
Abstract
Working with chronically ill children can overwhelm for professionals. It is necessary to study the factors related to compassion fatigue and satisfaction in order to effectively deal with it. Using a narrative review and inclusion criteria, we searched online databases for related studies from 2000 to 2023. Twelve articles were included in the final review. Understanding compassion fatigue/satisfaction will help to solve personal and professional problems and increase productivity, leading to positive outcomes for the patient, family, and the organization. This study identifies several factors that contribute to compassion fatigue (CF) in pediatric healthcare providers. These factors include workload, patient connections, lack of support, exposure to trauma, personal trauma, job dissatisfaction, and neglecting self-care. It is crucial to address these factors through targeted interventions and organizational support. Implementing evidence-based interventions shows promise in reducing the impact of CF, fostering a resilient healthcare workforce, and improving patient care.
Introduction
Studies conducted in the healthcare system show that the physical, emotional, social and spiritual health of medical staff may be affected for various reasons, for example they may face constant stress related to interacting with a large number of patients with acute problems, trauma and practice environments with limited resources and increasing demand. 1 Healthcare providers are often involved in situations where the family’s suffering is extreme 2 and exposure to suffering may create complex emotions. Staff in a pediatric ward may be asked to join the child’s primary healthcare team to review goals of care and help make critical decisions that can involve complex ethical issues, such as decision-making during end-of-life care. 2 They may also witness the death of a child, face high demands and expectations from families, experience secondary trauma, 3 stressful personal and work events, 4 physical fatigue, personal history of trauma, 2 and lack of social support.5,6
Stressful and traumatic experiences in a pediatric ward may have short and long-term consequences. One of these consequences that has been the focus of several studies in recent years is compassion fatigue (CF). The term “compassion fatigue” was first coined in 1992 when Joinson was studying burnout among emergency department nurses. In defining this term, he stated that health care workers experience changes in their ability to understand feelings and help others due to facing severe and aggressive stress and face some kind of frustration in themselves. These experiences with symptoms of anxiety, feelings of anger, lack of control and indifference were classified as burnout and introduced to the health care community. 7 Compassion fatigue occurs when the therapist loses the ability to empathize and comfort due to long-term involvement or close involvement with caregiving duties. It also occurs due to prolonged exposure to trauma, which leads to a variety of problematic symptoms and may manifest at work and at home. Compassion fatigue may have long-term consequences for the pediatric ward staff, as they must be prepared to help the family of a chronically ill, injured, or dying child, while also being prepared to deal with their own grief. 8 However, CF is not the only consequence of care. Another phenomenon known as compassion satisfaction (CS) has also been observed in the healthcare sector. Compassion satisfaction is a term for positive feelings resulting from helping others in traumatic situations. 9 It is a sense of pleasure an individual experiences from being able to effectively help others in a caring role, and this may include feelings of support from colleagues and satisfaction from being able to contribute to the organization and the greater good. 10 In many cases, it has been suggested that CF and CS can occur at the same time. Compassion satisfaction may reduce the negative effects of compassion fatigue.2,11
To overcome CF and increase CS, the phenomenon itself should be investigated from different dimensions. In recent decades, many related articles have been published, but few articles dealing with CF and CS in pediatric wards are available. Therefore, this study systematically reviewed previous research that examined CF and CS among pediatric ward staff. The present study hopes to contribute to the filed by offering a comprehensive analysis of the compassion fatigue and satisfaction within pediatric wars, a setting that has been underrepresented in existing research. By identifying key predictors and outcomes, this research aims to enhance our understanding of how to support these professionals better. The findings may guide future research and inform policy changes aimed at improving workplace conditions in pediatric wards. The main questions were: Do pediatric ward staff experience CF and CS? What are the risk factors for CF? What are the consequences of CF and CS in pediatric wards? What kind of interventions have been done for CF and CS? And how effective were the interventions after therapy and in the follow-up phase?
Method
A narrative review method was used to systematically review studies on compassion fatigue (CF) and compassion satisfaction (CS) in pediatric wards. The keywords “compassion fatigue,” “compassion satisfaction,” “neonatal unit,” “neonatal intensive care unit,” “intensive care units for pediatric,” “intensive care units for children,” “NICU,” “PICU,” and “health care” were searched in PubMed, Web of Science, CINAHL, PsycINFO, Embase, Cochrane Library, Google Scholar, and Scopus from 2000 to 2023. The inclusion criteria were articles related to staff in pediatric wards, written in English, with full text available, and receiving a high score in quality assessment.
