicable.
Results
The total number of live births registered by Colombia’s DANE between 2010 and 2020 was 7 166 168. For the 3 selected ICD-10 diagnostic codes mentioned above, 68 460 records with cases of late-diagnosed DDH dislocation in the time window for subjects under 18 years of age were included. The incidence rate in Colombia during the period 2010 to 2020 ranged from 4.3 [95% C.I.: 4.29-4.30] per 1000 live births in 2020 to 8.3 [95% C.I.: 8.34-8.35] per 1000 live births in 2014 (see Table 1). The maximum incidence rates were observed in 2014, with values of 11.50 [95% C.I.: 11.49-11.51] for females and 5.34 [95% C.I.: 5.33-5.35] for males, consistent with the female predominance reported in the literature.
Yearly Late-diagnosed DDH-Dislocation Incidence Rate (Per 1000 Live Births) in Colombia (2010-2020).

95% C.I. stands for “95% Confidence Interval.”
Figure 1 presents the trend in the annual incidence rate estimates of late-diagnosed DDH dislocation in Colombia from 2010 to 2020. After confirming that no autocorrelation was present in the time series for each group, linear regression analysis showed that the decreasing trend observed in this plot is statistically significant (p-values: .035 for females and .039 for males).
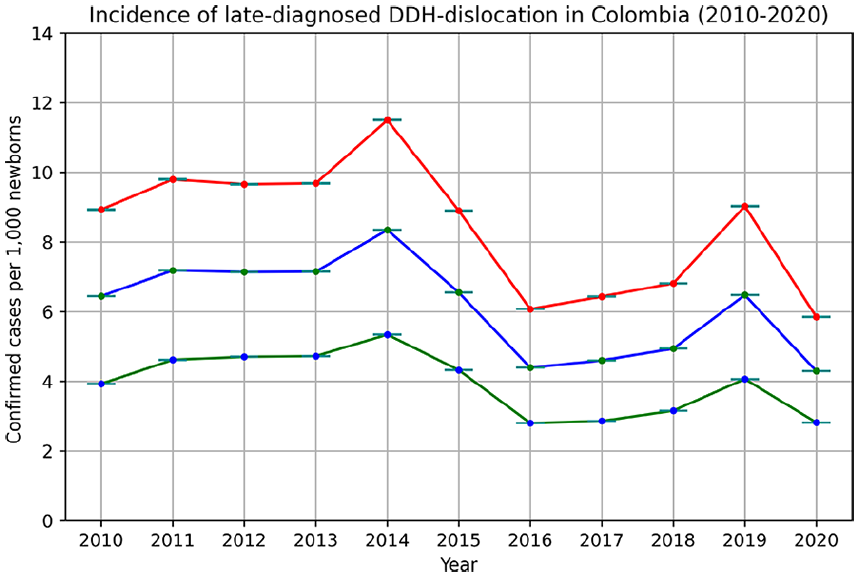
The incidence rate of late-diagnosed DDH-dislocation in the Colombian population born from 2010 to 2020 per year discriminated by sex: blue for the total population, red for female subjects, and green for male subjects.
Figure 2 shows the geographical distribution of the late-diagnosed DDH dislocation incidence rate for 2010 and 2020 (the first and last years in the observation window). This map illustrates the yearly count of new cases per municipality, offering insights into their spatial distribution in Colombia. Remarkably higher rates for male and female subjects are observed in municipalities within the Eastern Cordillera, particularly in the central Cundiboyacense region and around the southern Andean Massif (department of Nariño). Conversely, there is a discernible trend of lower incidence rates in rural areas with warmer climates. In contrast, the number of new cases increased in 2020 compared to 2010 within the eastern departments of Santander and Norte de Santander.
