
Abstract
Objective. Analyzing possible determinants for pulmonary tuberculosis (PTB) in under-five children with stunting and severely stunting in Bandung. Methods. Data was collected from 64 community health centers in Bandung using multiple stratified random sampling. Medical history, body measurements, tuberculin skin tests (TST), and chest X-rays (CXR) were collected. Possible determinants to PTB were analyzed using multiple logistic regression (P value of <.05 was significant). Results. 169 under-five children with stunting and severely stunting were included. 59.76% of children were diagnosed with PTB. The absence of BCG scars and weight-for-age were significant determinants of PTB (P value <.05). Conclusions. PTB was observed in more than half of stunted and severely stunted under 5 children. BCG scars are a protective factor, while weight-for-age is a risk factor for stunting and severe stunting.
Introduction
A child mortality rate of approximately 90% of 205 000 children can be attributed to undiagnosed and untreated TB infection, making children a particularly vulnerable population to the disease.1 -5 In 2020, Indonesia ranked second among nations with the highest prevalence of TB, following India, despite the possibility of unreported and diagnosed TB cases.5 -7
The issue of stunting in children remains a significant concern in developing nations.8 -10 While prevalence of stunting in under-five children in Indonesia had decreased from 27.7% in 2019 to 24.4% in 2021, it remained relatively high in comparison to other nations. 10 The West Java government is reducing stunting by working with various stakeholders, improving nutrition and clean water access, strengthening integrated health center (Posyandu [Posyandu is a mix of the Bahasa Indonesian words pos, pelayanan, and terpadu, translated into “integrated health center” in the context of health facility for the community]), enhancing health services, educating about nutrition, monitoring progress, and partnering with private sectors and NGOs. Based on the Indonesia Health Profile 2021, West Java had the highest pediatric TB prevalence in Indonesia, accounting for 27.2% of all TB cases in individuals aged 0-14 years.11,12 Considering the limited amount of resources, solving such an issue potentially requires a significant allocation of financial resources and effort. 13
Previous study conducted in other countries has identified the determinants of stunted growth in TB-infected children;8 -10 However, to the best of the authors’ knowledge, this is the first study that specifically examined the determinants that contribute to stunting and severe stunting in Indonesian under-five children. Studies on PTB in stunted and severely stunted under-fives are particularly crucial as these children are more susceptible to infections, including TB, due to a weakened immune system resulting from malnutrition. Stunting and TB have some overlapping risk factors, such as poverty and poor living conditions, which exacerbate disease progression and complicate diagnosis. Understanding this relationship can improve precision of diagnosis, refine TB control programmes, and guide integrated public health strategies to address both conditions. This study is important for developing comprehensive interventions to reduce the double burden of TB and malnutrition, which will ultimately improve the long-term health and outcomes of these vulnerable children.
This study was expected to provide sufficient data to assist in the formulation of appropriate health policies aimed at achieving the goals outlined in the End TB strategy. 14
Methods
A community-based cross-sectional study was conducted in Bandung City, encompassing 23 sub-districts of 64 community health centers, from May 30, 2022, to June 13, 2022. Bandung is the capital city of West Java and the fourth-most populated province in Indonesia. Bandung consisted of 30 sub-districts and 74 community health centers. In 2021, data from the Bandung City Health Office showed that out of 7568 children under 5 years old, 5791 were stunted and 1777 were severely stunted across 30 sub-districts in Bandung. However, 7 sub-districts were excluded from the study due to low numbers of stunting cases.
A sample size calculation, using a confidence interval of 95% and an error range of 0.12-0.15, determined that between 131 and 204 children were needed for the study. The research was eventually conducted on 174 children, but 5 were excluded, leaving 169 for analysis. The subjects were selected using proportionate stratified random sampling from 23 sub-districts to represent both stunted and severely stunted children. Random selection was performed with the help of Excel to determine the specific children to be included.
The inclusion criteria of the study are as follows:
- Age <5 years
The exclusion criteria of the study are as follows:
- Previous history of receiving TB treatment
- Previous history of positive tuberculin skin test (TST)
- Recent immunization (<1 month ago)
- Medical history of severe allergies
- Diagnosed with upper respiratory tract infection
- Parents refused for reading their child’s TST within 48-72 hours.