In the initial search, 59 articles were obtained. After removing 15 articles due to database overlap, simultaneous indexing, and duplicate titles, 44 articles remained. The screening of abstracts resulted in the exclusion of 27 articles based on the inclusion criteria, leaving 17 articles. Two articles were then removed due to lack of access to full text and ambiguous results. Finally, 3 articles were excluded based on Gifford’s qualitative assessment (Barr 5 ; Gifford et al, 2007 12 ), leaving a total of 12 articles for the final review. The full text of all papers was studied, and relevant data was extracted based on the research questions (Figure 1).

PRISMA flow diagram from Gifford et al, 2007.
Ethical Approval and Informed Consent
Ethics approval was not required for this narrative review. Also, Informed consent was not required for this narrative review.
Result
This study aimed to synthesize the results of research on CF and CS in pediatric wards. We found 12 papers (Table 1) with 2532 participants. Almost all studies were conducted in developed countries, including 10 in the USA, 1 in Australia, and 1 in Canada. The papers did not report an equal gender distribution, and in all articles, the percentage of female staff was higher than that of men. Three studies used the Compassion Satisfaction and Fatigue Test (CFST)2,11,13 and 7 studies used the Professional Quality of Life scale (ProQoL).4,5,11,14 -16 The work experiences of participants ranged from 5 to 20 years, and the age range of participants was between 20 and 70 years. The education level ranged from a high school diploma to a master’s degree.
Characteristics of Included Papers.
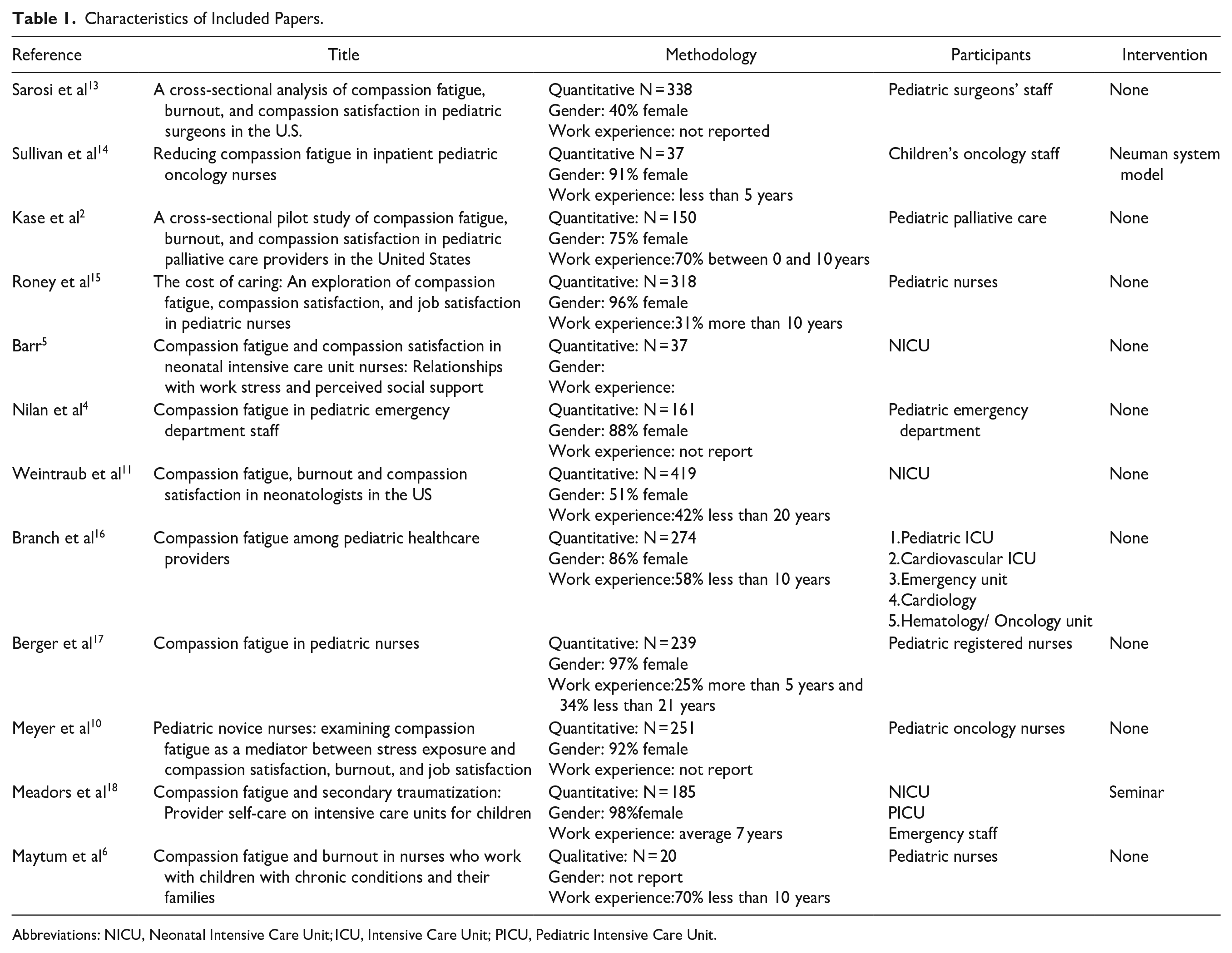
Abbreviations: NICU, Neonatal Intensive Care Unit; ICU, Intensive Care Unit; PICU, Pediatric Intensive Care Unit.