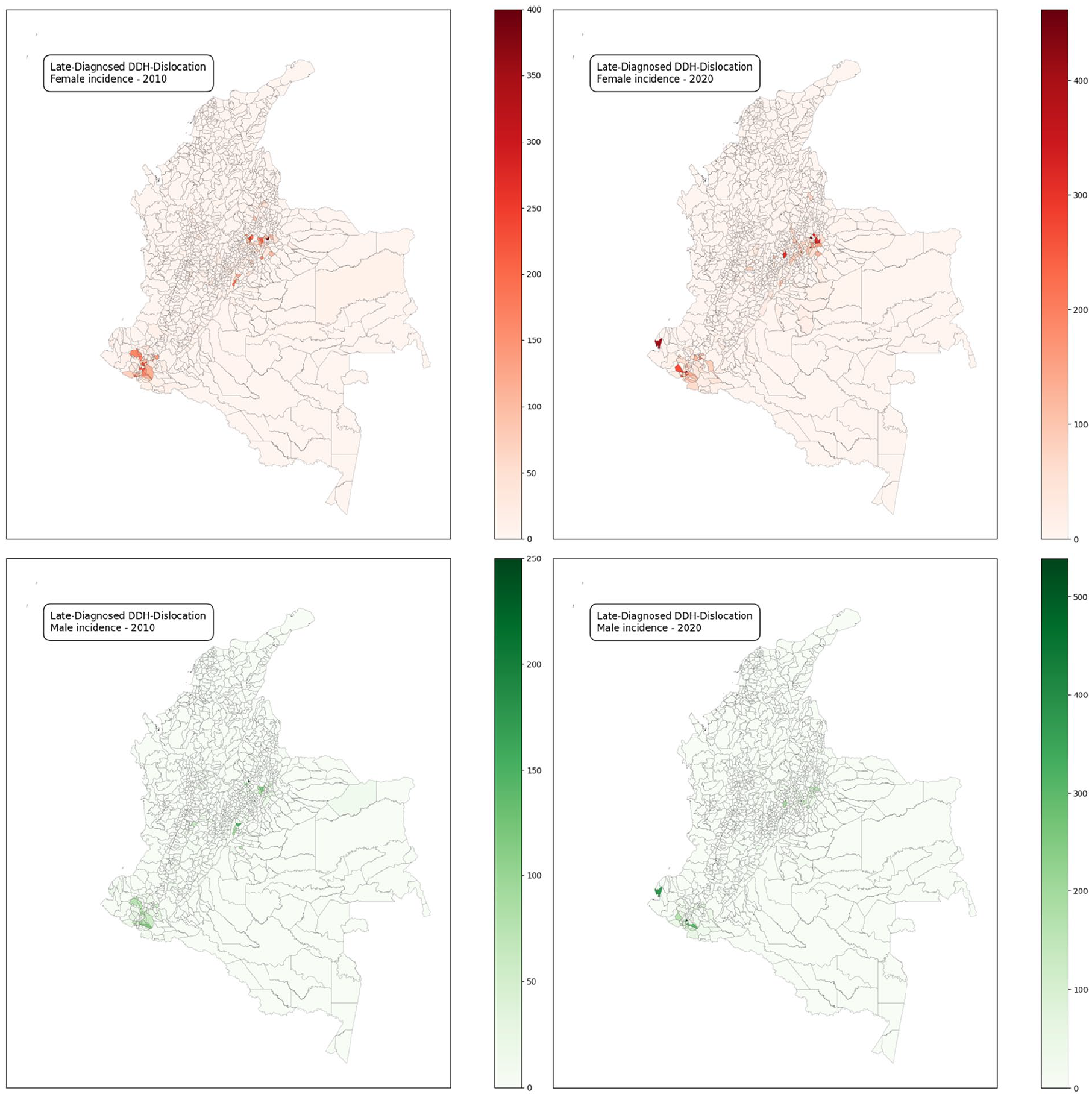
Geographical distribution of late diagnosed DDH-dislocation incidence rate in Colombia discriminated by sex (years 2010 and 2020).
Discussion
The main contribution of this study is the estimation of the incidence rate of late-diagnosed DDH dislocation in the pediatric population of Colombia per year between 2010 and 2020. With 68 460 cases identified during the study period, the observed incidence rate ranged from about 4.3 to 8.3 per 1000 live births annually, consistent with the worldwide incidence rates reported in the literature 2 (Table 1). These figures align with findings from both global and regional studies, yet they are significantly higher than those observed in countries with higher Human Development Index (HDI) scores. For instance, the incidence rate of late-diagnosed DDH dislocation reached a value of 0.4 per 1000 live births in Norway between 1975 and 1979, according to the early work of Bjerkreim and Johansen, 6 while it was just above 0.1 per 1000 live births in Sweden between 2000 and 2009. 5
On the other hand, Latin American countries share ethnic, social, and demographic features with Colombia, yet very few works report epidemiological data on DDH and, particularly, on DDH-dislocation. In Mexico, 26 a DDH dislocation incidence rate of 2.0 per 1000 live births has been reported. A recent study on male cases in Brazil 27 concluded that the most frequent form of DDH, according to a radiological classification, is high dislocation (28.7% of the cases), followed by subluxation (20.4% of the cases). Romero et al 28 performed a risk factor retrospective study in Chile, finding the main risk factors are associated with a positive family history of DDH and breech presentation of the newborn; they also reported a female/male ratio of about 6.5:1.
Figure 1 depicts a long-term downward trend in late-diagnosed DDH dislocation incidence rates in Colombia, with local maxima in 2014 and 2019. These results also indicate a female predominance (female-to-male ratio of 2.2:1) regardless of geographical differences, a well-known trend consistent with the findings of previous studies.2,29,30 A higher concentration of DDH dislocation cases in high-altitude mountainous regions has also been found, particularly within municipalities in the Colombian Eastern Mountain Range, notably the Cundiboyacense region and the Nariño Andean Massif. Conversely, rural areas with warm climates show significantly lower DDH dislocation incidence rates (Figure 2). Genetic and phenotypic features, as well as cultural practices associated with climatic conditions—such as traditional childcare customs like swaddling in specific high-mountain regions of Colombia—may contribute to significant differences in the incidence rates of DDH-related dislocations between colder and warmer regions. Consistent with this observation, several studies have documented a trend of elevated DDH incidence rates for births occurring during winter in temperate zone countries. 2 However, further research on these factors is needed in Colombia and Latin America.