Exclusion of history of TB disease and positive TST were aimed to remove the possible confounding variable brought by previous history of anti-tuberculosis treatment (ATT).
After the randomization and prior data screening from secondary data sources (medical records of under-five children in participating community health centers), community/medical representatives were requested to contact the parents/legal guardians of the child. Once the parents/legal guardians gave their consent for their children to participate in this study, the children were then transported to the Bio Farma Clinic for TB screening and anthropometric measurement. Child growth standards from 2006 World Health Organization (WHO) were used for diagnosis of stunting by comparing the growth curves according to the sex and age (body length < −2 SD and body height < −3 SD). Anthropometric measurements for children (<2 years) were carried out using Elitech DIGIT-ONE BABYÒ/TD 05219B3340 (accredited by the Ministry of Health of the Republic of Indonesia, Number 10901410291). For older children (>2 years), Elitech DIGIT-PROÒ/TD 09219B3781 was used for anthropometric measurements.
Variables collected consisted of age, sex, anthropometric variables (body weight, body length/height, birth weight, and birth length), history of exclusive breastfeeding (until sixth month of life), history of close contact with previously known TB patients, history of TB contact, parents’ height and education, parents’ occupation, monthly household income, the suggestive clinical manifestation of TB, evaluation of living conditions, source of drinking water in the household, and chest x-ray results. Tuberculin PPD RT23 SSI and injected intracutaneously (0.1 ml) in the right lower arm were used for TST test. Chest x-ray (CXR) was performed on the posteroanterior (PA)/antero-posterior (AP) views. Stunted growth (based on 2006 World Health Organization [WHO] child growth standards). Assessment of stunting or severe stunting in the study participants was conducted using height-for-age z-scores (HAZ) that were age- and sex-appropriate, following the WHO chart growth standard (WCGS). Based on WCGS, stunting was classified as < −2 SD to −3 SD, while severe stunting was classified as < −3 SD. 15 The TST results were interpreted 48-72 hours after injection by pediatricians during their visit to the patients’ addresses. Positive results in TST were defined as induration diameter (after 48-72 hours) of >5 mm for children with severe wasting and >10 mm for children without severe wasting. Moreover, the diameter of the induration was measured in millimeters (mm). Three radiologists interpreted the results of the CXR and the interpretation would be based on 2 or more similar conclusions made by the 3 examiners for each child. This study classified TB status in children into the following categories:
1. Tuberculosis (TB) was defined as radiological signs in the lung parenchyma or the tracheobronchial tree suggestive of PTB, such as tuberculous intrathoracic lymphadenopathy (mediastinal and/or hilar), without any other radiographic abnormalities in the lungs and with prior results of bacteriological or clinical diagnosis. 11
2. A TB infection was defined as a positive TST without the clinical and radiological signs associated with TB. 11
3. A non-TB infection was defined as healthy children with negative TST and normal CXR results. 11
Three independent pediatric respirology consultants (HMN, SS, and DAW) determined the TB status. Moreover, they determined the interpretation results for each child based on 2 or more similar conclusions.
Independent variables in this study were parents’ TB status, low birth weight, history of exclusive breastfeeding (until sixth month of age), source of drinking water, monthly household income, parents’ education, and history of TB contact. Dependent variables are stunting or severe stunting on children included in the study.
The demographics were presented using descriptive statistics. Moreover, this study employed logistic regression to analyze the following variables: maternal height, birth weight, exclusive breastfeeding, tuberculosis status, water source, family income, parents’ education level, and parents’ occupation. Logistic analysis was employed for the purpose of observing the association between the variables and the occurrence of stunting and severe stunting in patients. Furthermore, the results of logistic regression were presented as a P value and an odds ratio (OR) with a confidence interval (CI) of 95%. Statistical analyses were performed using SPSS Version 26.
This study was conducted in accordance with the Declaration of Helsinki. Moreover, the Ethical Review Board of the Faculty of Medicine, Universitas Padjadjaran, granted ethical clearance for this study (Number: 350/UN6.KEP/EC/2022). Additionally, prior to the study’s conduct, the legal guardians/parents provided written consent to participate in this study. To minimize the risk of COVID transmission during the pandemic, the authors adhered to government-mandated safety protocols during the study. These protocols included conducting prior screening and limiting close contact with both the staff and children participating in this study.