The first question of this research was that “Do pediatric wards’ staff experience CF and CS?” The first and most important finding is that they could experience compassion fatigue and satisfaction concurrently. The majority of pediatric wards’ staff had a high level of CF and CS.11,15 Burnout and high secondary traumatic stress were also reported in pediatric wards, which shows the risk of compassion fatigue.4,16 Compassion fatigue is commonly and episodically experienced by healthcare professionals who work with chronically ill children and their families. 6
The second question was that what are the risk factors for CF? Findings show that work stress,5,11 social support,5,6 work experience,11,14,17 expressing feelings and talking,2,11,13 co-workers and emotional depletion2,11 play important role in creating or reducing CF and CS. Personal events such as loss, suffering, or death in family 4 and a history of trauma and physical fatigue, and personal damage 2 were also reported as influential factors on CF and CS in only 2 studies.
The third question was what are the consequences of CF and CS in pediatric wards? CF and CS are related to secondary traumatic stress,14,18 emotional health, 11 professional performance,6,11 development of resilience, 17 leaving the job and the quality of patient care.6,11
The last question was, what kind of interventions have been done for CF and CS and how was the effectiveness of the interventions after therapy and in follow-up phase? Only 2 studies mentioned an intervention, including a training seminar 18 and using a self-care program called the Newman model. 14 The results indicated that the staff who experienced higher levels of personal stressors, experienced higher levels of clinical stress and CF. The training seminar on CF was successful in increasing awareness and reducing clinical stress among pediatric wards staff. A total of 185 healthcare providers working in a Children’s Hospital attended an educational seminar on compassion fatigue. The participants voluntarily completed questionnaires before and after the seminar. The questionnaires used in the study included a modified version of the Social Readjustment Rating Scale, Index of Clinical Stress, and a compassion fatigue measure developed by the researchers. The research protocol and questionnaires were reviewed and approved by a university institutional review board and the hospital’s NICU, PICU, and PEDS unit leadership teams. This study did not report follow-up data. 18 The Newman model showed that continuous organizational support and intervention can reduce CF and increase CS in nurses. Secondary traumatic stress scores improved significantly from baseline to 4 months. The Neuman Systems Model was used as the guiding framework for this project, which describes an individual as a whole client or client system who interacts with environmental stressors and uses protective mechanisms to cope with them. The model suggests that compassion fatigue is the depletion of one’s core energy due to ineffective coping and resilience against stressors, while compassion satisfaction reflects overall system wellness and resilience influenced by adaptive coping and role-related meaning. The study utilized the ProQOLV scale to measure secondary traumatic stress and compassion satisfaction among pediatric oncology nurses. Coping characteristics were assessed and correlated with ProQOLV subscale scores to identify potential factors associated with compassion fatigue and satisfaction. This study did not have a follow-up. 14
Discussion
According to data synthesis, pediatric ward staff simultaneously experience compassion fatigue (CF) and compassion satisfaction (CS). This finding aligns with previous research that suggests CF and CS are not opposing ends of a spectrum, but rather can coexist.19 -21 One study found that while caring for others can lead to CF, it can also create CS. 22 Another study showed that mothers initially experience CF when caring for their baby, but as the baby begins to respond to them, they also experience CS. 23 Compassion fatigue, a significant concern among pediatric ward staff, arises from continuous exposure to patients’ suffering. Our research has identified several well-established risk factors that contribute to the development of CF in pediatric ward staff, which aligns with previous studies in the medical field. High workload, characterized by a constant influx of emotionally depleting cases, leads to heightened emotional fatigue.11,14 Excessive empathetic connection with patients’ pain can overwhelm pediatric ward staff and deplete their emotional resilience. Lack of support from coworkers or the organization can create feelings of loneliness, further increasing the impact of CF.14,15,17 Additionally, encounters with patients who have experienced traumatic events can result in secondhand traumatization, adding to the burden of CF.2,10 Individuals with unresolved personal trauma may also find their past experiences resurfacing in similar patient encounters, heightening their vulnerability. 2 Job dissatisfaction, often caused by factors like lack of recognition or excessive organization, significantly contributes to stress and emotional depletion. Neglecting self-care activities, such as exercise and hobbies, further depletes emotional and mental resources. Lastly, certain personality traits, particularly excessive selflessness, can cause healthcare professionals to prioritize others’ needs over their own, increasing their exposure to CF.10,18 These factors, often interconnected, highlight the urgent need for targeted interventions and organizational support to protect the well-being of pediatric ward staff and reduce the prevalence of CF in clinical settings. The consequences of CF and CS in pediatric wards underscore the importance of recognizing and addressing these emotional states among healthcare professionals. Interventions such as counseling, peer support programs, and self-care initiatives have been shown to mitigate the negative effects of CF and enhance CS, ultimately improving the overall well-being of healthcare providers and the quality of patient care in pediatric settings.