Current official screening protocols for newborns in Colombia31-33 do not recommend hip radiography or ultrasound unless risk factors are identified or abnormalities are detected during an adequately conducted physical examination. 34 These guidelines apply strictly to newborns and do not cover criteria or practices beyond the first weeks of life, even if risk factors or abnormalities are identified during physical examination. 33
Given that most of the studies in the literature include the entire DDH spectrum,1,2,9,29,30 it is relevant to point out that their incidence estimates vary widely according to the subject’s age when ultrasonography is used. 35 When such scans are performed at birth, incidence rate can reach values of 80 per 1000 live births, yet it gradually decreases to 7.5 per 1000 live births for Caucasians when ultrasonography is performed at 4 to 6 weeks of age. 2 As mentioned above, the results of this work show several extreme values along the study time window, especially in the years 2014 and 2019 (Figure 1).
Nevertheless, the implementation of a screening program aimed at early diagnosis of developmental dysplasia of the hip (DDH) is typically followed by a decrease in the incidence of late presentations of DDH dislocation, as demonstrated by the results of Sweden’s nationwide program. 5 Indeed, several studies report that early diagnosis significantly reduces the need for surgical treatment. Thallinger et al 25 reported an incidence rate of open reduction in Austria as low as 0.12 per 1000 live births after the initiation of their screening program. Similarly, Wenger et al 36 found that implementing a secondary screening program in Sweden—with additional clinical examinations at 6 to 8 weeks, 6 months, and 10 to 12 months of age—reduced the proportion of high dislocation cases from 38% to 11% compared to when secondary screening was not performed.
Despite ongoing debates37,38 and some inconclusive results (eg, those related to the UK program 39 ), expert consensus initiatives, such as those reported by O’Beirne et al. 12 and Agostiniani et al, 13 strongly recommend the use of universal ultrasound screening. This approach supports the prevention of late diagnoses3,4,40,41 and reduces the need for surgical treatment interventions.25,36,42 To ensure their quality and reproducibility, both clinical and ultrasound-based examinations must be performed by expert healthcare professionals, while the establishment of continuous education programs for the staff in charge is highly recommended.12,13,43
Study Limitations
This study was performed on databases without access to specific medical records, so its results may be affected by under-registration since the RIPS are manually fed with ICD-10 diagnoses. Under- and delayed registration may also be present in some municipalities along the country’s Pacific coast, where the provision and reporting of healthcare services face significant difficulties due to geographical accessibility.
Additional limitations include the lack of stratification by severity within the DDH spectrum and the potential for data loss due to emigration. Some estimates suggest that Colombian internal and external migrants could exceed 4 million, nearly 10% of the country’s population. The perennial migration of Colombians from rural to urban areas and abroad, driven by internal armed conflict and poverty, peaked during the intense violence period between 1996 and 2000 44 but remained significant during the study period under consideration.
Conclusion
As far as the authors know, this study is the first to assess the incidence of late-diagnosed DDH dislocation in Colombia and Latin America. By considering the region’s distinct geographical, genetic, and cultural factors, this research offers insights that can support future DDH research and the formulation of effective public health strategies to mitigate the impact of this disease.
Indeed, late-diagnosed DDH dislocation is a significant public health concern in Colombia, with an estimated incidence of 4.3 to 8.3 per 1000 live births from 2010 to 2020. Higher rates are exhibited in the mountainous Colombian Andean region. Several studies in the literature report significant reductions in the incidence rates of late-diagnosed developmental dysplasia of the hip (DDH) and, specifically, DDH dislocations after the implementation of nationwide screening programs5,25 that combine expert clinical examination with ultrasound techniques (eg, Graf’s method). Thus, the authors believe adopting such a strategy could be valuable for the public health management of this disease in Colombia.
Footnotes
Authors’ Note
Marco Mahecha is also now affiliated to Hospital Infantil Universitario de San José, Bogotá, Bogotáá, Colombia.
Author Contributions
Víctor Vargas: Conceptualization, Methodology, Formal analysis, Investigation, Writing – original draft, Writing – review and editing, Supervision. Alejandro Satizábal: Data curation, Formal analysis, Writing – original draft. Marco Mahecha: Conceptualization, Formal analysis, Writing – original draft. Diana Patricia Rivera Triana: Methodology, Writing – original draft. Gloria Belén Machado: Methodology, Validation, Writing – original draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This work was approved by the Ethics Committee for Research (Comité de Ética en Investigación con Seres Humanos de la Fundación Hospital Infantil Universitario de San José, Bogotá, Colombia), on April 16th, 2024. No direct measurements nor procedures were performed on any subject for this study. Since the data supporting this work were acquired from public health databases under the administration of the Colombian government, all records were previously anonymized and complied with Colombian and International regulations on data privacy and security.