Results
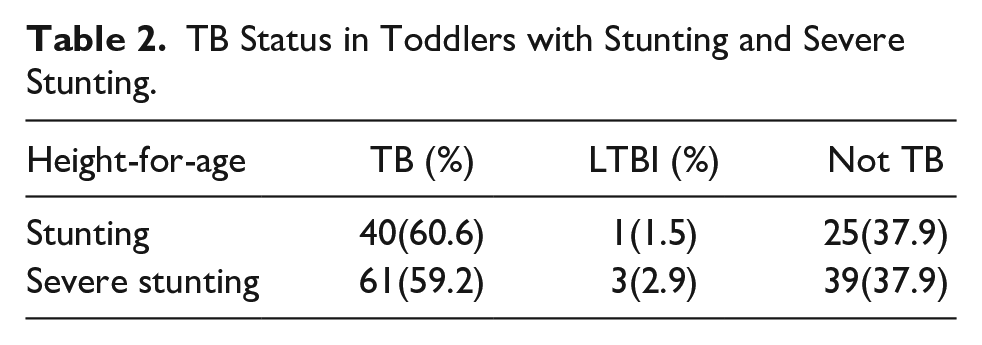
According to the findings of this study, 66 (39.05%) of the 169 children had stunting, and 103 (60.95%) had severe stunting. Furthermore, the age range of the participants was 9-59 months, with a median age of 34.26 months. It was discovered that babies exclusively nursed for 6 months accounted for 86.39% of the total. Moreover, most children had birth weight of more than 2500 grams (75.61%). This study revealed that 156 children (92.83%) of 169 children have received the BCG vaccination. Only 10 of 169 (5.92%) children have a history of TB contact with their families; low prevalence of history of TB contact may be related with low detection rate (55%) in the previous study in West Java. 16 Decreased appetite for the last 2-3 months (35.50%) was the most prevalent clinical symptom in this study, followed by failure to gain weight in the last 2-3 months (35.50%) and weight loss (18.93%). Additionally, this study found that 30.18% of the children had TST induration diameters larger than 10 mm. Furthermore, most of the CXR results were suggestive of TB (84.01%). The findings indicate that 101 (59.76%) children were diagnosed with TB infection and 4 (2.37%) were diagnosed with latent TB infection. The remaining 64 (37.87%) children had non-TB infection (presented with negative TST and normal CXR results). In addition, in the stunting child group, 60.6% of children were diagnosed with PTB, and in the severe stunting group, 59.2% of children were diagnosed with PTB. (Tables 1 and 2)
Characteristics of Toddlers with Stunting and Severe Stunting in Bandung.

TB Status in Toddlers with Stunting and Severe Stunting.
According to the findings of this study, the most common level of parents’ education is senior high school, with mothers at 39.05% and fathers at 42.01%. Moreover, the predominant fathers’ occupations are laborers (49.70%), followed by private employees (26.95%) and entrepreneurs (20.36%). Additionally, most of the mothers worked as housewives (94.05%). Additionally, the mothers’ height was mostly shorter than 150 cm (60.39%). The vast majority (73.37%) of household income was less than IDR 2 500 000, significantly smaller than the minimum regional wages as decreed by the Governor of West Java (IDR 3 774 860). (Table 3)
Parents’ Characteristics of the Children Included in the Study.