Despite the significant attention given to measuring the prevalence of CF in this group of workers, there is a lack of information and evidence about effective interventions designed to reduce CF in these occupational groups. We have found that, although there is recognition of the threat of CF to the mental health and well-being of at-risk occupational groups, and the existence of health programs to address CF and related concepts, rigorous academic evaluation of evidence on this topic has only recently emerged in the last few years. By consolidating the limited available evidence, we have identified promising interventions in this area, as well as evidence gaps and areas in need of further research. Implementing evidence-based workplace interventions has the potential to reduce CF and more serious, chronic, and economically costly mental disorders, benefiting individual staff, employers, and society as a whole by preserving healthy and productive workers who provide healthcare and social assistance to those in need.
This research has revealed several critical gaps in the existing literature. Firstly, there is an uneven global distribution of conducted studies, with a lack of precise information about this phenomenon in Africa and Asia. Additionally, there is an unequal gender distribution in all conducted research, with women participating significantly more than men. Detailed information about how men experience CF and CS remains elusive. Furthermore, there is a need for comprehensive investigations into the processes through which working hours and professional experience influence the onset of CF. Another important area that requires further examination in future research is the distinction between CF and burnout.
Implications
The findings of the present study have several practical implications. For instance, mental health professionals can use these insights to develop targeted interventions aimed at reducing compassion fatigue and enhancing compassion satisfaction among pediatric healthcare workers. Training programs focusing on stress management and resilience building could be particularly beneficial. Additionally, hospital administration can implement policies that promote a supportive work environment, such as regular health check-ins and peer support groups.
Based on the findings, some recommendations can be made for practitioners. First, regular training sessions on coping strategies and stress management should be implemented. Second, creating a supportive work culture that encourages open communication and peer support can help mitigate the effects of compassion fatigue. Lastly, providing access to mental health resources, such as counseling services, can support healthcare workers in managing their emotional well-being.
Limitation
While this review provides insights into compassion fatigue and satisfaction among pediatric ward staff, several limitations should be acknowledged. The first limitation is the inclusion of only English-language papers. This language restrictions may have led to the exclusion of relevant studies published in other languages, potentially including language bias. As a result, the findings may not fully represent the global research on compassion fatigue and satisfaction among pediatric ward staff. Future reviews should consider including studies in multiple languages to provide more comprehensive understanding of the topic. In addition, the included studies vary in terms of design, sample size, and measurement tools, which introduces heterogeneity. This variability can complicate the synthesis and comparison of the results across studies. Moreover, this study focuses specifically on compassion fatigue and satisfaction among pediatric ward staff, which may limit the generalizability of the findings to other healthcare setting or population.
Conclusion
The findings of this study demonstrate that numerous risk factors contribute to CF, including high workload, empathetic connections with patients, lack of organizational support, exposure to trauma, unresolved personal trauma, job dissatisfaction, neglecting self-care, and certain personality traits. It is crucial to address these interconnected factors through targeted interventions and organizational support to protect the well-being of healthcare providers in pediatric settings. Despite significant attention to CF prevalence, there is a critical gap in evidence-backed interventions. Academic scrutiny of CF interventions has recently emerged, highlighting the need for further research and the identification of promising interventions. There is an evident imbalance in global research distribution and gender participation, emphasizing the importance of comprehensive studies into men’s experiences and deeper investigations into the impact of work hours and professional experience on CF. Further exploration is needed to distinguish between CF, CS, and burnout. In conclusion, addressing these gaps through evidence-based interventions shows promise in reducing the impact of CF and cultivating a healthier, more resilient healthcare workforce for improved patient care and societal benefit.
Footnotes
Acknowledgements
Authors would like to thank colleagues who assisted in the coding process.
Author Contribution
All authors were involved in conceptualizing, data collection, data analysis and writing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.