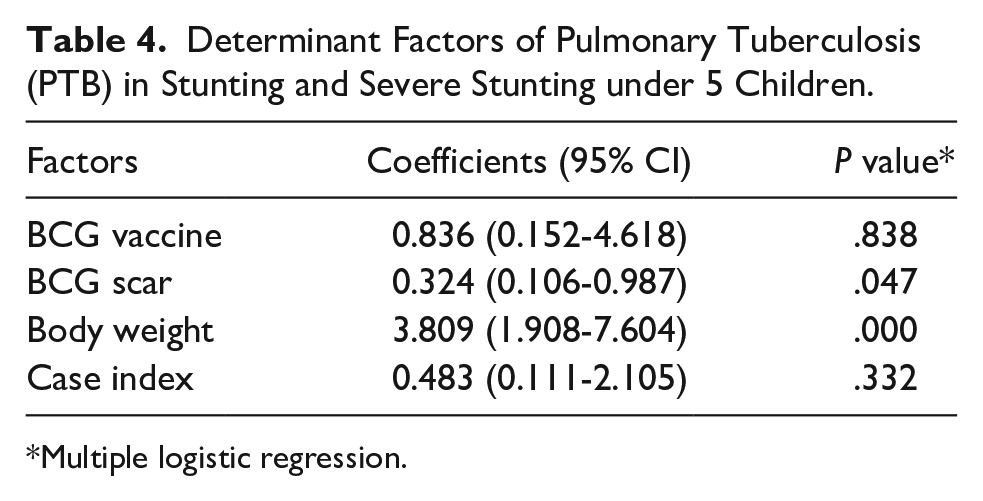
Among the determinants, BCG scar and body weight-per-age were significant (P < .005). BCG scar was associated with lower risk for stunting and severely stunting (P-value .047, 95% CI: 0.324 [0.106-0.987]). Body weight was risk factor of stunting and severely stunting (P-value .000, 95% CI: 3.809 [1.908-7.604]). (Table 4)
Determinant Factors of Pulmonary Tuberculosis (PTB) in Stunting and Severe Stunting under 5 Children.
Multiple logistic regression.
Discussion
Data from the Indonesian Toddler Nutrition Status Survey 2021 showed a decrease in the prevalence of stunting in under-five children, from 27.7% in 2019 to 24.4%. 17 Moreover, the prevalence of stunting in West Java province exceeded the national stunting rate of 24.5%. Furthermore, the Bandung City is among the ten regions in West Java with the highest number of stunted children, at 26.4% 18 Despite the fact that the global stunting rate is decreasing annually, the rate of decrease is relatively slow compared to the target set by the Global Nutrition Target 2025.10,18,19
The provinces of West, East, and Central Java are the most significant contributors to TB cases in children aged 0-14, accounting for almost half (46%) of all new cases of TB in Indonesia. 18 The results of this study support the high prevalence of TB in under-five children (62.13%). It was found that in the stunting group, 39 of 66 children (59.09%) were diagnosed with TB, whereas in the severe stunting group, 66 of 103 (65.08%) were diagnosed with TB. The results of this study support the high prevalence of TB in under-five children (62.13%). Furthermore, the findings revealed that in the stunting group, 0.59% of children were diagnosed with TB infection, whereas in the severe stunting group, 2.36% of children were diagnosed with TB infection. The results of this study are significantly different from the previous study conducted in Makassar that focused on other areas of Indonesia. The study showed that the TB prevalence found in stunting and non-stunting under-five children was 38.10%. 20 In addition, other study conducted in the West Bandung sub-district using different methods and populations found that 26% of under-five children and 14% of under-five children with severe stunting had TB. 21
Based on the stunting report data from the Bandung City Health Office for the previous year, the number of severely stunted children was estimated to be lower than stunted children. However, this study had found the opposite. Potentially, recategorization of stunting/severe stunting after remeasuring anthropometric measurements using calibrated equipment alluded to the differences in measurement methods between the centers and this study, causing variance between the sub-district and research data. Implementation of the Posyandu program was temporarily halted during the pandemic, potentially resulting in issues for regular anthropometric measurements for the children.
Previous studies have identified the main determinants of stunting in Indonesia, including the absence of exclusive breastfeeding during the first 6 months of life, low socioeconomic status, lack of education about stunting, chronic infection, premature birth, low birth weight, and maternal height <150 cm.11,22 -25 In contrast to the results of this study, 86.39% of children were exclusively breastfed in the first 6 months of life. However, malnutrition and poverty emerged as significant contributors to the prevalence of stunting. 25 Furthermore, the economic impact of the COVID-19 pandemic on poverty is evident in the increasing unemployment rate, which increased from 6.92% in February 2020 to 9.76% in August 2020. 18 Many experts consider poverty a crucial determinant of stunting in under-five children.10,22,25 Nevertheless, according to this study, nearly 80% of the families had a household income less than the Bandung City minimum wage that year. In this study, while household income was not statistically significant correlated with stunting, it is likely one of the causes of stunting because poor household conditions may make parents unable to meet their children’s nutritional intake.
This study discovered that maternal height was mostly below 150 cm (60.39%). Nevertheless, a number of previous studies conducted in Indonesia have shown moderate to significant correlations between short maternal height and stunting in children.18,22,24,26 The prevalence of severe stunting was higher compared to stunting. This indicates that there may be variations in the criteria used to diagnose stunting or severe stunting between the community health centers in Indonesia and the standardized anthropometric measurement used in this study. Furthermore, due to the lack of training of community health center officers involved in this study, the measurement’s conduct may differ from that of officers of other sub-districts. In addition, previous studies have shown that anthropometric measurements taken from children with aberrant body composition might vary both among and between observers. 27
Several previous studies have established a correlation between TB infections and stunting.20,28 According to a cross-sectional study conducted in 13 Makassar Municipality healthcare facilities, 30.18% of 126 under-five children with stunting had TB and a positive TST. 20 In those with moderate to severe impaired nutritional status, the chance of TB infection was 2.36 times greater. 20 In addition, based on a case-control study conducted in 7 community health centers in West Bandung sub-district, West Java, which examined 98 under-five children diagnosed with TB, it was found that under-five children with stunting had a higher risk of TB. It was also explained that stunted and severely stunted children have a risk of TB that is 3.5 and 9 times higher, respectively. 21
Many TB cases in children have an unidentified case index (the source of infection) due to several key factors such as undiagnosed subclinical TB due to asymptomatic features. These individuals may still spread TB to children, but their status as carriers remains unidentified. Adults with active TB late due to barriers such as limited access to healthcare, stigma, or lack of awareness. Third, contact tracing may be incomplete or ineffective. If all close contacts are not thoroughly screened, the index case may go unidentified. Low prevalence of history of TB contact may be related with low detection rate (55%) in the previous study in West Java. 16 Stigma surrounding TB can lead individuals to avoid seeking medical attention or disclosing their TB status, further complicating the identification of the source of infection. These factors contribute to the challenge of identifying the case index in pediatric TB, making it difficult to fully control and prevent the spread of the disease.
There are some limitations to this study. This study only conducted PA/AP views without lateral views on CXR examinations, potentially presenting a risk for over- or underdiagnosed TB cases in under-five children. Moreover, 3 pediatric pulmonology consultants independently reviewed the case before inclusion to minimize the risk of diagnostic inaccuracies related to CXR results in under-five children suggestive of TB. Additionally, the number of subjects was relatively small. Cross-sectional study design cannot determine the effect of catch-up growth in stunted / severely stunted children for the determinants. Limitations for available resources for urine lipoarabinomannan (LAM) test and recommended molecular test in the included community health centers may affect the accuracy of TB diagnoses in this study. In addition, this study did not collect human immunodeficiency status (HIV), despite the relatively significant prevalence of TB with HIV coinfection. 29 The variances in data collection among each community health center involved in this study caused incomplete data for HIV status for the patients included in this study.
Conclusion
More than half of children with stunting were diagnosed with TB, and a small number had a TB infection. Among the other determinants, BCG scars and body weight were significant determinants of stunting. BCG scars were a protective factor while the body weight was a risk factor for stunting. Significant efforts and urgency in the implementation of public health programs are required to prevent stunting and wasting, the possible economic impact, the high prevalence of pediatric TB, and the compounding risk of developmental delays in Indonesian children with stunting, wasting, and pediatric TB infection.8 -10
Footnotes
Authors’ Contribution
CC and HMN initiated the study of ideas and concepts. CC and HMN contributed equally to the intellectual content of the manuscript. FRR contributed to designing statistical analysis concepts, and CC performed the analysis, which FRR supervised. CC wrote the first draft of the manuscript, supervised by HMN and MAT. The remaining authors critically reviewed and approved the final version of the manuscript.
Availability of Data and Materials
The datasets used and analyzed during the study are available from the corresponding author on reasonable request.
Consent of Publication
All the authors in this study have consented to the publication of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: In-kind sponsorship was provided by Bio Farma Group in form of the venue and equipment utilized during the period of the study. No monetary compensation or funding were provided by Bio Farma Group.